To lay the foundation for prevention programs, a number of potential risk factors for eating disorders have been examined in cross-sectional and prospective studies. Most of these studies have involved predominantly or exclusively white study groups and—at least for the younger samples—have included a restricted set of measures—measures not validated for the targeted age range—and/or used diagnoses derived from paper-and-pencil measures.
Previous studies have also used different methods of defining risk. Kraemer et al.
(3) suggested a definition for risk that we employed for this study: “A risk factor is defined as a characteristic, experience or event that, if present, is associated with an increase in the probability (risk) of a particular outcome over the base rate of the outcome in the general (unexposed) population.” They set forth the following requirements for evaluating risk: 1) define the outcome clearly and completely and measure it validly; 2) define the population and sample it properly; 3) define the risk factor, establish that it defines a characteristic that occurs before the outcome, and measure it validly and reliably; 4) use analytic procedures that lead to definitions of high- and low-risk groups and establish that a statistically significant difference exists in the risks of these groups; and 5) use analytic procedures that lead to meaningful demonstrations of potency.
Results
Baseline Description
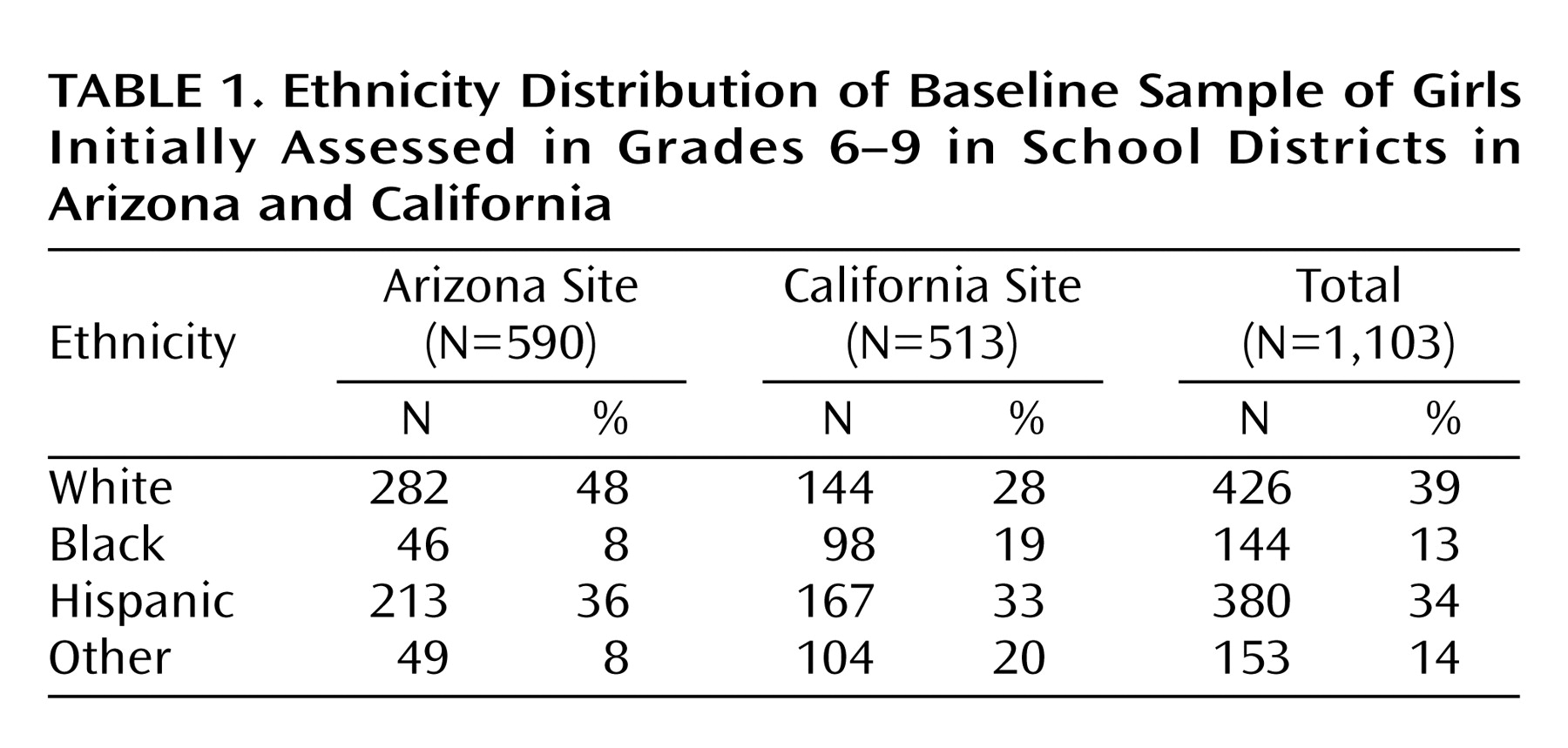
Of the 1,358 girls at baseline, 34 (2.5%) already had a full- or partial-syndrome eating disorder diagnoses and were omitted from this analysis. (Of these, five were diagnosed as having bulimia nervosa, 16 with partial-syndrome bulimia, eight with binge eating disorder, and five with partial-syndrome anorexia.) A total of 221 girls were assessed at baseline only and thus were not available for longitudinal analyses. The percentages of students available at 1, 2, and 3 years for follow-up for the Arizona and California sites, respectively, were 80%, 66%, and 60% and 79%, 69%, and 60%. The ethnic distribution by site for the remaining 1,103 girls can be seen in
Table 1.
There were no significant differences in dropout rates between girls from the two sites. Dropouts from the study were more likely to be African American (χ2=8.8, df=1, p<0.01), to use illegal substances (t=5.0, df=1310, p<0.001), to have more negative life events (t=3.8, df=1310, p<0.001), and to be less successful in school (χ2=22.7, df=3, p<0.001). There were no differences between the two groups on other measures.
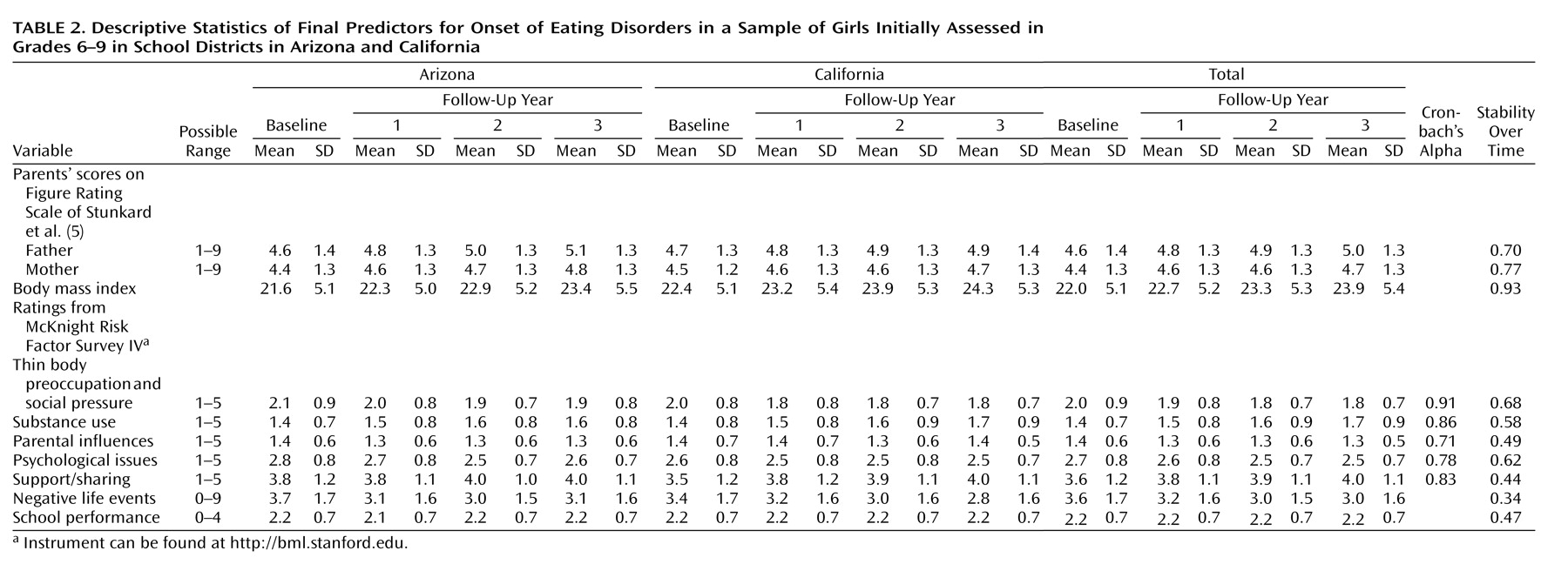
The baseline and follow-up scores for the predictor variables for the Arizona and California samples can be seen in
Table 2.
Stability of Baseline Measures
Table 2 shows the stability analysis for the variables measured across time. Five variables (body mass index, thin body preoccupation and social pressure, general psychological issues, and mother’s and father’s scores on the Figure Rating Scale) had stability scores >0.6. Therefore, the corresponding change variables were not included in the risk factor analysis.
Incidence of Eating Disorders
During the course of follow-up, 32 (2.9%) of the 1,103 girls developed a partial- or full-syndrome eating disorder and were classified as follows: one as having bulimia nervosa, 26 with partial-syndrome bulimia, and five with binge eating disorder. There were no new-onset cases of either anorexia nervosa or partial-syndrome anorexia. Nineteen of the new-onset cases were identified at the Arizona site and 13 at the California site.
Risk Factor Analysis
Because there was a significant site-by-Hispanic-ethnicity interaction (W=7.3, p<0.01) for survival, the two sites were analyzed separately.
Arizona site
In this sample, 19% (N=112) of 590 students developed eating disorders. Potential risk factors for the 19 new-onset cases were Hispanic ethnicity (W=6.5, p<0.01), thin body preoccupation and social pressure (W=17.4, p<0.0001), general psychological influences (W=9.8, p<0.01), and change in reported negative life events (W=9.1, p<0.01).
Thin body preoccupation and social pressure and general psychological influences occurred in the same time period and were examined in a pairwise analysis. These variables were significantly correlated (R=0.66, p<0.001) and, when entered into the model together, general psychological issues was no longer significantly related to time to onset, whereas thin body preoccupation and social pressure remained a significant predictor of time to onset (W=7.3, p<0.01). This result suggested that general psychological issues was a proxy for thin body preoccupation and social pressure and could be dropped from further risk factor analyses for this sample.
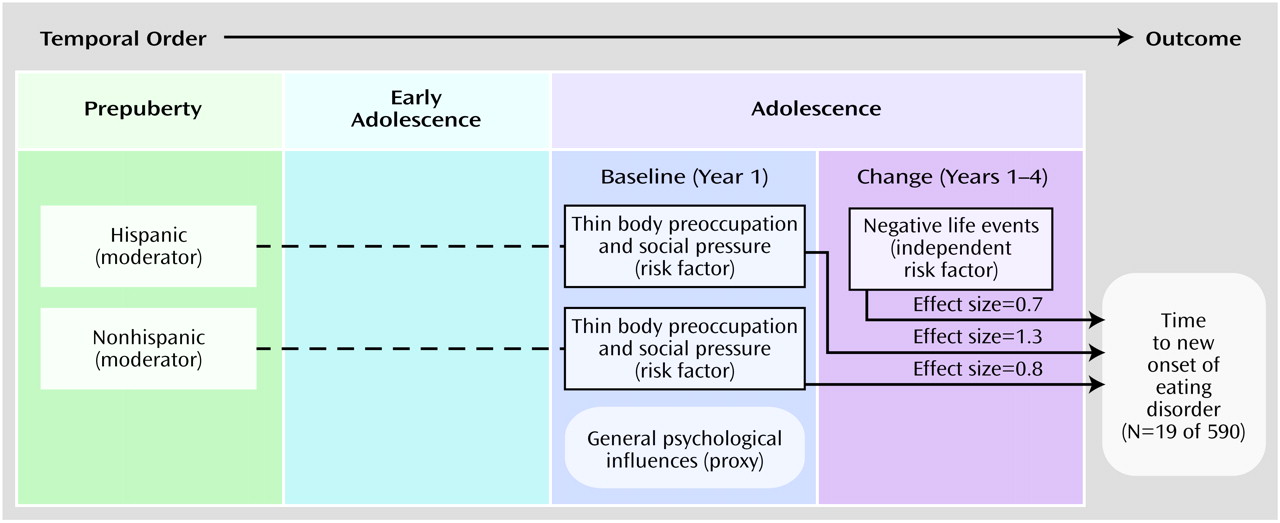
The remaining variables (being Hispanic, thin body preoccupation and social pressure, change in number of negative life events) were then examined in pairs on the basis of temporal sequence. Change in negative life events was found to be an independent risk factor, as it was not correlated with being Hispanic or thin body preoccupation and social pressure. Subjects with new onset showed an increase in negative life events (mean=0.39, SD=1.2), whereas noncases showed a decrease (mean=–0.25, SD=1.0; effect size for differences=0.65). There was a significant interaction effect between being Hispanic and thin body preoccupation and social pressure (W=9.7, p<0.01), indicating that being Hispanic moderates thin body preoccupation and social pressure. To further explore this issue, we looked at the mean scores for thin body preoccupation and social pressure in Hispanic cases and noncases: 68% of the subjects were Hispanic, whereas Hispanics were only 35% of the noncases. New-onset Hispanic subjects scored 3.2 (SD=0.9) on thin body preoccupation and social pressure compared to 2.1 (SD=0.8) for Hispanic noncases (effect size for differences=1.3). For non-Hispanics, new-onset subjects scored 2.7 (SD=0.5) compared to 2.1 (SD=0.9) for noncases (effect size=0.7). The final model can be seen in
Figure 1.
California site
The same analytic approach was used for the California data. In this sample, 13 of 513 students developed eating disorders. Only thin body preoccupation and social pressure (W=15.0, p<0.0001) was significantly related to outcome. New-onset subjects scored 3.0 (SD=0.7) compared to 1.9 (SD=0.8) for noncases (effect size for differences=1.2).
Risk Factor Screen
To determine which items from thin body preoccupation and social pressure might be used to screen for potential cases, all five domain scores for thin body preoccupation and social pressure and all questions for these domains were entered into a signal-detection analysis. Each domain and question score was treated as a test for illness and evaluated across a range of cutoff points to determine the variables that would produce an optimally efficient test.
The analysis identified three criteria derived from four questions (each question was scored 1–5): “How often have you been on a diet to lose weight?” (score of 4 or 5); “How often does your weight make boys not like you?” (score of 5); and the average of “How often do you change your eating around boys?” and “How often do you change your eating around girls?” (mean score ≥3.5). Answers above the cutoff for any of three criteria resulted in a screen sensitivity of 0.72, a specificity of 0.80, and an efficiency of 0.79. The predictive value of a positive test was 0.10 (of a base rate of cases of 2.9%), and the predictive value of a negative test was 0.99 (of a base rate of noncases of 97.1%). In this sample, the screen selected 242 students as being possibly at risk (21.9% of the total). Of these, 23 (10%) would become new cases.
Discussion
Higher scores on a factor (thin body preoccupation and social pressure) measuring concerns with weight, shape, and eating (including media modeling, social eating, dieting, and weight teasing) significantly predicted onset of eating disorders in young women in middle and high school. For instance, of those scoring in the upper quartile of this factor (mean >2.4), 8% developed new-onset eating disorders over the course of follow-up compared to 1.2% in the lower three quartiles. In the Arizona sample but not the California sample, thin body preoccupation and social pressure was moderated by ethnicity (Hispanic). An increase in negative life effects was also an independent risk factor in the Arizona sample. Our results also indicated factors that did not predict onset of eating disorders in multivariate analyses, including parental influences, social support, perfectionism/school performance, perceived parental weight, or having an early start of menstrual periods.
The finding that a factor reflecting high weight/shape and other concerns and issues (including dieting) predicts onset of eating disorders is consistent with other recent longitudinal studies in less diverse populations
(8,
9). The use of the principal components analysis combines domains (such as dieting and weight concerns) that, in univariate analyses, have been found to be important. An important next step in this area of research is to begin to examine the interactions among the components of thin body preoccupation and social pressure, developmental issues and methods of reducing weight/shape concerns, and dieting.
The finding that being Hispanic moderated the onset of eating disorders at the Arizona but not the California site raises an important issue. Smolak and Striegel-Moore
(10) argued that one of the reasons for the often inconsistent findings concerning ethnicity and eating problems is that ethnicity is actually a summary variable capturing diverse experiences and elements such as immigration status, gender roles, discrimination, socioeconomic disparities, and acculturation. The Hispanic girls in Arizona may have differed from those in California on one or more of these factors. For instance, the California girls had higher rates of non-English-speaking households (50% versus 35%, respectively) (χ
2=9.3, df=1, p<0.01) and were more likely to identify themselves as being Latin American (44%) compared to the Arizona girls (19% Latin American). Such factors need to be explicitly investigated in future research
(11,
12).
More puzzling, perhaps, is the failure to find any difference between African American girls and any of the other ethnic groups in terms of eating problems. Studies routinely find African American girls to be more satisfied with their bodies and to show fewer eating problems and disorders than white or Hispanic girls
(12). African Americans have lower rates of anorexia nervosa than do white populations, but there may be less of a difference in the disorders involving binge eating
(10,
11).
An increase in negative life events was also an independent (but relatively weak) risk factor for onset of illness in Arizona. This finding is consistent with work by Welch et al.
(13) and others who found stress to be a risk factor in retrospective analyses.
Although 86% of the sample was available for at least 1 year of follow-up, the relatively large dropout rate suggests that the results must be interpreted with caution.
At the Arizona site, general psychological issues was found to be a proxy for thin body preoccupation and social pressure. At the California site, the general psychological issues factor approached significance in predicting outcome in the univariate analysis (W=3.6, df=1, p=0.058). Many studies have found an association between eating disorders and various psychological factors, such as negative affect. Stice
(14) argued that eating disorders can develop through two pathways—by means of excessive dieting or negative affect. In our model, negative affect (as reflected by self-reported depression) is subsumed under general psychological influences as part of a proxy variable for weight/shape issues.
The power of our analysis was restricted by the low incidence of new cases. However, the incidence of new cases is similar to what has been reported in other populations. The incidence of partial- or full-syndrome eating disorders was 3.6%, which is similar to that reported by Lewinsohn et al.
(15) and Killen et al.
(9).
Of the new cases, most (81%) were of partial-syndrome bulimia nervosa. Only one of the new cases (3%) was of full-syndrome bulimia nervosa; the rest were of binge eating disorder (15%). Although partial-syndrome and full-syndrome eating disorders appear to exist on a continuum, new-onset full-syndrome cases are relatively rare in middle and high school students. We did not identify any new-onset cases of anorexia nervosa or partial-syndrome anorexia—a surprising finding since the peak age at onset of anorexia is during adolescence—but this is consistent with our previous studies
(8,
9). A study from Australia
(16) found an incidence of 0.5% of partial-syndrome anorexia and no anorexia nervosa in about 2,000 students followed for up to 2 years. Anorexia nervosa or partial-syndrome anorexia are also less prevalent in African American populations, which constituted 13% of our sample.
The stability data also provide a glimpse into the course of potential risk factors. The thin body preoccupation and social pressure factor was very stable throughout the course of the study. This suggests that the attitudes measured by this factor are formed earlier than was measured here.
Adding to the validity of the thin body preoccupation and social pressure risk factor, we compared the thin body preoccupation and social pressure at baseline for the 34 individuals who reported being ill compared to the students who did not have eating disorders. The mean thin body preoccupation and social pressure score was 2.1 (SD=0.9) and 1.9 (SD=0.8) at Arizona and California, respectively, for noncases compared to 2.8 (SD=1.1) and 3.3 (SD=1.0) for cases.
We also found that four questions could be used to identify 80% of the students who would become ill. The screen had moderate levels of sensitivity, specificity, and efficiency and could be used to help identify students at risk.