Effects of season of birth have been documented in several neuropsychiatric disorders and are important to clarify because they may indicate such possible etiologies as viral infection, perinatal hazard, immunological response, ambient temperature, or diet
(1) . In autism, studies of season of birth date back to Bartlik
(2), who first reported higher rates of births of autistic children in March and August. The next studies, however, had conflicting findings. Several studies have demonstrated evidence of peaks of birth rates of autistic children in March
(2 –
6) and August
(2,
3), and one study found a peak in October
(7) . Other studies have shown no evidence for peaks in individual months but instead found seasonal trends, with winter
(7) and spring
(8) demonstrating significantly higher rates of autistic births. However, most studies do not agree on the definitions of these seasons, and the significance of the finding may depend on whether December, for example, is assigned to winter
(7) or fall
(9) . Finally, several studies have suggested that there is no evidence for seasonal
(4,
5) or monthly trends
(5,
10) in the birth rates of autistic children.
In addition to being inconsistent in their findings, previous studies of season of birth in autism also had some methodological limitations. First, most studies used clinical, rather than epidemiological samples
(2 –
6,
8 –10) . Second, comparison groups varied between studies in which live births
(2 –
9), siblings
(5,
7), or children with other developmental disabilities
(10) were used. Third, different diagnostic definitions for autism were employed within and across studies. Finally, criticism of the statistical methods applied in these studies have also been raised, specifically that it is only through multiple subanalyses that significant findings emerge
(4 –
7) .
In the present investigation, we used data on almost all live births of Israeli-born Jews during 5 consecutive years to address the relation of month and season of birth and autistic spectrum disorders. These data include information on autistic spectrum disorders and the month of birth collected during mandatory military induction assessments at adolescence. Based on our literature review, we hypothesized that risk for autistic spectrum disorders would be associated with season of birth and would specifically increase in March and August.
Method
The subjects were 311,169 Jews born in Israel over 5 consecutive years in the early 1980s and assessed by the Israeli Draft Board at age 17. After receiving approval for the study from the local Human Subjects Committee, a unidentified data file was created by the managers of the draft board database. The draft board population includes all individuals eligible for military service in addition to those who would be exempted owing to medical, psychiatric, or other reasons. Comparison to the Israeli Jewish birth cohort for the corresponding years (using data provided by the Israeli Bureau of Statistics) indicated that over 98% of the men in the birth cohort who were alive after the first year of life appeared in the draft board registry. The proportion for women was lower, mostly because orthodox women are exempted from military induction. Two hundred and eleven subjects were ascertained to have autistic spectrum disorders, corresponding to a prevalence of 0.00068% (6.8:10,000), consistent with most epidemiological studies during the same time as our study
(11) .
Diagnoses in the draft board registry are based on ICD-10. The medical status of individuals with developmental disabilities is reported annually to the draft board by government agencies and other organizations responsible for the care and protection of these individuals. For individuals with autistic spectrum disorders, the responsible agency is the Israeli Society for Autistic Children. All persons suffering from autistic spectrum disorders and originally diagnosed and followed during childhood or adolescence are registered with this organization.
Relative risks and 95% confidence intervals were obtained by fitting Poisson regression models that predicted the frequency of autistic spectrum disorders according to the month of birth. A subsequent model adjusted for potential confounders with control for the year of birth and socioeconomic status. Socioeconomic status was based on paternal years of education also available from the draft board. Analyses were then repeated using previously proposed
(7) month categorizations for seasons; p values were calculated with the likelihood-ratio chi-square statistic. The significance level was set at 0.05, and all tests were two-tailed. Power analyses for tests of monthly or seasonal differences suggested that the study cohort had the power above 90% to detect a relative risk of 2.
Results
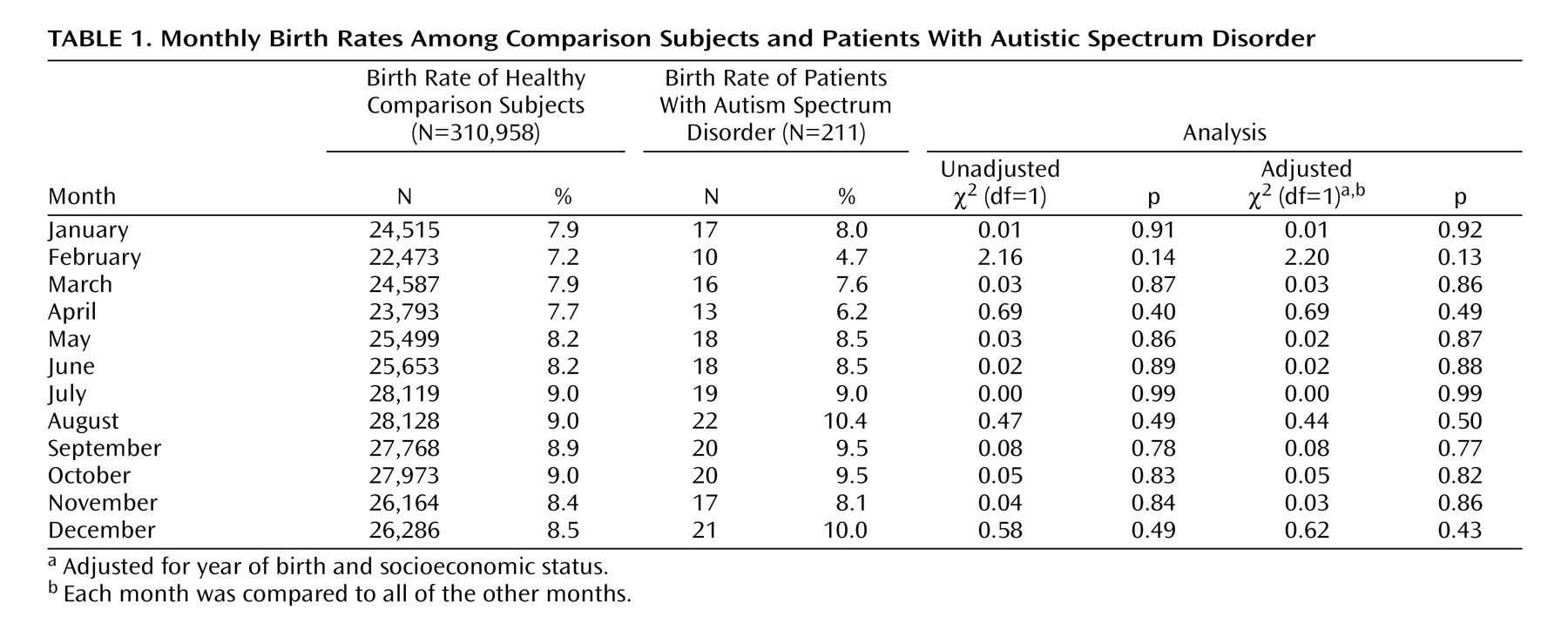
Table 1 presents the months of birth and rates of autistic spectrum disorders. We found no overall association between the two (χ
2 =3.91, df=11, p=0.97). Similar results were obtained after we adjusted for potential confounders. Stratifying the analysis by gender did not modify the findings. Excluding cohort members without autistic spectrum disorders who received any psychiatric diagnosis other than autistic spectrum disorders by the draft board did not affect the results (χ
2 =3.86, df=11, p=0.97). Specific examination of March and August births found no association with the risk of autistic spectrum disorders. Finally, the effect of season on the rates of autistic spectrum disorders, likewise, did not reveal any association (data not shown).
Discussion
In a historical population-based cohort study, we found no relationship between month or season of birth and the prevalence of autistic spectrum disorders at age 17. These findings are similar to those of two studies reporting no effect of month or season of birth in autism
(5,
10) . Of interest, a previous study
(3), also performed in Israel, did show a significant increase in autism in individuals born during March and August. However, the authors used a combination of older diagnostic criteria for autism, and the study was likely to have underascertained cases.
This study is unique in that it is based on data from the complete nationwide Jewish population. Thus, virtually all subjects with autistic spectrum disorders were included in the cohort. Another strength of the present study is that diagnoses are assigned at the time of draft board assessment and were based on ICD-10 criteria. They were not based solely on the original diagnosis of the individual in childhood but rather on the individual’s history to date. Individuals with autistic spectrum disorders are receiving services and treatments from numerous well-trained clinicians who have followed them over a long period of time. Therefore, by the time information is sent to the draft board (at age 17), it is likely that most of these patients have been well diagnosed and are likely to truly meet ICD-10 diagnostic criteria. This precludes any effects of the incidence of age from influencing the findings and decreases the possibility of overdispersion, both suggested as potential confounders in previous studies
(7) .
A limitation of the present study is that draft board diagnosis did not distinguish between patients with autism and those with autistic spectrum disorders. However, subjects in the present cohort were diagnosed and followed at times when the diagnosis of autism was relatively narrow and uncommon and the diagnosis of an autism spectrum disorder, such as Asperger’s syndrome, was very rare
(11) . Therefore, it is reasonable to assume that subjects with autism considerably outnumbered those with autistic spectrum disorders in the study cohort. Records from the Israel Society for Autistic Children of individuals registered in the same years as our cohort support such a conclusion.
In light of the present and other recent findings, it would seem logical that future attempts to identify an association between birth months and risk for autistic spectrum disorders should be exercised with caution. The combined evidence suggests the absence of any season of birth effect in autism.