Mr. A, a 34-year-old man, came to our outpatient clinic for treatment of a major depressive episode. His history was also notable for polysubstance abuse and dependence in sustained remission, with prior abuse of alcohol, LSD, and other hallucinogens and prior dependence on marijuana, cocaine, opiates, and Ecstasy (MDMA [3,4-methylenedioxymethamphetamine]). He began using alcohol at age 9, marijuana at age 12, cocaine at age 13, opiates at age 20, and Ecstasy at age 21. He had a history of depressive symptoms 6 years earlier in the context of active substance dependence and chronic back pain but had no other prior psychiatric diagnosis or treatment. One year before presentation to our clinic, he had been smoking cocaine daily, using Ecstasy several days a week, and consuming two to 10 alcoholic drinks daily but reported no depressive symptoms. After consuming cocaine, Ecstasy, oxycodone, and methadone at a party, he became aggressive and was brought to an emergency room. There, he ingested all of his remaining methadone to prevent it from being discovered. He reported no suicidal intentions surrounding this ingestion. He became unresponsive, hypoxic, and hypotensive. Mr. A was resuscitated and then stabilized in an intensive care unit over 4 days.
After this overdose, Mr. A became acutely depressed. He endorsed a depressed mood, anhedonia, low energy, difficulties concentrating and remembering, feelings of hopelessness and guilt, poor self-esteem, social isolation, increased sleep, and a 20-lb weight gain over the ensuing year. He reported the disappearance of drug cravings and remained abstinent from all recreational drugs other than an occasional glass of wine with dinner. He reported that he no longer experienced pleasure from drinking alcohol. Four serial urine toxicology screens were negative over 6 months.
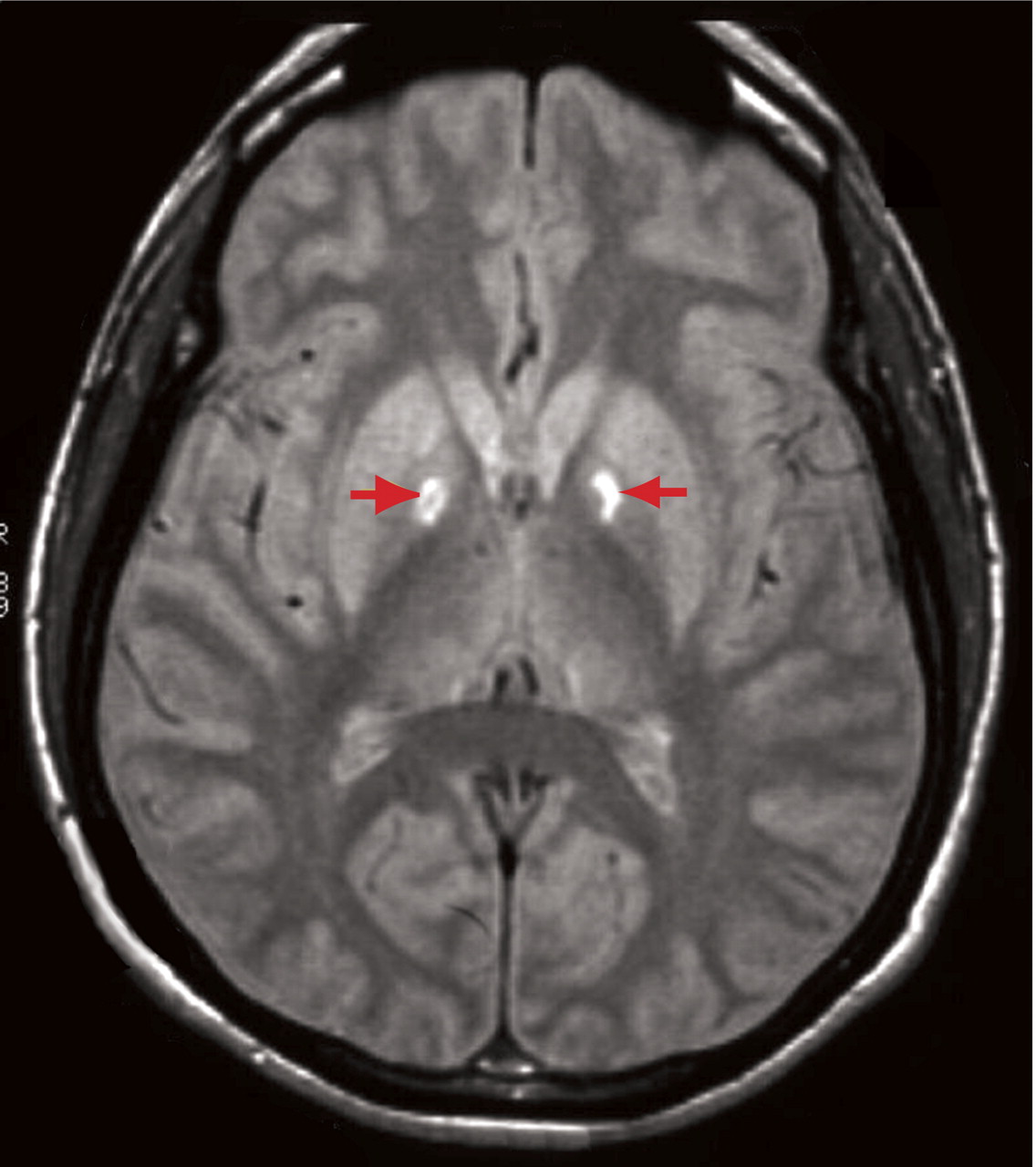
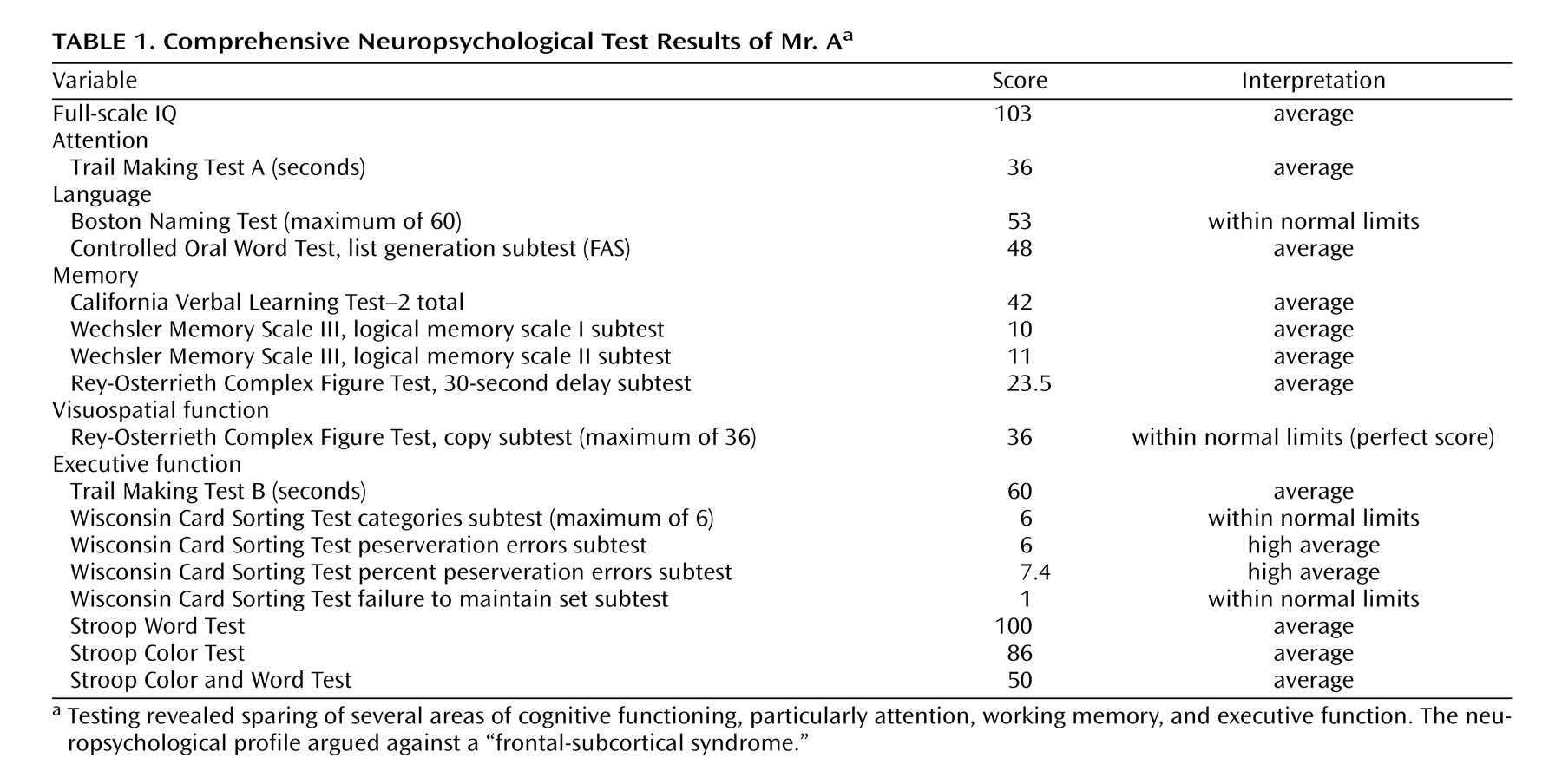
Mr. A developed a resting tremor of his left hand, slight rigidity of his right arm and left leg, and slowing of rapid alternating movements of his left hand, all of which were still present 16 months after the overdose, as assessed by a movement disorders specialist. He had no prior history of neurological problems. A magnetic resonance imaging (MRI) scan of his brain revealed a selective bilateral lesion of the globus pallidus ( Figure 1 ), with clear involvement of the internal globus pallidus on the right and both internal and external globus pallidus on the left. The bilateral lesion was small, selective, and restricted to the globus pallidus. There were no other lesions or findings on the MRI. Comprehensive neuropsychological tests revealed intact cognitive functions, including attention, working memory, and executive function, and an indicated absence of a frontal-subcortical syndrome ( Table 1 ).
Figure 1. An Axial Proton Density Magnetic Resonance Imaging Scan of Mr. A at the Level of the Basal Ganglia, Demonstrating Signal Hyperintensities in the Globus Pallidus Bilaterally a
a See arrows.
Basic blood tests, including a CBC, a basic metabolic panel, liver function tests, and thyroid function tests, were all within normal limits at the time Mr. A came to our clinic. There was no known family history of affective disorders or substance abuse.
Discussion
In summary, we describe the case of a 34-year-old man with a history of polysubstance abuse and one prior episode of depressive symptoms who developed a severe depressive episode, a loss of drug cravings, a diminished pleasurable response to alcohol, and extrapyramidal motor symptoms after a hypoxic episode. Testing was notable for bilateral lesions of the globus pallidus on his MRI and intact cognitive functioning on extensive neuropsychological tests.
The globus pallidus is a “watershed area” that is highly sensitive to hypoxic damage (1) . Cerebrovascular ischemic damage (stroke) of the globus pallidus after hypoxemia secondary to opiate overdose has been described (2) . Although depression is common after a stroke, poststroke depression has been most highly correlated with lesions of the globus pallidus (3) .
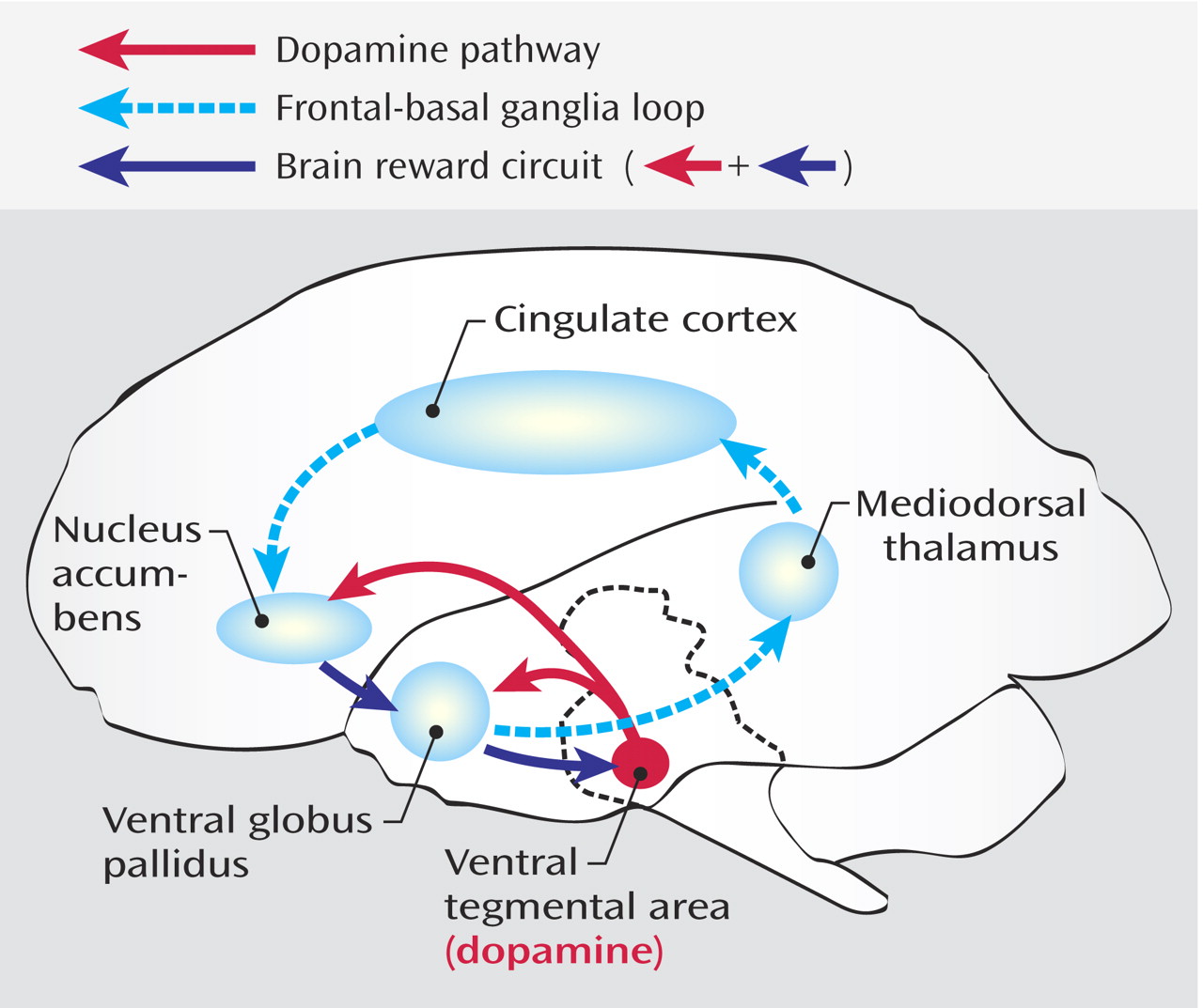
The clinical presentation of anhedonia in response to drugs, as well as to naturally occurring pleasurable stimuli, is consistent with the involvement of the globus pallidus in reward. The brain reward circuit ( Figure 2 ; see also references 4–8) includes the ventral tegmental area, which projects dopaminergic fibers to the nucleus accumbens as well as to the globus pallidus (6) . The nucleus accumbens projects fibers to the ventral globus pallidus, which, in turn, projects to the ventral tegmental area (4, 6, 8) .
Figure 2. The Brain Reward Circuit a
a Dopaminergic neurons project from the ventral tegmental area to the nucleus accumbens and the ventral globus pallidus. Neurons from the nucleus accumbens project to the ventral globus pallidus, which, in turn, projects to the ventral tegmental area. In addition, the ventral globus pallidus gains access to the prefrontal cortex through projections to the mediodorsal thalamus, which projects to the anterior cingulate.
The defining characteristic of this circuit is its ability to sustain brain stimulation reward (9) . That is, laboratory animals can be easily trained to perform an operant response (e.g., lever pressing) that results in delivery of rewarding electrical stimulations through an electrode implanted into any site of the brain reward circuit. Indeed, rats will perform electrical self-stimulation of the ventral globus pallidus at a high rate.
Presentation of rewards and stimuli predictive of future rewards trigger the firing of ventral globus pallidus neurons (10) . Blockade of the ventral globus pallidus has been shown to impair intravenous drug self-administration in laboratory animals (11) as well as to impair relapse to drug- and stress-triggered drug-seeking behavior (12, 13) . These findings are consistent with the patient’s loss of drug cravings and alcohol-induced euphoria. In animal studies, disruption of the ventral globus pallidus interferes with partner bonding and partner preference (14) . The patient’s social isolation and diminished pleasure in social situations may have been related to impaired encoding of social rewards through the globus pallidus. Finally, lesion of the dorsal portion of the globus pallidus, which is involved with motor behavior through extrapyramidal motor circuits (15), is consistent with the patient’s tremor, rigidity, and bradykinesia.
In conclusion, this case suggests an association between bilateral lesions of the globus pallidus and a syndrome of anhedonia, loss of drug cravings, and extrapyramidal signs that are consistent with the participation of this brain structure in both reward circuitry and movement. We describe a clinical correlation between damage of the globus pallidus and diminished rewarding effects of drugs of abuse, which has been previously observed in animal models. Cases such as this may occur with increased frequency in the future, given the significant increase in emergency room visits related to heroin use and narcotic analgesics from 1995 to 2002 (35% and 163%, respectively) (16) and the fivefold increase in the purity of street heroin from 1981 to 2000 (17) . Indeed, 48% of heroin users report a history of at least one nonfatal overdose (18) . We hope that this individual case may lead to future controlled studies in both animals and humans to further elucidate the role of the globus pallidus.
Footnote
Received Dec. 2, 2005; revision received Feb. 16, 2006; accepted Feb. 16, 2006. From the New York State Psychiatric Institute, Department of Psychiatry, and the Department of Neurology, Columbia University. Address correspondence and reprint requests to Dr. Vorel, Department of Psychiatry, Columbia University, 1051 Riverside Dr. #99, New York, NY 10032; [email protected] (e-mail).The authors thank Dr. Alexander Glassman, Dr. Ronald Rieder, and members of the Division of Substance Abuse, Department of Psychiatry, Columbia University, for their suggestions; and Ms. Eve Vagg for graphic production.Drs. Miller and Vorel made an equal contribution to this work.
References
1.
Janavs JL, And M, Aminoff J: Dystonia and chorea in acquired systemic disorders. J Neurol Neurosurg Psychiatry 1998; 65:436–445
Vila N, And M: Chamorro, ballistic movements due to ischemic infarcts after intravenous heroin overdose: report of two cases. Clin Neurol Neurosurg 1997; 99:259–262
Robledo P, Koob GF: Two discrete nucleus accumbens projection areas differentially mediate cocaine self-administration in the rat. Behav Brain Res 1993; 55:159–166
Emergency Department Trends From the Drug Abuse Warning Network, Final Estimates 1995–2002. Rockville, Md, Department of Health and Human Services, 2003
McGregor C, Darke S, Ali R, Christie P: Experience of non-fatal overdose among heroin users in Adelaide, Australia: circumstances and risk perceptions. Addiction 1998; 93:701–711
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.