The etiology of complex disorders such as anorexia nervosa and bulimia nervosa is likely to involve a dynamic interplay of environmental and genetic factors. New approaches in genetic research provide an opportunity to study associations between a disorder and specific genes but face a well-recognized problem of phenotypic definition. It is likely that diagnostic categories as presented in the DSM-IV do not fully correspond to underlying biological factors.
One approach to specifying phenotypes is to use both axis I and axis II dimensions. The restricting subtype of anorexia nervosa is typically linked to personality traits such as perfectionism, sense of ineffectiveness, preoccupation with orderliness, and excessive persistence and compliance
(1–
7). Bulimia nervosa is often linked with impulsive personality traits
(8,
9), but the majority of people with bulimia nervosa are also found to be perfectionistic
(4). In a study of obsessive-compulsive disorder (OCD) symptoms in women with bulimia, 39% of the subjects with current bulimia or a history of bulimia were found to have obsessions related to symmetry and exactness
(10). Perfectionism and preoccupation with orderliness have been found to persist after recovery from eating disorders
(10–
13). Perfectionism in childhood is one of the risk factors for both anorexia and bulimia
(6,
14). In family studies, persons with a high level of perfectionism are overrepresented among healthy first-degree relatives of patients with eating disorders, suggesting that obsessive-compulsive personality disorder, or its traits, represent a heritable factor contributing to vulnerability for both types of eating disorders
(13,
15,
16).
The aim of this study was to determine whether retrospectively measured childhood personality traits reflecting obsessive-compulsive personality predicted development of eating disorders. To minimize biases related to retrospective reporting, the study used a newly developed interview instrument with items based on examples of childhood behavior. The study hypothesis was that childhood traits linked to obsessive-compulsive personality are important risk factors for the development of eating disorders. The subsidiary hypothesis was that people with an eating disorder who had a high number of childhood traits reflecting obsessive-compulsive personality have a higher prevalence of this type of personality disorder and have more compulsive symptoms later in life.
Method
Participants
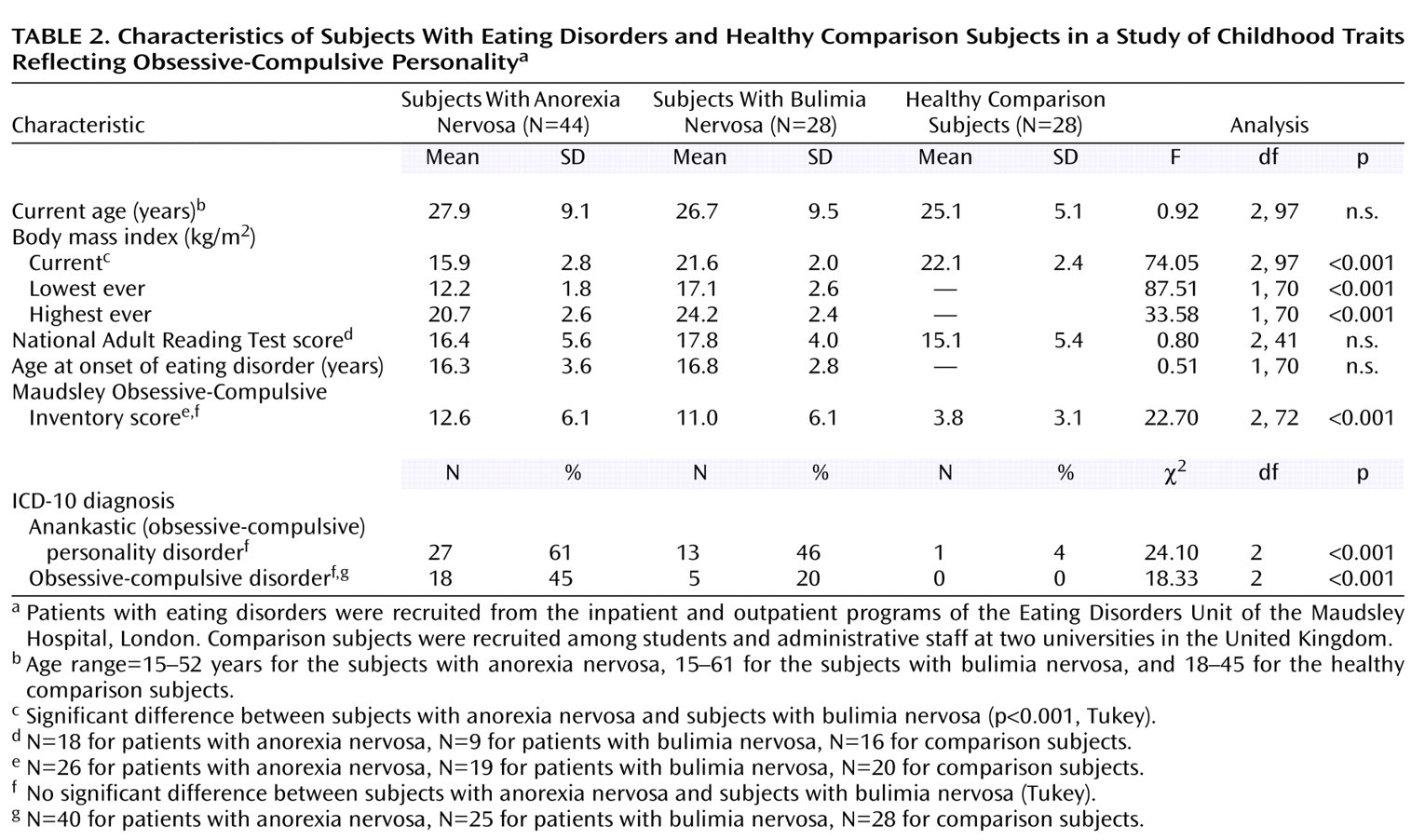
The participants consisted of three groups: 44 female patients with a DSM-IV diagnosis of anorexia nervosa (26 with the restricting type, 18 with the binge-eating/purging type), 28 female patients with a DSM-IV diagnosis of bulimia nervosa, and 28 healthy female comparison subjects. The clinical participants were recruited from the inpatient and outpatient programs of the Eating Disorders Unit of the Maudsley Hospital, London, a tertiary referral center. To avoid possible reporting biases related to an acute physical state, patients who fulfilled the diagnostic criteria and were willing to participate were entered in the study 3–4 weeks after the beginning of treatment. Exclusion criteria consisted of a history of psychotic disorder or bipolar disorder assessed according to the ICD-10 criteria. The comparison subjects were administrative staff and students from two universities in different towns in the United Kingdom. They were matched by age, sex, and educational level with the patients and were blind to the study hypothesis. The comparison subjects were of normal weight, had no personal or family history of an eating disorder or any other psychiatric disorder, and had no history of bingeing, vomiting, or abuse of laxatives. All subjects except those recruited as inpatients were reimbursed for their time. All participants were native English speakers. The study was approved by the South London and Maudsley National Health Service Trust and Institute of Psychiatry ethics committee. After complete description of the study to the subjects, written informed consent was obtained.
Procedure
Specialists in the Eating Disorders Unit who were blind to the study hypothesis made the initial screening diagnoses of eating disorders using the DSM-IV criteria. Study subjects were interviewed by a trained researcher (one of six postgraduate psychologists and psychiatrists) using a semistructured interview (described in the next section). On the day of the interview, data on demographic characteristics were collected, and the subject’s weight and height were measured. Thirty interviews were recorded on audiotapes and were rerated by one of two assessors who were blind both to the previous scoring and to the subject’s diagnosis.
Measures
The instruments used in the study included the semistructured EATATE interview and the self-report Maudsley Obsessive-Compulsive Inventory. The National Adult Reading Test was used to match patients and comparison subjects in intellectual ability.
The EATATE interview
The EATATE interview was developed for the European Healthy Eating Project, which examined genetic and environmental risk factors for eating disorders and obesity. (The instrument is available from the first author.) The first part, which consists of an adaptation of the Eating Disorder Examination
(17), is used to identify a lifetime eating disorder diagnosis in subjects and first-degree family members. The first part also is used to assess whether the subject meets the criteria for an ICD-10 lifetime diagnosis of OCD. Food and body-related obsessions are excluded as symptoms of OCD. The second part of the EATATE interview, which provided the data that are the focus of this paper, is used to assess whether the subject meets the criteria for current obsessive-compulsive personality disorder, according to the ICD-10 International Personality Disorder Examination
(18) module for anankastic personality disorder, and to collect data on childhood traits reflecting obsessive-compulsive personality. (An ICD-10 diagnosis of anankastic personality disorder corresponds to a DSM-IV diagnosis of obsessive-compulsive personality disorder).
The prototype of the assessment of childhood traits was developed in an expert meeting by collaborators on the European Healthy Eating project and other experts with extensive clinical and research experience in the field. After this session, the MEDLINE and PsycINFO databases (1965–2001) were searched for papers describing current and past personality traits linked with eating disorders. The key words used in the search were “personality,” “perfectionism,” “rigidity,” “inflexibility,” “obsessionality,” “anankastic,” and “childhood.” A focus group of patients with anorexia nervosa was held to identify behavioral examples of childhood traits reflecting obsessive-compulsive personality. The behavioral examples were used in designing the EATATE interview to minimize the problems associated with retrospective reporting and to reduce rationalization. The final instrument is used to assess five childhood traits that reflect obsessive-compulsive personality (
Table 1): perfectionism (e.g., Did you spend a long time doing or redoing your hair to make sure it was straight without bumps?), inflexibility (e.g., To what extent were you the sort of person who liked to make written plans/notes or have intricate details about the time ahead?), rule driven (e.g., Were you the kind of person who felt she always had to follow rules? For example, how far did you bend or break rules that were set by your parents or teachers?), drive-for-order and symmetry (e.g., While trying to get your room tidy and organized, were you particularly concerned about making sure that everything was “just so” and in its proper place?), and excessive doubt and cautiousness (e.g., Were your frightened to make a mistake as a child? Can you give an example?). The interviewer used a scoring manual to rate the responses according to predefined criteria. The interviewers were trained in the use of the manual by scoring videotaped interviews and by participating in consensus meetings where ratings were discussed. The presence of each trait was assessed together with its effect on the child’s life in terms of the child’s relationship with the world and with others. Traits were rated 0 for absent, 1 for present but not influencing the child’s life, or 2 for impinging on the child’s life or her relationship with the world or with others. Assessment of interrater reliability was based on the full 3-point scale. In all other analyses, the values 0 and 1 were not discriminated, and only traits that were reported to impinge on the child’s life (a rating of 2) were regarded as present. Any problems with the ratings were discussed at consensus meetings.
Maudsley Obsessive-Compulsive Inventory
The Maudsley Obsessive-Compulsive Inventory
(19) is a 30-item self-report scale that assesses four types of obsessive-compulsive complaints: checking, washing, doubting, and slowness. Alpha coefficients of 0.7, 0.8, 0.7, and 0.7 for the four subscales, respectively, were found. Good test-retest reliability has been reported for the instrument (Kendall’s tau=0.8)
(19).
The National Adult Reading Test
The National Adult Reading Test
(20) was used to match the participant groups in terms of approximate intellectual ability. The National Adult Reading Test requires the participant to read aloud 50 phonetically irregular words, and the number of mistakes is recorded. The test results have been found to correlate significantly with level of education
(20).
Analysis
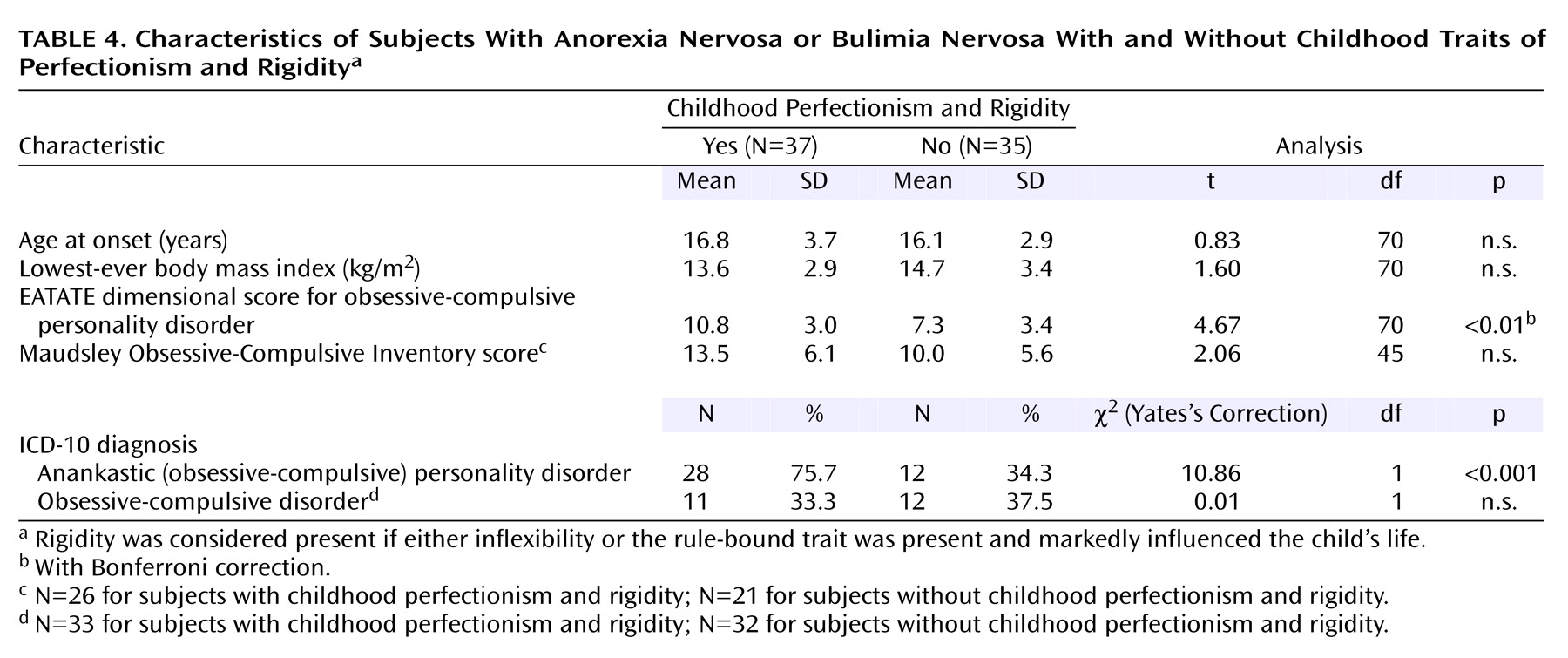
The clinical and demographic data were compared across groups by using chi-square tests and one-way analysis of variance, with the Tukey test for post hoc comparisons of group differences. Interrater reliability for the childhood trait scale of the EATATE interview was assessed with weighted kappa coefficients calculated for individual items (rated as 0–2) and an unweighted kappa coefficient for the diagnosis of obsessive-compulsive personality disorder. Cronbach’s alpha was calculated to measure the internal consistency of the childhood trait scale. Linear regression analysis was used to examine the relationship of childhood and adult obsessive-compulsive personality traits within the eating disorder and the comparison groups. Logistic regression was used to measure the association of childhood obsessive-compulsive personality traits with the presence of an eating disorder and obsessive-compulsive personality disorder later in life. T tests for independent samples (with Bonferroni corrections) and chi-square tests (with Yates’s corrections) were used to compare the subjects with eating disorders who did and did not report childhood perfectionism and rigidity. Two-tailed tests with a 5% level of significance were used throughout the analyses. No significant differences were found between the subjects with the restricting type of anorexia nervosa and those with the binge-eating/purging type. Thus, the data for those subgroups were analyzed together. All analysis were carried out by using SPSS-PC
(21).
Discussion
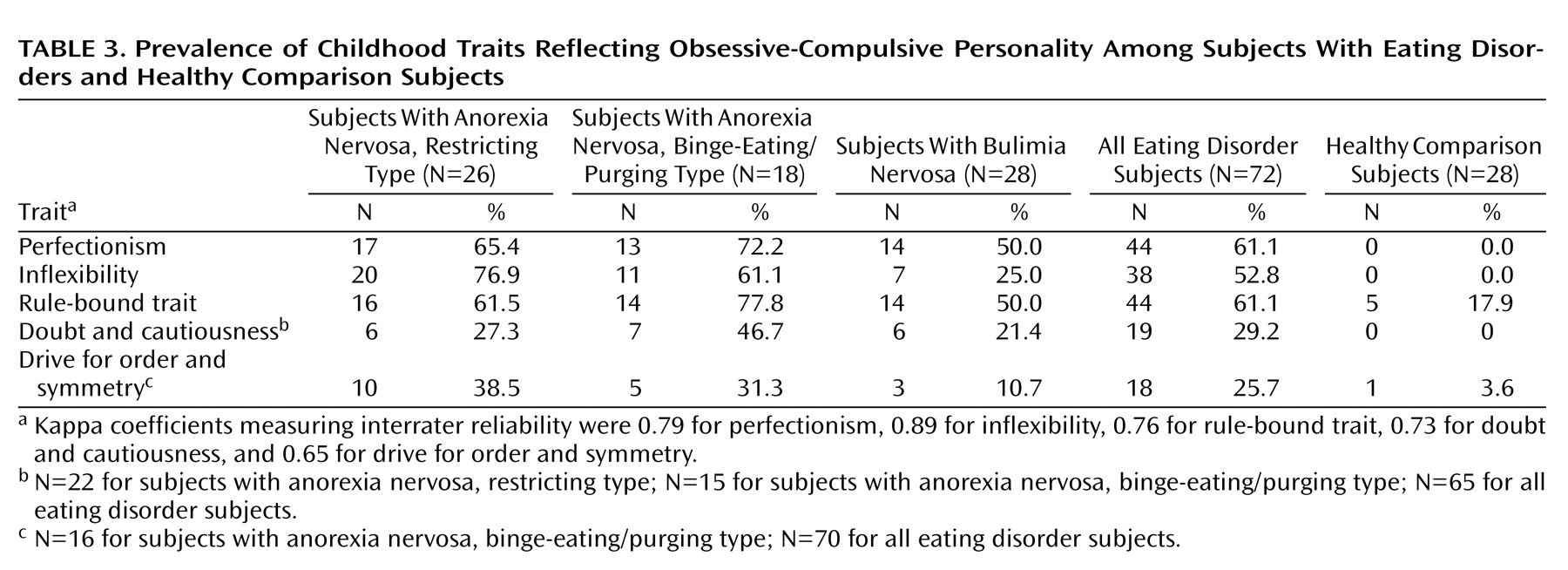
The results of this study confirm our hypothesis that women with eating disorders show high levels of obsessive-compulsive personality traits in childhood, relative to healthy comparison subjects. There was a strong increasing relationship between the number of reported childhood traits and the odds of developing an eating disorder, with each extra reported trait increasing the odds of developing an eating disorder nearly sevenfold. We also confirmed our subsidiary hypothesis of developmental continuity in that the presence of childhood perfectionism and rigidity identified a subgroup of people with eating disorders with a significantly higher prevalence of obsessive-compulsive personality disorder later in life.
Our results confirm and extend findings from previous studies. Fairburn et al.
(14) assessed perfectionism in childhood with a single item (high personal standards) and identified it as a risk factor for anorexia and bulimia in eating disorder patients, compared with healthy subjects (odds ratio=3.9, 95% CI=2.1–7.4, and odds ratio=2.6, 95% CI=1.5–4.6, respectively). The instrument we developed retrospectively examined a broader spectrum of obsessive-compulsive personality traits, including perfectionism, by using a range of behavioral examples.
Approximately two-thirds of the subjects with anorexia nervosa reported perfectionism and rigidity in childhood. This prevalence is consistent with that reported by Rastam
(22) for premorbid obsessive-compulsive (or anankastic) personality disorder in anorexia nervosa. We are not aware of any similar studies conducted for patients with bulimia nervosa. However, previous findings that perfectionism, obsessionality, excessive concern about mistakes, and doubt about actions persist after recovery from both disorders suggest that they represent persistent traits
(10,
13,
16).
The prevalence of comorbidity of anorexia and bulimia with OCD in this study was congruent with the published rates of 25%–69% in women with anorexia nervosa
(23–
25) and 25%–36% in women with bulimia nervosa
(8,
26).
The prevalence of cluster C personality disorders, which include obsessive-compulsive personality disorder, has been reported to range between 5% and 80% in people with anorexia nervosa
(4,
27–
29) and to be as high as 25% in people with bulimia nervosa
(8,
28). These figures are congruent with our findings.
This study had several limitations. The retrospective assessment was subject to inaccuracies of memory and subjectivity in reporting. Although the instrument used in this study was based on simple behavioral examples and used interviewer-based ratings (according to predefined criteria) to optimize the precision of the assessment, further studies with other informants or with a prospective design are needed to confirm the findings. It was impossible for the assessor to be blind to the primary diagnosis in assessing severely emaciated subjects with anorexia nervosa. This source of bias was minimized by rerating audiotaped interviews. Indeed, for the interviews that were audiotaped, we found a high level of agreement between the two raters, one of whom scored the taped interview and was blind to the subject’s appearance. The subjects with eating disorders were recruited from a tertiary referral center and were taking medication while participating in the study. Thus, their medication status may have influenced reporting accuracy.
The findings suggest that childhood obsessive-compulsive personality traits are important risk factors for later development of eating disorders, particularly anorexia nervosa. Furthermore, the findings suggest that childhood perfectionism and rigidity may offer a more specific and homogenous phenotypic determination for genetic studies. Further studies are needed to determine whether these traits are specific for eating disorders or are also linked to other psychiatric disorders, such as depression or OCD. Personality traits may also act as maintaining factors and as such may have an important influence on the prognosis of the disorder. Studies of people who have recovered from an eating disorder would be needed to explore the influence of childhood obsessive-compulsive-personality traits on the length of illness and its severity. Female subjects were included in this study because the prevalence of eating disorders is approximately nine times higher in women than in men. However, further studies that include male subjects are needed to better understand the role of the assessed traits. To our knowledge, the interview scale described here is the first to measure these personality trait risk factors in a broad and comprehensive way. The finding that perfectionism and rigidity represent strong risk factors suggests that these items might also be also used to identify people at high risk for developing an eating disorder later in life. Prospective studies are needed to replicate these findings.