According to DSM-IV, subjects with hypochondriasis suffer from the fear or idea that they are seriously ill. They attribute benign physical symptoms to a serious disease, despite adequate medical reassurance to the contrary
(1) . The estimated prevalence of hypochondriasis in primary care ranges according to DSM-III-R criteria from 4.2%–8.5%
(2,
3) . The disorder is associated with marked impairments in physical and psychological functioning, work performance, and increased health care utilization. In addition, psychiatric and functional somatic syndromes are diagnosed more frequently in hypochondriacal subjects than in healthy comparison subjects
(3) .
Although hypochondriasis has a reputation for being chronic and relatively refractory to treatment, several controlled studies have demonstrated the efficacy of cognitive behavior therapy (CBT) for the condition
(4 –
7) . The literature on the pharmacological treatment of hypochondriasis, however, is scarce and ambiguous. Data obtained by means of open-label trials
(8 –
10) suggest that selective serotonin reuptake inhibitors (SSRIs) are effective. To date, only the preliminary results of a small cohort placebo-controlled trial have been reported. These results suggest somewhat higher response rates to fluoxetine than to a placebo
(10,
11) . However, research in this field has yet to include randomized controlled trials comparing the efficacy of CBT and pharmacological treatment.
To compensate for this gap in information, we compared the short-term treatment effect of open-labeled CBT with paroxetine and a placebo in a 16-week, multicenter randomized trial. Paroxetine and placebo were administered in a double-blind fashion.
We hypothesized that CBT and paroxetine would be more effective than the placebo and that they would not differ significantly from each other in efficacy.
Method
Participants
We included subjects from age 18 who met DSM-IV criteria for hypochondriasis
(1) . Diagnosis and treatment took place at three psychiatric outpatient clinics in the western region of the Netherlands. Excluded were subjects with comorbid psychotic disorders, substance use disorders, and organic mental disorders. Pregnant and lactating women and subjects with severe medical illnesses were also excluded. Concomitant use of antidepressants, mood stabilizers, antipsychotics, and anticoagulants, an allergy for SSRIs, and being in psychotherapy for hypochondriasis elsewhere were also exclusion criteria.
Individuals with hypochondriasis suffering from a comorbid mood disorder, anxiety disorder, and other somatoform disorders were included only when they indicated hypochondriasis to be the psychiatric disorder they suffered the most. Concomitant use of benzodiazepines was permitted to a maximum of the equivalent of 30 mg oxazepam, but only if subjects had been taking benzodiazepines for more than 3 months and were willing to keep use at a constant dosage for the duration of the trial.
This study received ethical approval from the participating medical centers and was conducted between Jan. 1998 and July 2002.
Study Design
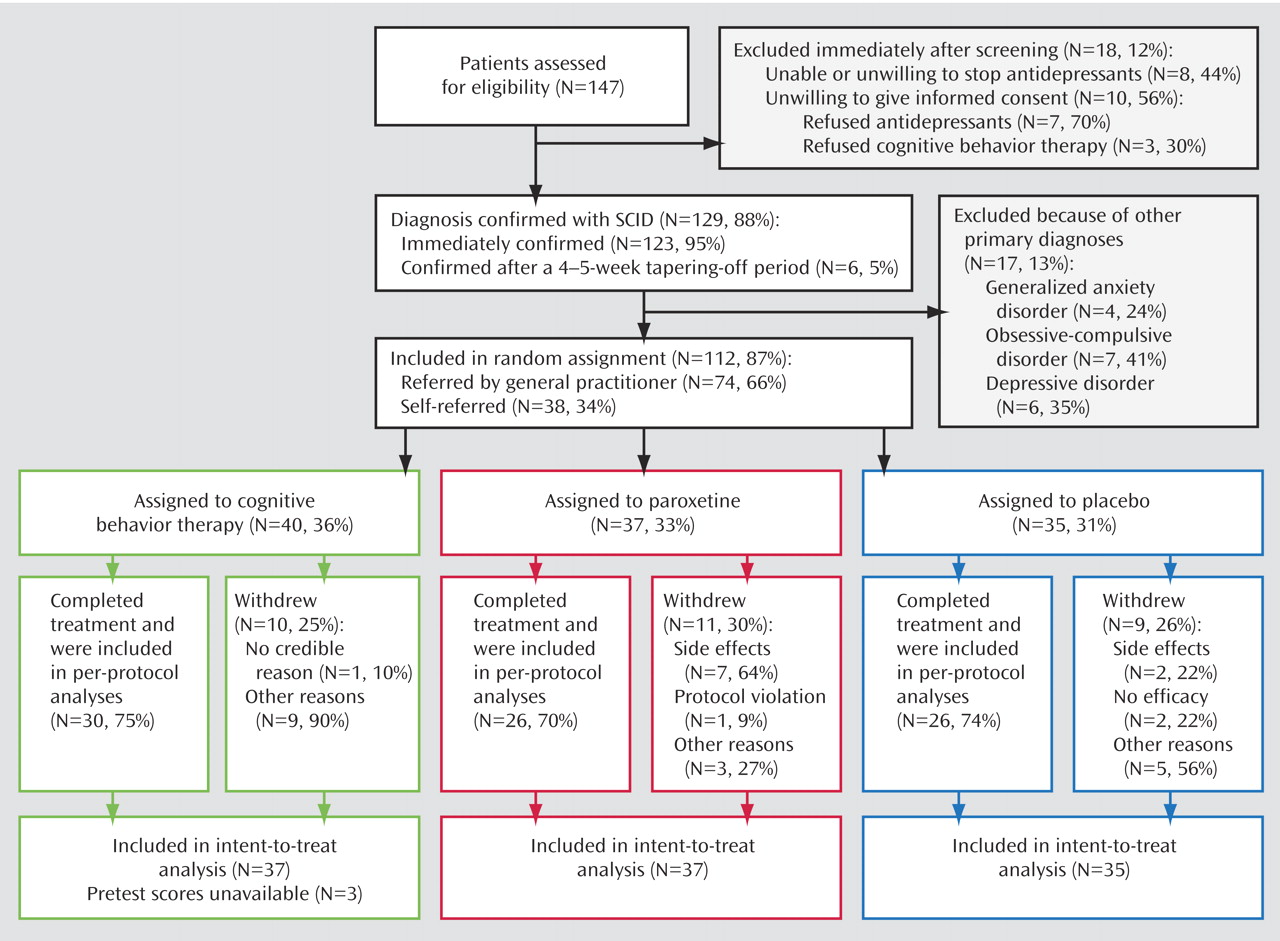
Subjects were assessed for eligibility for the trial by means of an intake session with an experienced psychiatrist who did a psychiatric assessment. In case subjects did not use antipsychotics, mood stabilizers, and antidepressants at the time of the intake session, the diagnosis was immediately confirmed by means of the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID)
(12), and written informed consent was obtained. Those who used these drugs and were willing and/or able to stop taking them, started tapering-off supervised by the intake psychiatrist. When subjects remained drug-free for 4 weeks (5 weeks for fluoxetine), the diagnosis was confirmed and written informed consent was obtained (
Figure 1 ).
The participating subjects were randomly assigned by site to receive CBT, paroxetine, or a placebo (1:1:1). The randomization code was developed by a statistician not involved in this study. Random permuted blocks with a length of six were selected, and the details of the series were unknown to any of the researchers. The subject numbers were put in sequentially numbered, opaque, sealed envelopes by the independent statistician, bearing only a number on the outside. When a subject was included, the envelope with the appropriate number was opened. The card inside indicated the group to which the subject was assigned.
In the placebo and paroxetine groups, the subjects, psychiatrists, and researchers remained blinded throughout the entire duration of the study.
Medication was prescribed by five experienced psychiatrists. Subjects started with a daily dosage of 10 mg of paroxetine in the first week. During the second week, the dose was increased to 20 mg per day. Following that, the dose increased weekly in increments of 20 mg per day to a maximum dosage of 60 mg per day
(9) . Where subjects began suffering from intolerable side effects, the daily dose was decreased to 40 mg or to 20 mg. During the 16-week treatment period, the subjects were scheduled for 12 medication-control visits lasting 20 minutes each. The psychiatrists were not allowed to resort to any formal psychotherapeutic intervention. In addition, they were required to use a written manual to record the perceived effect of the medication, the prescribed dose, adverse events (scored on the Fawcett side effect scale
[13] ), concomitant illnesses, and concomitant medication, including benzodiazepine use, between the visits. Paroxetine blood samples were taken in week 16 to verify subject compliance. Subjects who received paroxetine had a mean plasma level of 69.56 μg/liter (SD=41.12 μg/liter). Paroxetine was detected in all subjects in the paroxetine group, whereas no paroxetine was found in the blood samples of subjects receiving the placebo.
CBT was based on the treatment protocol used by Visser and Bouman
(6) . The treatment consisted of anywhere from six to 16 individual sessions, depending on the speed of recovery. For the intent-to-treat cohort, the average number of sessions was 7.3 (SD=4.7), while treatment completers attended their therapist 10 times. Treatment was administered by 10 behavioral therapists who were trained to use the treatment protocol and were supervised by senior cognitive behavioral therapists (Drs. Visser and van Rood) during treatment provision. To monitor treatment progress and the psychotherapists’ treatment integrity, all sessions were audiotaped. CBT consisted of the following components: identification of dysfunctional automatic thoughts and basic assumptions, verbal challenge of the tenability of the hypochondriacal automatic thoughts and basic assumptions, formulation of realistic or more functional beliefs, formulation of behavioral experiments to test the credibility of automatic versus alternative cognitions, exposure and response prevention, homework assignments, and relapse prevention.
Outcome Measures
Measurements took place at pretest (week 0) and posttest (week 16). We used the 4-point Likert scale version of the Whiteley Index as the primary outcome measure. The Whiteley Index is a 14-item self-report questionnaire designed to assess the core features of hypochondriasis
(14,
15) . Secondary outcome measures consisted of the following self-rated questionnaires: 1) the subscales Health Anxiety (11 items) and Illness Behavior (6 items) of the Dutch version of the Illness Attitude Scales, which purports to measure beliefs, fears, and behavior associated with clinical hypochondriasis
(15) ; and 2) the Symptom Checklist-90, a multidimensional measure of psychopathology
(16) . Independent raters assessed global psychopathology using the Comprehensive Psychopathological Rating Scale
(17,
18) . We used the following instruments: the Montgomery Åsberg Depression Rating Scale and the Brief Anxiety Scale. All outcome measures have good psychometric properties.
Statistical Analysis
We analyzed the pretest differences on demographic and clinical variables between the three groups with the use of analysis of variance (ANOVA) for continuous variables and chi-squared tests for categorical variables.
We analyzed the primary and secondary outcome measures by means of General Linear Model 3×2 repeated-measures ANOVAs, with the three groups as between-subject factors and the two evaluations (pretest and posttest) as within-subject factors. We broke down the between-subject factors further into two Helmert contrasts. The first contrast compared the mean change from pretest to posttest scores for the CBT and paroxetine groups with the mean change from pretest to posttest scores for the placebo group. The second contrast compared the mean change from pretest to posttest scores for the CBT group with the mean change from pretest to posttest scores for the paroxetine group. We chose to analyze our data using a relatively limited number of planned orthogonal contrasts because of two connected reasons, namely protection against type I errors and at the same time maximum statistical power to detect possible differences between means, which is especially important in relatively smaller cohort sizes
(19) . We also examined the correlation of changes in hypochondriacal symptoms with changes in comorbid symptoms by means of residualized gain scores.
To compare the magnitude of the treatment effect of both active treatments and the placebo, we calculated standardized effect sizes at posttest by means of Cohen’s d (subtraction of the mean posttest scores of the groups and dividing the difference by the pooled standard deviation).
We further analyzed significant time effects for the primary and the secondary outcome measures for each group separately, using paired t tests (pretest versus posttest).
We also compared the proportion of responders on the Whiteley Index across the three groups. Responders were defined according to the criteria proposed by Jacobson and Truax
(20) . Jacobson and Truax suggest that subjects can be considered to have improved when they shift from a dysfunctional distribution to a functional one, and the reliable change scores exceed measurement error (calculated by dividing the difference between the pretest and posttest scores by the standard error of the measurement). Because of a major overlap in scores for hypochondriacal subjects and nonhypochondriacal subjects, we considered scores below one standard deviation—instead of two standard deviations—of the mean pretest score on the Whiteley Index as falling within the functional range
(15,
21) . Moreover, we calculated confidence intervals for response rates by means of the following formula: proportion of responders minus 1.96 × standard error of observed proportion
(22)In addition, demographic and clinical characteristics of responders and nonresponders were compared using t tests for independent groups or chi-squared tests when appropriate.
All analyses were conducted on an intent-to-treat basis as well as on a completer basis. The first analysis included all subjects with a pretest measurement, regardless of the duration of their treatment. We tried to measure all dropouts at the time they decided to leave the study prematurely. Fifty percent of all dropouts completed a posttest assessment. For the remaining 50% of dropouts, pretest data were carried forward to serve as posttest scores (least observation carried forward). Since the results of the completer analyses were identical to the results of the intent-to-treat analyses on the primary and secondary outcome measures, the results of the latter are reported in this study. With respect to the responder analyses, both the results of the intent-to-treat cohort and the completer cohort are reported in this study, since these results differed.
Results
Attrition
Of a total of 147 subjects assessed with the SCID, 35 subjects (24%) were excluded because of the following: 1) the subject’s most disabling diagnosis did not appear to be hypochondriasis, but another disorder (N=17 [49%]); 2) the subject was unable or unwilling to discontinue antidepressants (N=8 [23%]); or 3) the subject refused informed consent (N=10 [28%]) (Figure 1). Of the remaining 112 subjects randomly assigned, 74 (66%) had been referred by their general practitioner and 38 (34%) responded to articles in newspapers (34%). Subjects were randomly assigned over the three conditions: cognitive behavior therapy (N=40 [36%]), paroxetine (N=37 [33%]), placebo (N=35 [31%]) (χ
2 =2.681, df=2, p=0.26). Of the 112 subjects included, a total of 30 dropped out prematurely, leaving 82 completers. The number of dropouts was evenly distributed over the three conditions (χ
2 =2.49, df=2, p=0.88) (see
Figure 1 ).
Analyses on the pretest scores of dropouts and completers revealed that dropouts worried significantly more about their health (subscale health anxiety from the Illness Attitude Scales, t=–2.314, df=106, p=0.02) and suffered from significantly more anxious symptoms on the Brief Anxiety Scale (t=–2.807, df=107, p=0.01), depressive symptoms on the Montgomery Åsberg Depression Rating Scale (t=–2.199, df=110), and psychoneurotic symptoms on the Symptom Checklist-90 (t=–2.727, df=39.733, p=0.01).
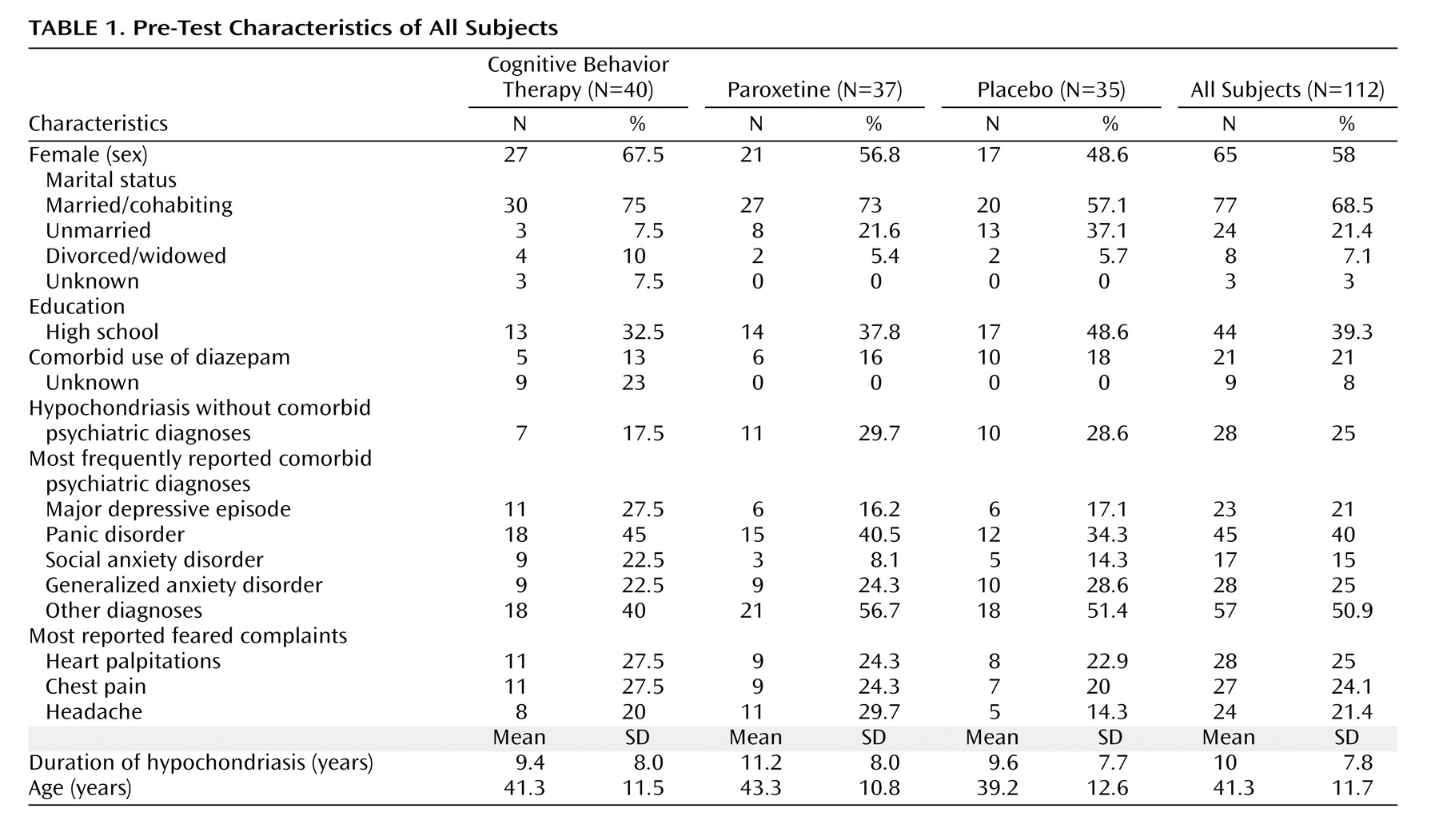
Pretest Characteristics of the Intent-to-Treat Cohort
As can be concluded from the pretest scores, our cohort can be considered severely hypochondriacal, given a mean duration of 10 years (SD=7.8 years), with 75% suffering from comorbid psychiatric diagnoses and 19% using benzodiazepines chronically (
Table 1 ). No significant differences were found between the three conditions, nor were critical differences found between the three sites. In addition, referral by a general practitioner or self-referral did not result in any differences on demographic and psychiatric status variables.
Efficacy
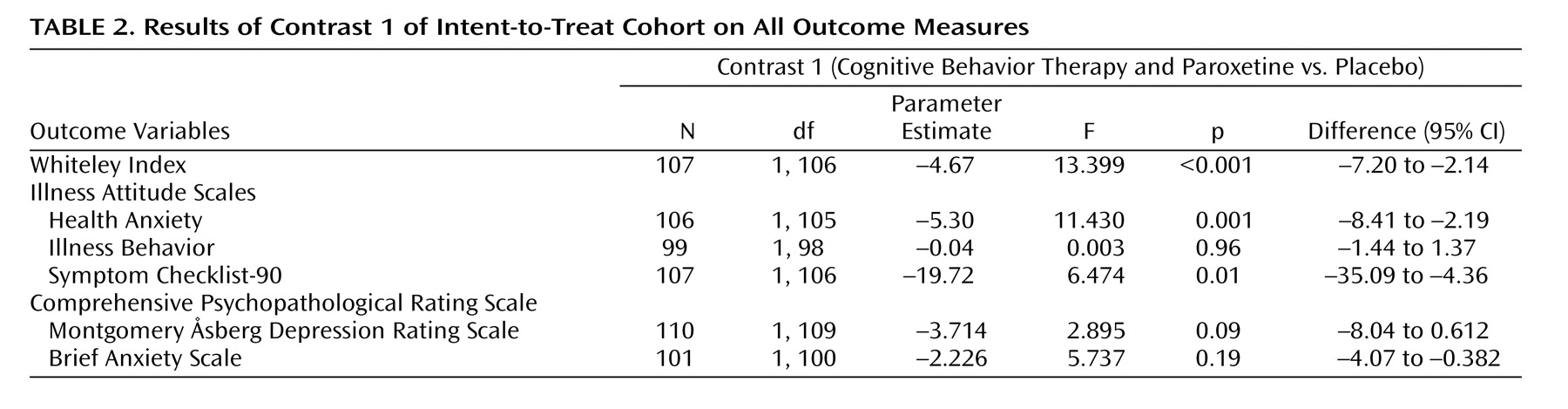
Helmert contrasts on the Whiteley Index revealed significant differences across the two testing points between the placebo group and both treatment groups pooled (
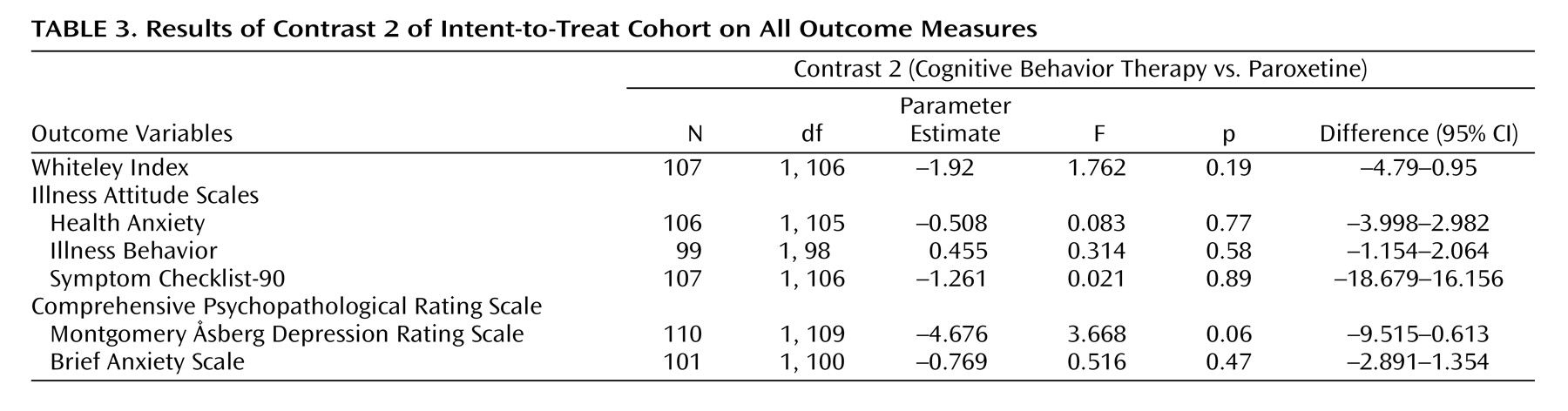
Table 2 ). We found no significant differences between cognitive behavior therapy and paroxetine (
Table 3 ). Except for the subscale Illness Behavior (Illness Attitude Scales) and both subscales of the Comprehensive Psychopathological Rating Scale, the Helmert contrasts for the secondary outcome measures yielded the same pattern of results: pooled cognitive behavior therapy and paroxetine were significantly superior to the placebo. The correlations between changes on the Whiteley Index and the Symptom Checklist-90, the Whiteley Index and the Montgomery Åsberg Depression Rating Scale, and the Whiteley Index and the Brief Anxiety Scale (Comprehensive Psychopathological Rating Scale) were 0.42, 0.69, and 0.65 (all significant at p<0.001), respectively.
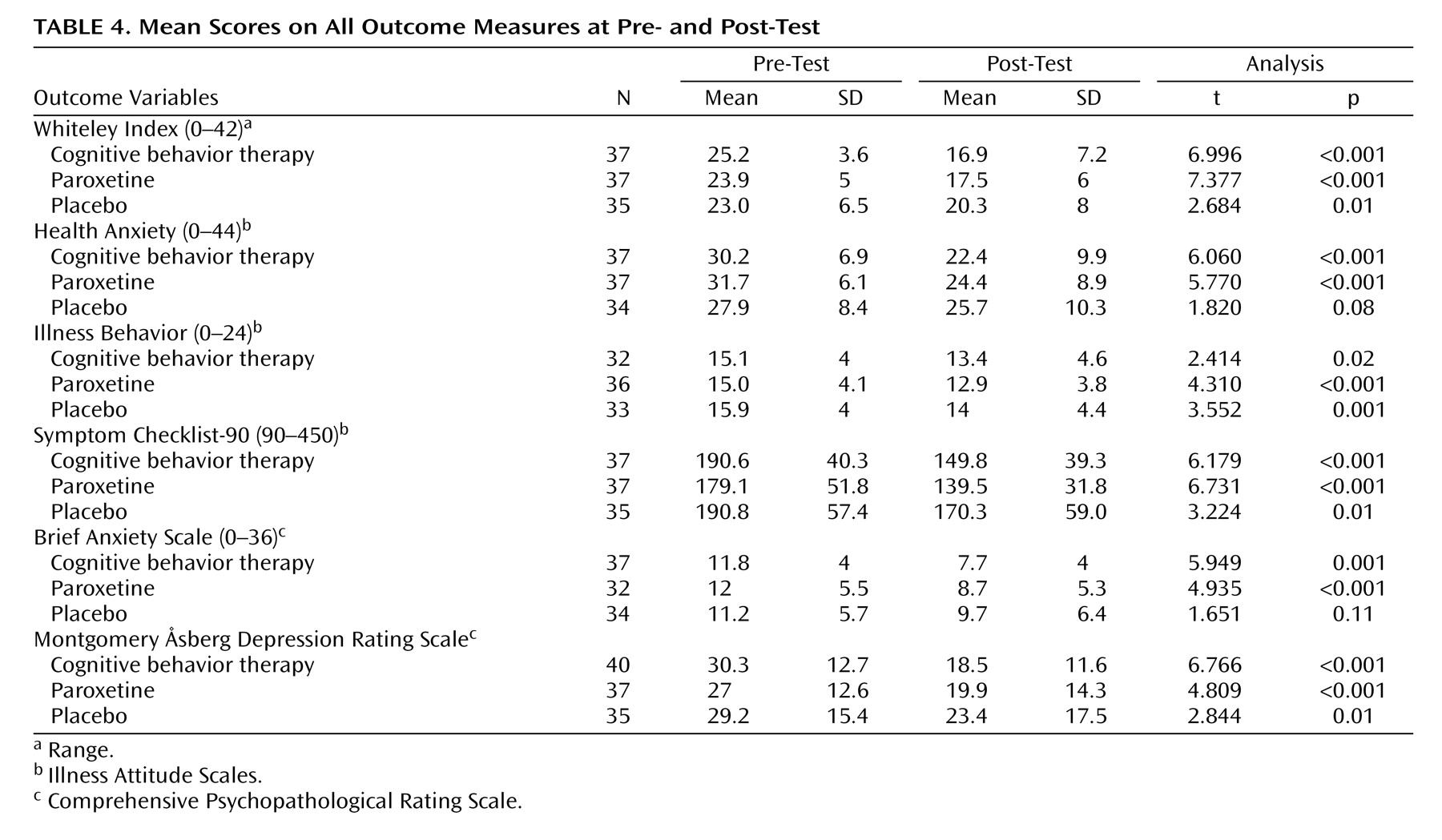
The standardized effect sizes on the Whiteley Index for the comparison between CBT and placebo, paroxetine and placebo, and CBT and paroxetine at posttest were 0.44, 0.40, and 0.09, respectively, for the intent-to-treat cohort and 0.58, 0.53, and 0.11, respectively, for the completers cohort. These results support the results of the Helmert contrasts, namely that CBT and paroxetine are about equally effective and both are more effective than placebo. On most outcome measures, all three groups improved significantly from pretest to posttest (
Table 4 ).
In the intent-to-treat cohort, 45% (95% confidence interval [CI]=030–0.60) of the CBT subjects responded, compared with 30% (95% CI=0.15–0.45) in the paroxetine group and 14% (95% CI=0.03–0.26) in the placebo group. The difference between CBT and placebo in the proportion of responders was significant (χ
2 =8.282, df=1, p=0.004). In contrast, we found no significant differences in the proportion of responders between paroxetine and the placebo (χ
2 =2.482, df=1, p=0.12) and CBT and paroxetine (χ
2 =1.909, df=1, p=0.17). The proportion of responders in the per-protocol cohort was 54% (95% CI=036–0.72) in the CBT group, 38% (95% CI=0.18–0.58) in the paroxetine group, and 12% (95% CI=0–0.25) in the placebo group. Here, we found significant differences between CBT and placebo (χ
2 =10.718, df=1, p=0.001) and between paroxetine and placebo (χ
2 =5.026, df=1, p=0.03). Once again, the difference between CBT and paroxetine was not significant (χ
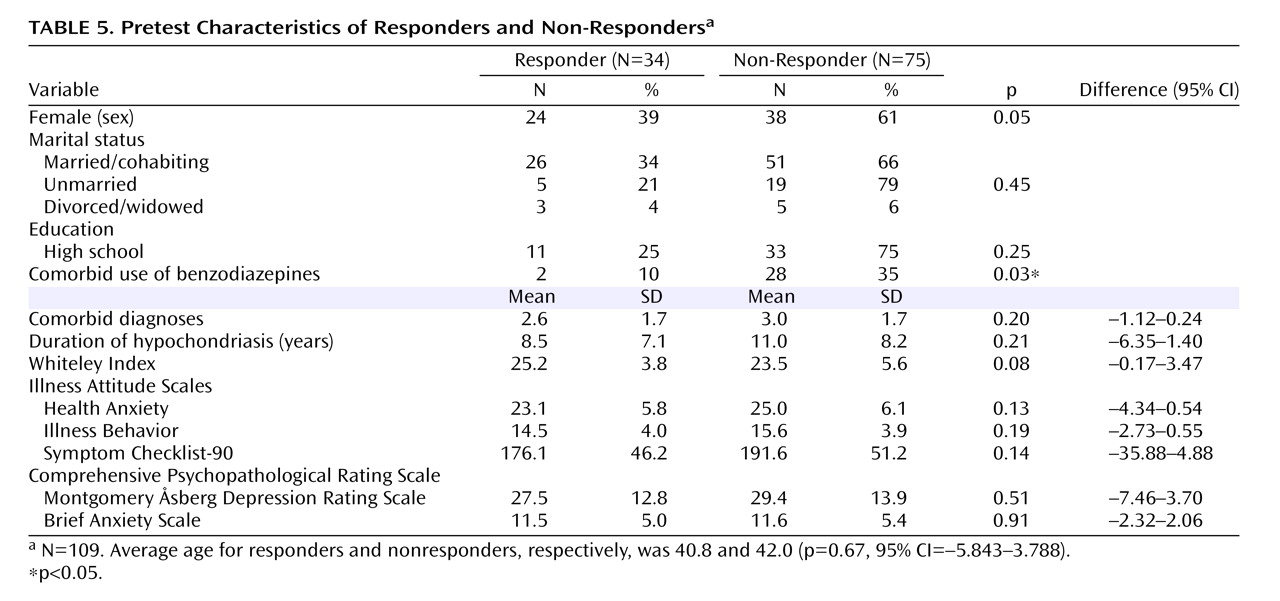
2 =1.238, df=1, p=0.27). Except for benzodiazepine use, responders and nonresponders did not differ critically on demographic and clinical variables (
Table 5 ).
Subjects using benzodiazepines did not have significantly more severe hypochondriacal symptoms than those not using benzodiazepines. However, they reported more depressive (Montgomery Åsberg Depression Rating Scale, t=2.172, df=101, p=0.03) and anxiety symptoms (Brief Anxiety Scale, t=2.489, df=98, p=0.02) than those who were not. These results suggest that subjects used benzodiazepines for symptoms different from those regarding their hypochondriasis. However, we had to demonstrate differences between responders (N=34) and nonresponders (N=75) with a clinically meaningful effect size that was rather limited (0.67, assuming a medium large effect size of d=0.50 and an alpha set at 0.05).
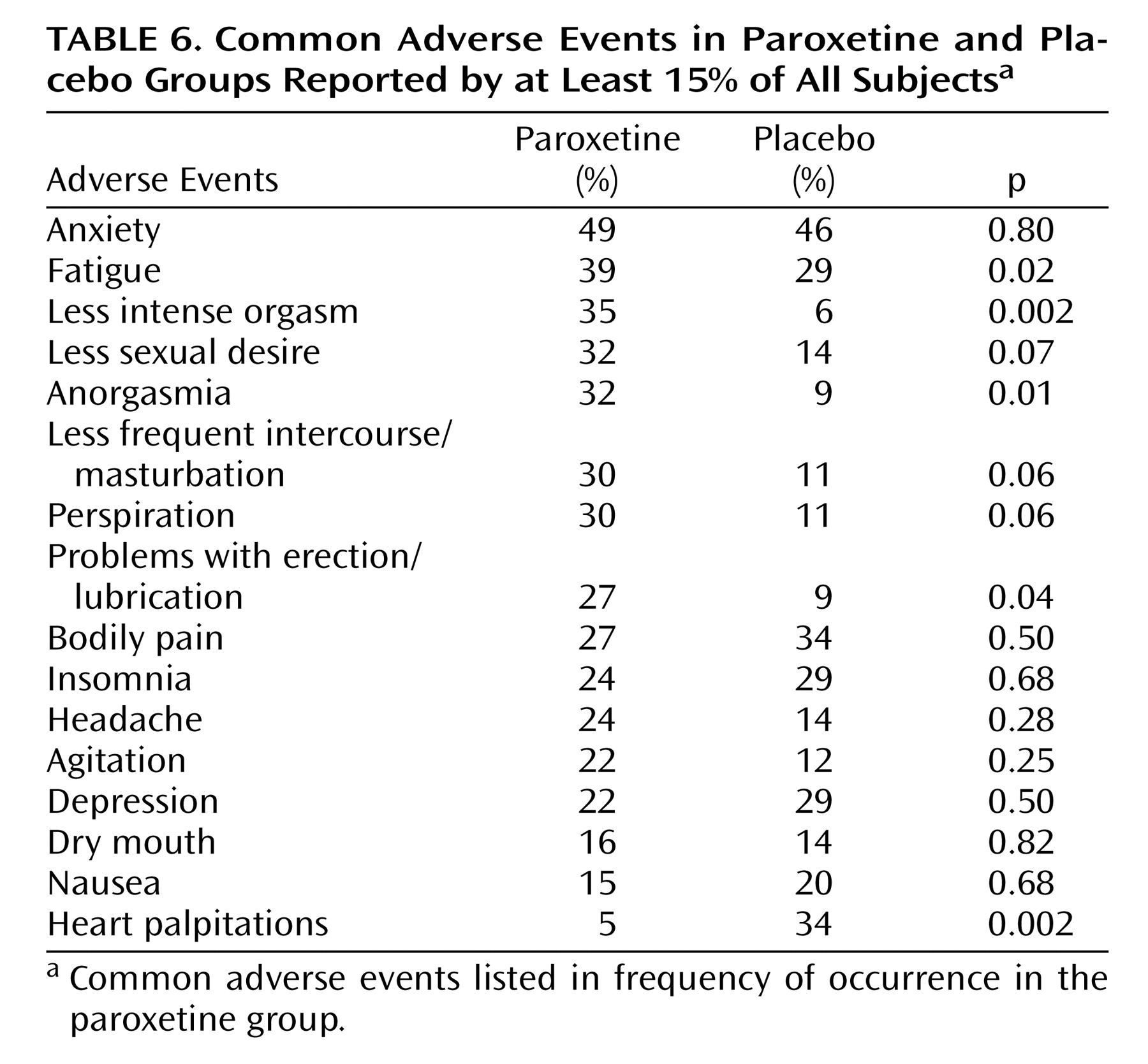
Table 6 lists the adverse events in both the intent-to-treat and completers cohort in frequency of occurrence (regardless of whether they were thought to be related to treatment) in at least 15% of all subjects.
Subjects in the paroxetine group reported sexual problems, fatigue, and perspiration significantly more often. Subjects in the placebo group reported significantly more heart palpitations. No subjects attempted suicide, and none of them reported suicidal ideations.
For the intent-to-treat cohort, the mean final daily dose was 40.0 mg (SD=18.5 mg) in the paroxetine group (median 40.0 mg), compared with 45.4 mg ([SD=21.3 mg], median 60.0 mg) in the placebo group (t=–1.146, df=69, p=0.26). In the treatment completers cohort, the mean final daily dose of the paroxetine group was 46.0 mg ([SD=14.4 mg], median 40.0 mg), compared with 53.1 mg ([SD=13.8 mg], median 60.0 mg) in the placebo group (t=1.593, df=49, p=0.12).
Discussion
This randomized controlled trial investigated the efficacy of 16 weeks of treatment of hypochondriasis with cognitive behavior therapy and paroxetine compared with a placebo. We hypothesized that cognitive behavior therapy and paroxetine would be more effective than a placebo and would not differ significantly from each other in efficacy. These hypotheses were tested by means of Helmert contrasts. First, we compared pooled cognitive behavior therapy and paroxetine with placebo. Second, we compared both active treatments with each other. The results on the main outcome measure, the Whiteley Index, confirmed our hypothesis. In addition, the effect sizes also suggest that cognitive behavior therapy and paroxetine are more effective than a placebo and do not differ from each other. The responder analyses on the Whiteley Index of the intent-to-treat cohort, however, revealed cognitive behavior therapy to have a slight advantage over paroxetine: the proportion of responders differed significantly between cognitive behavior therapy and placebo, but not between paroxetine and placebo. In the completer analysis, paroxetine differed significantly from placebo as well. Considering these results, we can conclude that our findings are compatible with other studies on the efficacy of cognitive behavior therapy
(4 –
7) and expand on it by including also a paroxetine group and a placebo group in a double-blind fashion.
The finding that cognitive behavior therapy and paroxetine were not only effective in reducing the hypochondriacal symptoms, but in reducing symptoms of comorbid anxiety, depressive, and somatoform disorders, is in line with treatment research in anxiety disorders. Antidepressants and cognitive behavior therapy not only ameliorate “pure” anxiety disorders, but comorbid diagnoses as well
(23,
24) . In order to examine to what extent changes in hypochondriacal symptoms were accompanied by changes in other (not hypochondriacal) symptoms, we correlated changes on the Whiteley Index with changes on the Symptom Checklist-90, the Brief Anxiety Scale, and the Montgomery Åsberg Depression Rating Scale. All correlations appeared to be significant. Although we cannot say anything about the direction of the relation, we hypothesized that relief of hypochondriacal symptoms led to amelioration in related symptoms because of several reasons: 1) hypochondriasis was the primary complaint of all subjects included in this study, 2) especially cognitive behavior therapy targeted hypochondriacal symptoms and not the comorbid depressive and anxiety symptoms. These arguments are supported by the finding that both treatment groups did differ significantly from the placebo on hypochondriacal symptoms at posttest, but not on depressive symptoms. Finally, the presence of a comorbid disorder did not predict responder status.
We chose to increase the generalizability of our results by including subjects with a comorbid diagnosis of a mood, anxiety, or other somatoform disorder (75% of our cohort), under the restriction that these comorbid diagnoses were less impairing than their hypochondriasis according to the subject. This decision was based on the results of two studies that examined in detail the prevalence of psychiatric disorder of subjects with DSM-III-R hypochondriasis. Both studies demonstrated that a substantial proportion of subjects with hypochondriasis also suffers from a comorbid depressive disorder (from 44% to 55%) or a comorbid anxiety disorder (from 22% to 86%)
(25,
26) . This means that, in daily practice, clinicians are confronted only rarely with “pure” subjects and selection of subjects without comorbid diagnoses therefore seems to restrict severely the external validity of the results of randomized controlled trials.
Subjects who used benzodiazepines chronically (19% of our cohort) were also included on behalf of generalizability of the results. Even though benzodiazepines are in general prescribed for the comorbid disorders associated with hypochondriasis
(27), it could not be ruled out that changing the benzodiazepine dosage would influence outcome. For that reason, subjects were asked to keep their use at a constant level during the trial, which was checked at all visits. Given our policy with respect to concomitant benzodiazepine use, it seems unlikely that subjects surreptitiously used extra benzodiazepines. We found that subjects using concomitant benzodiazepines responded significantly less than those who were not. Several treatment studies on panic disorder and social phobia also found that benzodiazepine use negatively affected treatment outcome
(28 –
30) . According to Fava et al.
(31), benzodiazepine use increases anxiety sensitivity, the belief that anxiety has undesirable consequences aside from its immediate unpleasantness
(31) . For CBT, this could mean that subjects were less motivated to expose themselves to threatening stimuli and situations, while subjects receiving paroxetine and placebo using concomitant benzodiazepines were less able to tolerate the anxiety, experienced as a side effect of the medication, than subjects who were not using benzodiazepines. This effect of benzodiazepine use is, however, evenly distributed over the three groups.
Considering the fact that there were no significant differences between the three conditions on the demographic and clinical variables and, with the exception of benzodiazepine use, none of these variables predicted responder status, our choice to include a heterogeneous hypochondriacal population was probably not at the expense of the internal validity, namely the reliability or the accuracy of the results. However, we have to be careful when interpreting the results because the statistical power of 0.67, assuming a medium large effect size of d=0.50 and an alpha of <0.05, is inadequate to demonstrate differences between responders and nonresponders. Besides, the twofold increase of the standard deviation at posttest on the Whiteley Index for the CBT group seems to suggest that a subgroup of subjects responds extremely well to treatment, while others do not. Because the primary aim of our study was to demonstrate treatment efficacy, we only analyzed possible differences between responders and nonresponders with respect to clinical variables in order to assess the generalizability of our results. These study aims are demonstrated in the choice of our dependent variables. This leaves the possibility that other unknown variables are important in predicting treatment response (e.g., credibility of the therapy). Future studies, designed especially for predicting which subjects benefit from which treatment, should therefore include a broader array of variables.
Another limitation of the study is that the inadequate statistical power to detect differences between all randomly assigned groups separately led to the choice to analyze our data by means of Helmert contrasts. Although this approach is statistically sound
(19), it, at the same time, reflects a weakness of our study because it excluded the possibility to compare both active treatments separately with placebo. Moreover, it has to be noted that approximately one-fourth of all our subjects dropped out of treatment prematurely, and although the number of dropouts did not differ significantly between the groups, we cannot neglect the risk of randomization being compromised, which could bias treatment effect, reduce statistical power, and decrease the generalizability. Furthermore, dropouts appeared to have more severe symptoms on pretest than completers. For treatment studies, the problem of dropouts warrants the use of more frequent assessments than were conducted in our study, so a more sophisticated data-analytic approach, such as multilevel analysis, can be used. This approach takes into account the differences in the number of measurements for each subject without losing any information.
Notwithstanding the fact that we have put much effort in maximizing the external validity of our findings, we must emphasize that our results can be generalized only to those subjects with hypochondriasis who are willing to undergo psychiatric treatment. Those unable to accept their general practitioner’s explanation that their symptoms and concerns stem from a mental rather than a somatic disorder usually refuse to be referred to a psychiatrist. Instead, they persist until they are referred to a somatic specialist.
However, despite some limitations, the results allow us to conclude that CBT or paroxetine are effective in the treatment of hypochondriasis in a severe and heterogeneous outpatient population. After these treatments, subjects appeared to be less frequently and intensively preoccupied with their fears of having a serious disease and also had less associated depressive, anxious, and psychoneurotic symptoms. Future research should investigate whether these positive effects continue over a longer period of time to gain a full picture about efficacy of these treatments.