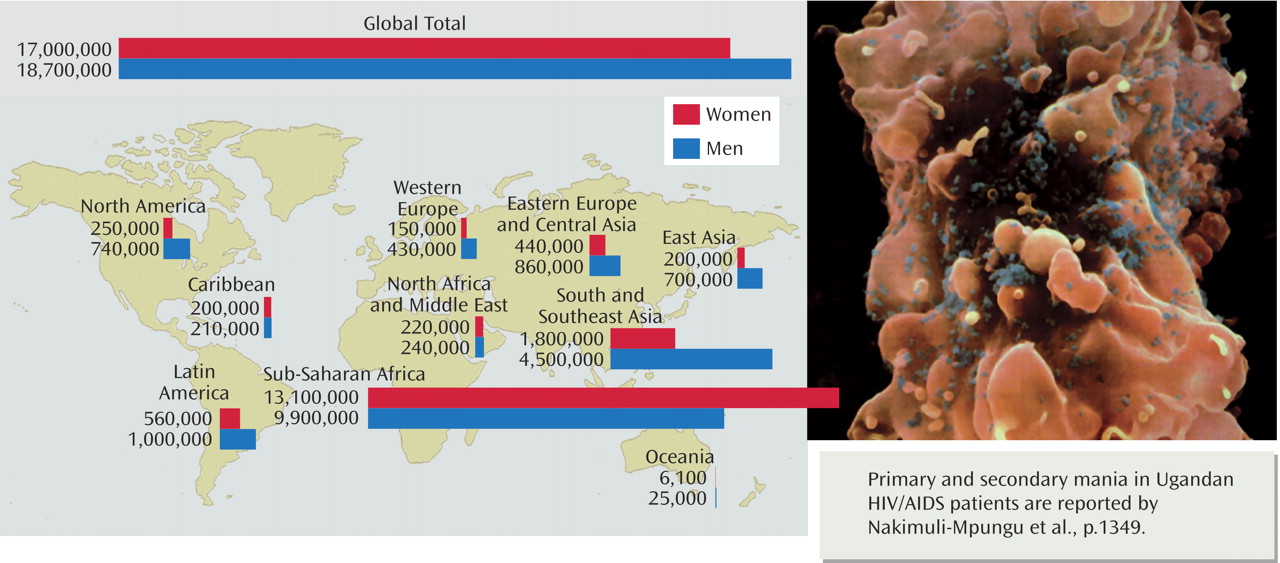
HIV is a retrovirus that has caused the worst worldwide epidemic in recent medical history, as the above
World Health Organization statistics show. HIV was first identified in 1981 as a syndrome associated with reductions in DE4+ T cells. In 1984, evidence first became convincing that HIV caused acquired immunodeficiency syndrome (AIDS). Soon, azidothymidine (AZT) was demonstrated to be a partial treatment, molecular characteristics of the illness were defined, and the role of the CD4 receptor was discovered. The HIV infection begins locally and spreads to distant sites by infected blood elements, predominantly the CD4+ T cells. In addition, HIV infects macrophages, often not killing them but activating them to release interferon-alpha, other inflammatory cytokines, and TGF-alpha, all probably of symptomatic significance. HIV is a persistently infecting virus and therefore does not rapidly kill off its target cells. Once the HIV protein (gp120) binds to the CD4 molecule on the T cell, subsequent binding to its coreceptors, CXCR cytokines, occurs and facilitates infection. Disease progression is based on many factors, including the type of HIV, innate host immunity, anti-HIV suppressor factor, coreceptor expression, and the magnitude of the immune response; both genetic and environmental factors play a role. Moreover, while HIV is not a tumor virus (i.e., infected cells do not become neoplastic), HIV infection fosters neoplastic transformation of some uninfected cells; HIV could be called a potent cocarcinogen. HIV enters the brain early after infection but is rarely symptomatic until systemic immunosuppression develops, when motor, cognitive, and behavioral changes can occur. An HIV-mediated primary brain infection occurs in 20%–25% of all HIV-infected individuals. Brain lesions include stroke, demyelinating illnesses, dementias, peripheral neuropathies, and, most commonly, cognitive alterations. Brain pathology includes infected macrophages and activated astrocytes, but no neuronal infection. Infected macrophages release potent toxins like viral gene products (tat and gp120) and proinflammatory cytokines; neuronal injury can occur directly (by interaction with viral proteins) or indirectly (through the inflammatory reaction products of the blood cells and astrocytes). Current treatments consist of a cocktail of at least three different small molecule inhibitors of more than one of the HIV enzymes, specifically of the reverse transcriptase and of the HIV protease; the mixture is called “highly active antiretroviral therapy” (HAART). At present, despite broad promise, the HIV virus has not been eradicated. Toxicity is common, and resistance occurs, such that 50% of infected patients fail therapy in less than 2 years. While treatment issues are manageable in industrialized nations, complex problems exist in developing countries, predominantly around treatment costs and practical drug delivery systems.