An increasing number of studies using postmortem, computerized tomography (CT scan), or magnetic resonance imaging (MRI) techniques have provided evidence for subtle cerebral structural abnormality in individuals with schizophrenia
(1–
5). The most consistently replicated finding is that of larger lateral ventricles and, somewhat less frequently, a larger third ventricle
(2,
6). Studies have also reported enlarged cortical sulci or fissures, suggesting a mild degree of diffuse volume loss
(7–
11). A smaller frontal lobe area, smaller cerebral and cranial size, and a smaller volume of gray matter in the hippocampus and temporal lobe have also been found
(12). Postmortem studies have provided some, but less consistent evidence for subtle structural anomalies primarily in the limbic temporal lobe areas
(13), including smaller hippocampal and/or parahippocampal volumes
(14,
15); alterations in cell density and cytoarchitectural changes in the hippocampus, frontal and enterorhinal cortex, and cingulate gyrus
(16–
22); and enlarged temporal horns
(23,
24).
However, the absolute size of these reported differences between individuals with schizophrenia and normal comparison subjects has been generally small, with notable overlap between the two groups and considerable normal variation within each group. Such normally occurring interindividual variations may mask subtle, yet potentially informative cerebral characteristics related to schizophrenia. To allow a refined focus on schizophrenia-related cerebral characteristics, researchers have sought a research strategy that would reduce the normal variation in brain structure characteristics across individuals.
Researchers have thus investigated the brain structure characteristics in monozygotic twins in pairs that are discordant for schizophrenia. In such research, any differences in brain structure between the twin with schizophrenia and the genetically identical co-twin without schizophrenia must be considered to reflect the disease and the effect of environmental factors.
In contrast, prenatal insults did not consistently characterize these discordant twin pairs. Compared with concordant and normal comparison pairs, the discordant pairs did not have an increased rate of pregnancy complications
(30) or of minor physical anomalies (slight somatic defects that putatively develop during early gestation), although the ill twins tended, nonsignificantly, to have more minor physical anomalies than their well co-twins
(32). On the other hand, notable within-pair differences were found among discordant twins on dermatoglyphic characteristics that are established during the second trimester of gestation
(33,
34). Although those results seem to indicate a prenatal influence disrupting the course of development in individuals with schizophrenia
(27), our previous findings in this sample indicated the importance of trauma at the time of labor and delivery and suggested that birth order may be associated with the timing of obstetric complications occurring in the sample. Discordant pairs in which the twin with schizophrenia was born second in the pair had very high rates of prolonged or precipitous labor (88%) but lower rates of pregnancy complications (38%), while the opposite was true for pairs in which the twin with schizophrenia was born first. Birth order is thus also of interest as a possible mediator of a history of obstetric complications in twin pairs discordant for schizophrenia and may have a relationship to brain structure characteristics.
RESULTS
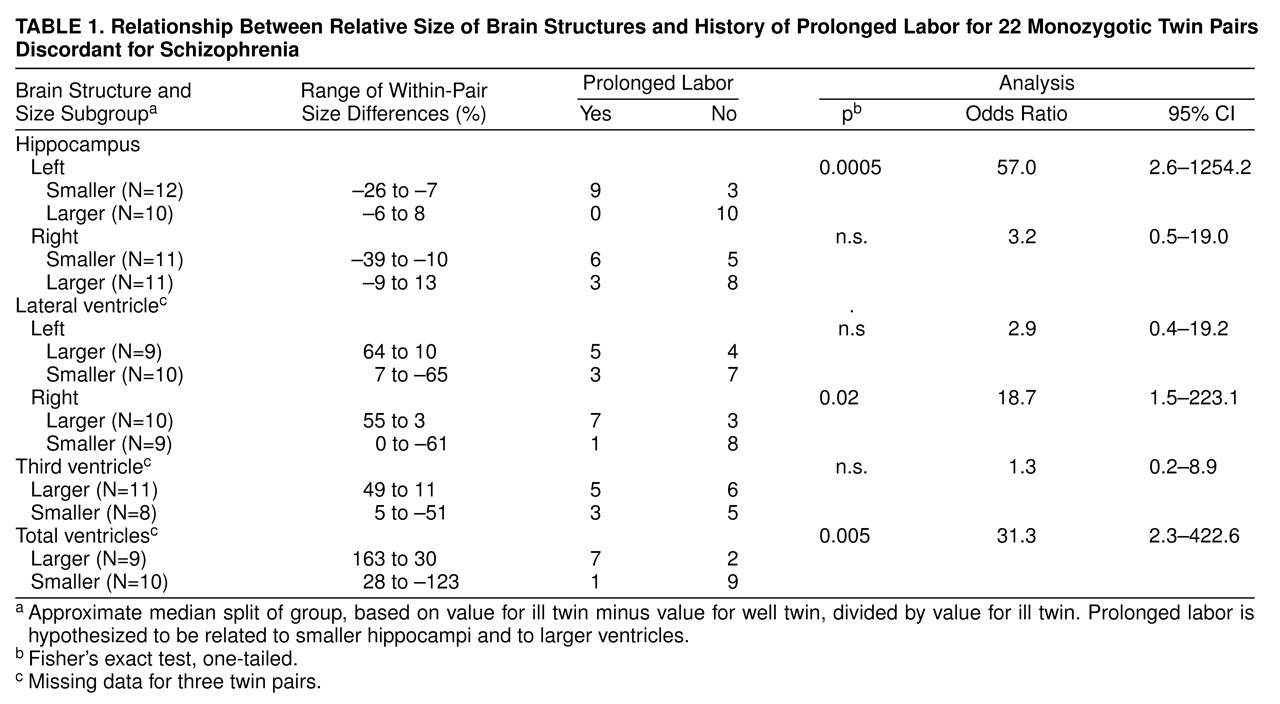
In most of the pairs, the hippocampi were smaller and the ventricles were larger in the ill twin than in the well co-twin. The ill twin had a smaller left hippocampus in 18 of 22 pairs (no tied pairs) (sign test, p=0.002), a smaller right hippocampus in 18 of 22 pairs (one tied pair) (p=0.001), a larger right lateral ventricle in 10 of 19 pairs (two tied pairs) (p=0.32), a larger left ventricle in 14 of 19 pairs (two tied pairs) (p=0.006), and a larger third ventricle in 14 of 19 pairs (no tied pairs) (p=0.03). Nevertheless, for each of the brain areas, the different twin pairs showed a considerable range of scores for relative size in the ill versus well twin, providing an appropriate basis for subgrouping.
table 1 shows the ranges of within-pair values in the two subgroups for each MRI variable.
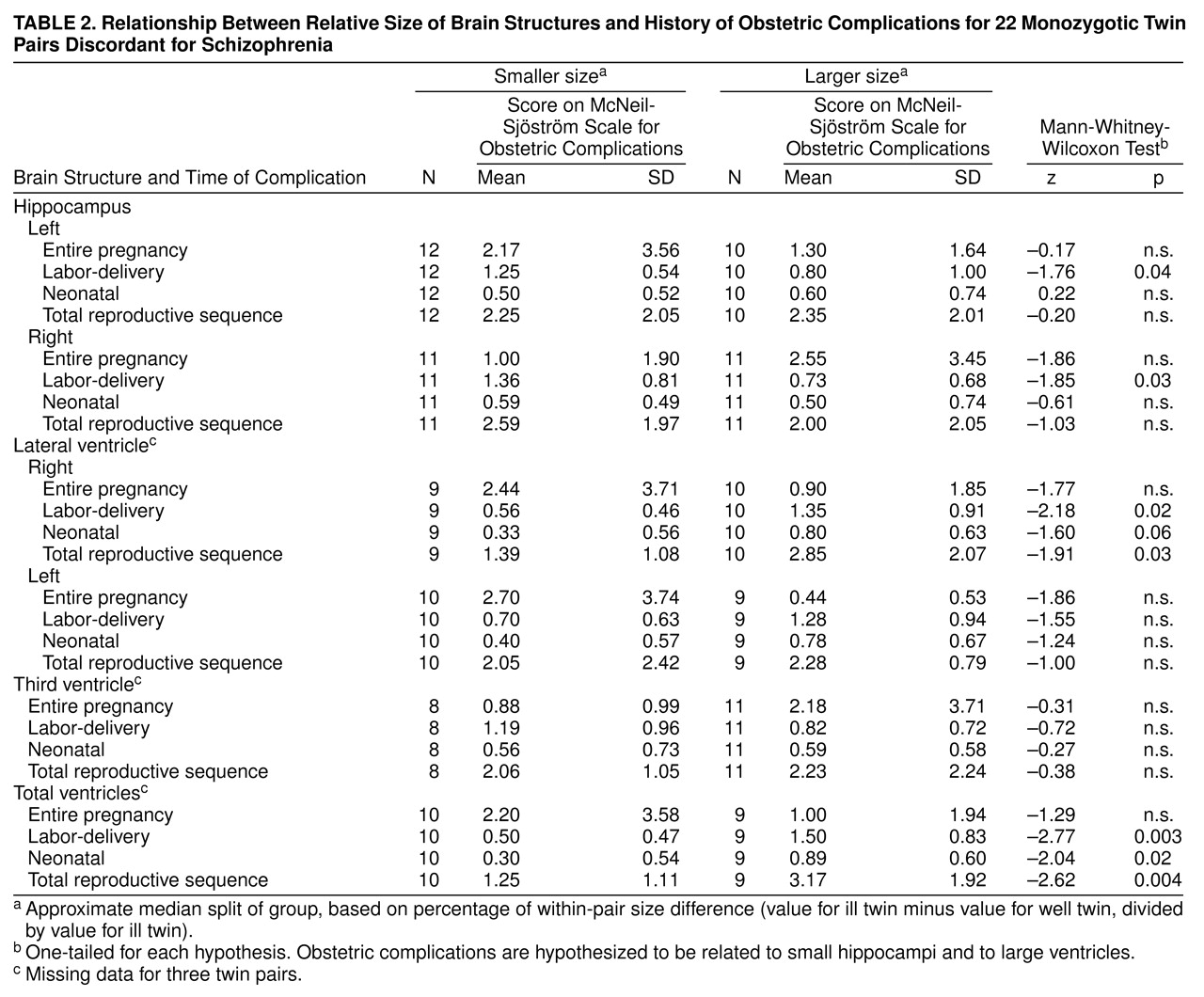
As hypothesized, rates of obstetric complications were significantly higher for the subgroups of twin pairs in which the ill twin had especially small hippocampi and especially large ventricles, and the relationships were specific for both brain area and timing of the obstetric complications (
table 2). An especially small left hippocampus and a small right hippocampus in the ill twin were each significantly related to increased rates of labor-delivery complications only. Furthermore, an especially large right lateral ventricle and an especially large total ventricle size in the ill twin were each significantly related to increased rates of labor-delivery complications, neonatal complications, and total obstetric complications for the entire reproductive sequence. An especially large left lateral ventricle and a larger third ventricle in the ill twin were not associated with an increase in any obstetric complication summary score.
As also hypothesized, the occurrence of prolonged labor was highly significantly related to smaller left hippocampus size in the ill twin and also significantly related to larger right lateral ventricle size and larger total ventricle size in the ill twin (
table 1). Prolonged labor occurred frequently, in nine of 12 twin pairs, in the subgroup in which the ill twin had a relatively small left hippocampus and did not occur at all in the subgroup in which the ill twin had a relatively larger left hippocampus.
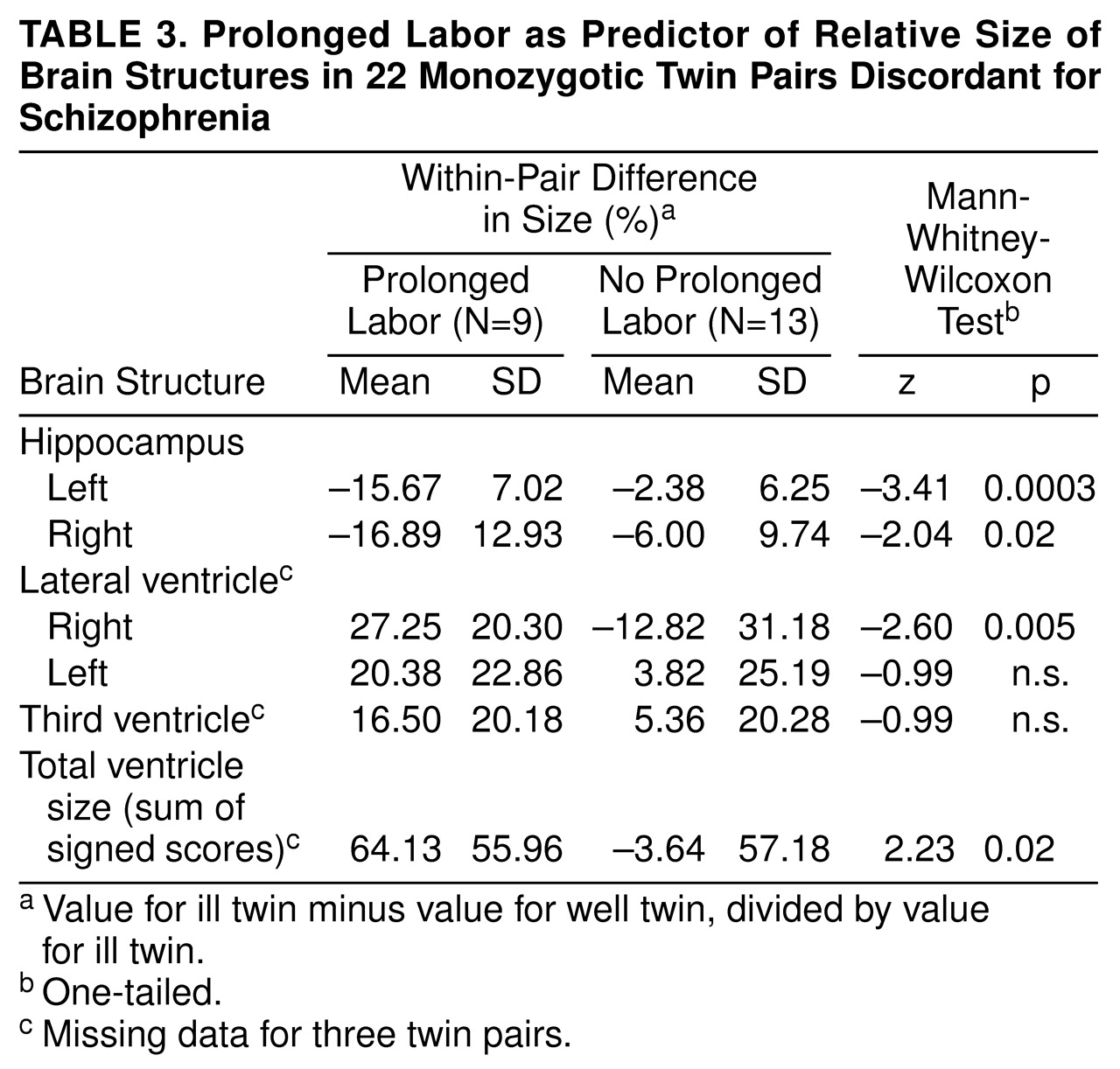
When prolonged labor was used as a predictor variable for relative size of the brain structures within the pair, pairs with prolonged labor, compared with the remaining pairs, were found to have significantly smaller left and right hippocampus size in the ill twin and also significantly larger right lateral ventricle size and larger total ventricle size in the ill twin (
table 3). Furthermore, length of labor, measured in hours, correlated significantly with relatively small left hippocampus size (Spearman rank correlation r
s=–0.55, N=20, p=0.006), larger right lateral ventricle size (r
s=0.53, N=17, p=0.02), and larger total ventricle size in the ill twin (r
s=0.41, N=17, p=0.05), but not with relatively small right hippocampus size (r
s=–0.28, N=20, n.s.), larger left lateral ventricle size (r
s=0.01, N=17, n.s.), or larger third ventricle size (r
s=0.17, N=17, n.s.) in the ill twin.
In contrast, the signs of brain abnormality in the ill twin, such as especially small hippocampi and especially large ventricles, were not significantly related to rates of pregnancy complications (
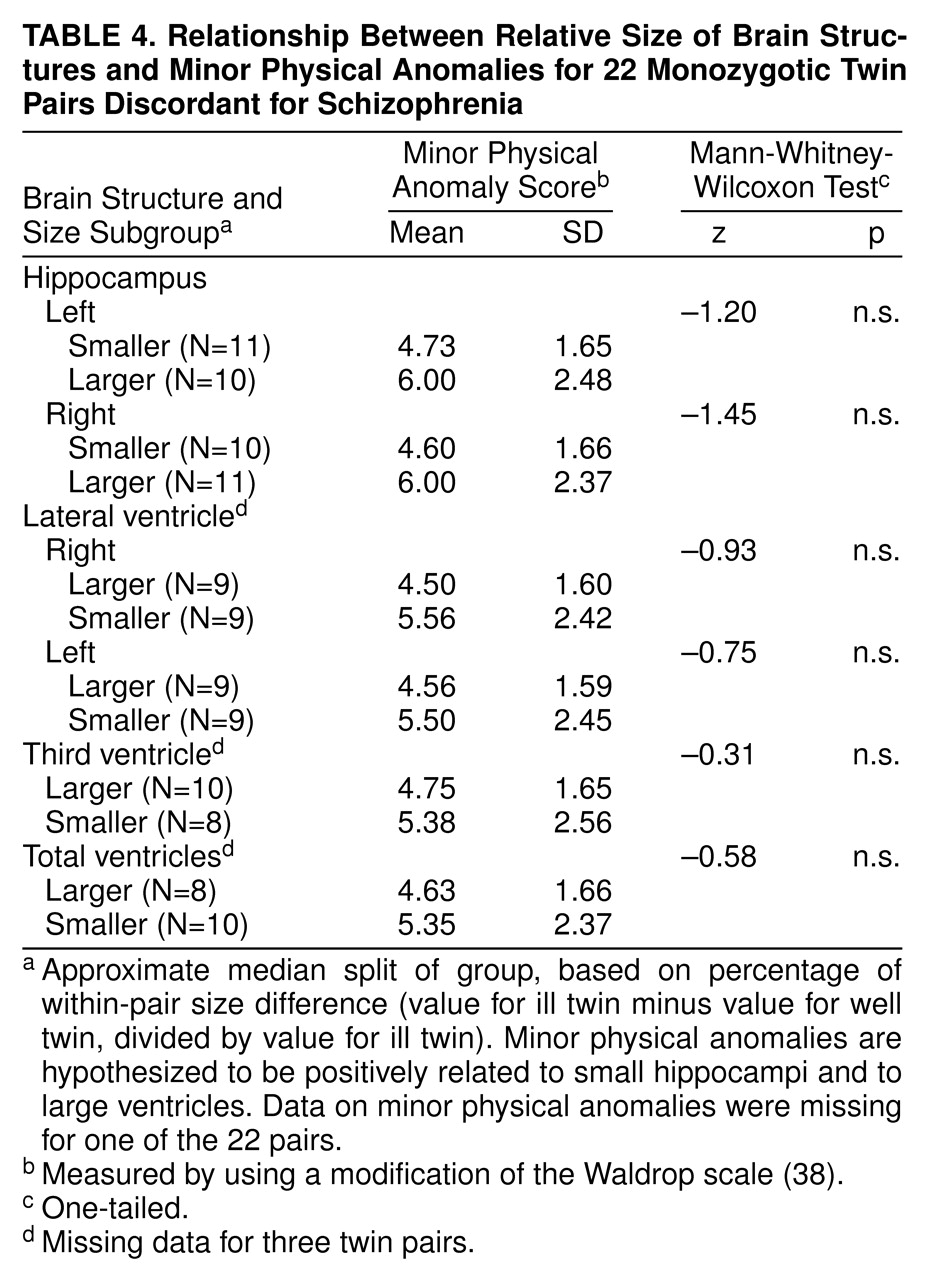
table 2) or to rates of minor physical anomalies (
table 4). Furthermore, birth order in itself was not significantly related to small hippocampi or large ventricles in the ill twin versus the well twin (results available from authors on request).
DISCUSSION
Within 22 monozygotic twin pairs discordant for schizophrenia, the ill twin significantly more often had smaller left and right hippocampi, a larger left lateral ventricle, and a larger total ventricle size than the mentally well co-twin. These results were congruent with the results for a smaller subsample of these cases that had been previously examined
(26). The results also corroborate previous findings in studies of individuals with schizophrenia born singly
(1,
6,
14).
As predicted, obstetric complications were found to be significantly associated with the relative size of brain structures of the ill twins. Increased rates of total obstetric complications for the entire reproductive sequence, as well as of labor-delivery and neonatal complications, were associated with relatively large right ventricle size and relatively large total ventricle size in the ill twin. Labor-delivery complications were more specifically related to relatively small left and right hippocampus size in the ill twin. As a single obstetric complication chosen a priori, prolonged labor showed an impressively strong relationship to smaller hippocampal size and larger right lateral ventricle and total ventricle size in the ill twin. Prolonged labor occurred very frequently, in nine of 12 pairs, and only in pairs in which the ill twin had a notably smaller left hippocampus. The left hippocampus has been identified as a brain area of particular importance in schizophrenia
(6), especially in relation to positive psychotic symptoms
(2). Indeed, correlational analyses showed increased length of labor to be significantly related to smaller relative size of the left hippocampus in the ill twin versus the well twin, as well as to larger right lateral ventricle and total ventricle size in the ill twin versus the well twin.
Prolonged labor thus bore an impressive association with the relative brain structure characteristics in the ill twins. This obstetric complication has been found to characterize patients with schizophrenia in previous studies
(28,
29,
31). The definition of prolonged labor used in this study (more than 10 hours in null parae, more than 6.5 hours in others) was based on modern Swedish recommendations for optimal delivery times and was previously used empirically in our prospective study of high-risk offspring
(39,
41) and in our previous study of obstetric complications in the these twin pairs
(30). In our previous study, the discordant pairs had significantly increased rates of prolonged labor defined in this manner compared with normal or concordant monozygotic twin pairs. Thus, prolonged labor was a salient characteristic of the discordant twin group. This definition of prolonged labor is liberal by other obstetric standards; our international obstetric complication scale
(42) defines prolonged labor as more than 16 hours and more than 10 hours for null versus one or more parae, respectively. During labor, the mothers of the twins in this study appeared to have been subject to considerable clinical surveillance and assisted with interventions as needed, and thus their labors may not have been extremely protracted, as is sometimes seen in other samples of offspring with schizophrenia. Nevertheless, the significant correlations between actual length of labor and both smaller left hippocampus size and larger left lateral ventricle size and larger total ventricle size indicate the apparent relevance of prolonged labor even within the range of labor durations observed for this sample.
Despite the unusual research opportunities offered by this sample, sample size was nevertheless limited, and the power to detect significant differences in within-group analyses of 22 cases was necessarily limited. The odds ratios for some of the statistically nonsignificant findings in table 1 suggested interesting tendencies for prolonged labor to be associated with the size of other brain structures (right hippocampus odds ratio=3.2; left lateral ventricle odds ratio=2.9), and these associations might have reached statistical significance had the sample size been larger. The small sample size suggests caution in drawing any conclusions about the specificity of relationships between prolonged labor and only the left hippocampus as well as only the right lateral ventricle.
Because of the general absence of medical obstetric records for this North American sample, retrospective maternal reports were used as the source of information on obstetric complications. The validity of maternal reports of obstetric complications has been the subject of much speculation, generally unaccompanied by empirical facts. The first systematic study of psychiatric samples clearly suggested maternal reports to be a satisfactory source of information on obstetric complications
(43). In our recent study
(44) of medical record information versus retrospective reports of Swedish mothers (mean age=64 years) of patients with schizophrenia and of normal comparison subjects, considerable discrepancies between the records and the reports of obstetric events and conditions 35 years in the past were found for both maternal groups. In both groups, errors of omission were more frequent than errors of commission, with patients’ mothers tending toward more omissions than comparison mothers (Mann-Whitney-Wilcoxon test, N=45 patient mothers and N=34 comparison mothers, p=0.06, two-tailed). In the sample of twins included in this study, evidence indicated clearly that the reports given by the mothers appeared to be free of commissive errors
(30). Most reported obstetric complications concerned both the ill and the well twin in the pair, and the well twin was often reported to be the more abnormal of the two when differences in obstetric complications did occur within the pair. Furthermore, the report data had predictive validity, as they strongly related to other characteristics of the twins in adulthood; the obstetric complications reported by parents related significantly to independently assessed minor physical anomalies
(32), neurological abnormality
(45), and brain structure size. These three correlates of obstetric complications can all be objectively and reliably investigated
(26,
46,
47), while the reliability of information on obstetric complications is less certain. Given the possible general tendency toward errors of omission (but not commission) in data on obstetric complications, the possibility exists that even more striking relationships would have been observed between obstetric complications and brain structure characteristics if information on the obstetric complications been entirely veridical.
In total, the results for pregnancy complications, minor physical anomalies, labor-delivery complications, birth order, and brain structure characteristics suggest at least two possible trajectories, with seemingly different temporal paths for obstetric complications within the twin sample
(30). One trajectory relates labor-delivery complications to small left hippocampus size to later schizophrenia. Evidence for this trajectory includes our finding that brain abnormality in the ill twin (small hippocampus, enlarged ventricles) was significantly positively related to total obstetric complications and especially to labor-delivery complications, but not to prenatal influence as represented by both pregnancy complications and minor physical anomalies. This relationship may be partly mediated by birth order, as discordant pairs in which the twin with schizophrenia was born second in the pair had very high rates of labor-delivery complications but lower rates of pregnancy complications
(30), and increased rates of labor-delivery complications were related to both small hippocampi and enlarged ventricles in the ill twin. Second-born birth order in the ill twin thus appears to play a role by mediating labor-delivery complications.
The other possible trajectory relates pregnancy complications to minor physical anomalies to nondeviant brain structure (in the ill versus the well co-twin) to later schizophrenia. This trajectory may tend especially to characterize pairs in which the twin with schizophrenia was first born
(30). This subgroup had high rates of pregnancy complications (73%) and lower rates of prolonged or precipitous labor (33%)
(30). Pregnancy complications were significantly positively related to minor physical anomalies in these discordant pairs
(32), but neither pregnancy complications nor minor physical anomalies were significantly related to structural brain abnormality in the ill (versus the well) discordant twins. In fact, both pregnancy complications and minor physical anomalies tended to be related to less brain abnormality in the ill twin (
table 2: right hippocampus and right and left lateral ventricles;
table 4: all brain structures). The most likely explanation for this pattern of results is that the brain regions found to be affected in these ill twins are susceptible to late-occurring obstetric complications, such as labor-delivery complications and even neonatal complications (
table 2), but not to the earlier developmental events represented by minor physical anomalies and pregnancy complications. Furthermore, minor physical anomalies and pregnancy complications were significantly negatively related to labor-delivery complications in this sample
(48), supporting the concept of two different developmental trajectories.
With respect to possible etiological variability, there may well be different timing sequences for obstetric complications as well as different etiological influences among the twin pairs. Twins with schizophrenia whose structural brain characteristics do not differ notably from those of their well co-twins may have received their illness through a different etiological process than did ill twins with notable brain differences, which seem to be related to obstetric complications, and to labor-delivery complications in particular. The concordant pairs in the twin series studied by Torrey et al. are interesting in this respect, as our previous study found that they had significantly lower rates of total labor-delivery complications than the discordant pairs (Mann-Whitney-Wilcoxon test, N=10 and N=23, p=0.02), and only one of the 10 concordant pairs had an abnormal length of labor compared with 52% of the discordant pairs
(30). Although the classic study of Fischer
(49) indicated that genetic factors related to schizophrenia are relevant for discordant pairs, some authors have suggested that discordant pairs represent proportionally more “environmental” etiological influence, while concordant pairs represent more “genetic” etiological influence
(50–
52). This suggestion would be congruent with the significantly increased rates of labor-delivery complications in discordant (versus concordant) twin pairs as well as with the apparent relevance of labor-delivery complications for especially notable differences in brain structure size within discordant pairs.
Interestingly, both the ill and the well co-twins in this study had experienced the same prolonged labor and many of the other obstetric complications as well, but with entirely different psychiatric outcomes. Several possible explanations for this apparent discrepancy in outcome exist. First, the two twins may in reality have received different exposures to what operationally appears to be the same complication. Previous evidence has suggested clearly that only one of the two monozygotic twins in a pair may be compromised by seemingly untoward prenatal or perinatal influences
(30) and that the effect on individuals may depend on many varied and differential prenatal or perinatal intra-uterine influences. For example, twins in the same pair may experience very different prenatal environments as a function of inequality of blood flow, resulting in a wide range of developmental deviations, from poorly perfused cranial tissue and abnormal tissue formation to gross structural deviations, growth retardation with large within-pair birth weight differences, and even death
(53,
54). Differential blood flow could result not only in the more obvious within-pair differences in provision of oxygen and other nutrients but also in potential differences in exposure to infectious and teratogenic agents during pregnancy and labor. The observed within-pair differences in brain structure size and associated psychiatric outcome would be congruent with such variations in exposure to the early perinatal events recorded for these discordant twin pairs.
Second, the obstetric complications that occurred in these discordant pairs may possibly have had a deleterious effect on the well co-twins but did not lead to schizophrenia for other unknown reasons. A significantly increased rate of neurological abnormality was observed in these well co-twins compared with comparison twins
(45), and their neurological abnormality was found to be significantly related to obstetric complications
(45). Lewis et al.
(55) have raised the possibility that early trauma resulting, for example, from labor-delivery complications might actually reduce rather than increase risk for subsequent schizophrenia. Such a reduced risk could possibly be a result of reorganization of the surviving neural circuitry
(56), leading to other neurological abnormality but not to schizophrenia.
Third, other influences occurring during subsequent developmental phases could have provided the basis for divergence in both brain development and mental health status. Perinatal trauma such as that observed in the current sample is known to be related to considerable individual variation in long-term damage and recovery over time
(57) as a result of such influences. The results presented here represent only the relationship between obstetric complications and adult status regarding brain structure size and the presence or absence of schizophrenia and in no way take into account environmental influences occurring after the neonatal period.
The possibility that labor-delivery complications in individuals who later develop schizophrenia are secondary consequences of preexistent abnormality in the fetus has been raised by a number of authors
(58–
60). This possibility would not explain the current findings, as it would be unlikely that a second-born twin who later developed schizophrenia would effectively cause a prolonged labor, while a first-born twin who later developed schizophrenia or two such twins in the same pair (concordants) would not cause prolonged labors. Second-born status is known to be associated with increased risk for asphyxia and other labor-delivery complications
(61). Furthermore, our analyses of data on obstetric complications in the current twin sample, in individuals with schizophrenia born singly, and in genetically high-risk offspring indicated clearly that fetuses with putative prenatal abnormality do not have increased rates of labor-delivery complications, including prolonged labor
(41,
62). The current results showing brain structure abnormality in the ill twin to be positively related to labor-delivery complications but not related to both prenatal factors (pregnancy complications and minor physical anomalies) would further support the conclusion that labor-delivery complications are not secondary consequences of an identifiable preexistent fetal abnormality. Had prenatal abnormality led to labor-delivery complications, then we should have observed brain abnormality to be related to both prenatal factors and labor-delivery complications, with prenatal factors and labor-delivery complications positively related to each other. Neither of these conditions obtained. Nevertheless, we cannot rule out that the labor-delivery complications reflect a primary developmental defect in the fetus rather than an independent trauma to the fetus at delivery. Indeed a recent study has demonstrated that even gross cerebral malformations can be associated with prenatal complications
(63). One additional caveat here, in keeping with findings on the tendency for omissions in obstetrical histories, is that relevant adverse prenatal events may be less dramatic and concrete and thus less likely to be recalled and rated than are labor and delivery events.
The present findings of a relationship between obstetric complications and brain structure abnormalities among discordant pairs do not per se indicate that labor-delivery complications “cause” schizophrenia, as the current within-group analyses only compared obstetric complication history for twins with schizophrenia who had more deviant versus less deviant brain structure characteristics. What the current findings do suggest is that obstetric complications, especially labor-delivery complications, and very specifically prolonged labor are related to brain structure characteristics that are a central focus in schizophrenia. These findings are all the more salient, as they emanate from the very powerful discordant-twin research design and implicate early environmental factors that have been repeatedly observed in other studies of individuals with schizophrenia
(28,
29).
Important insights into the development of schizophrenia might be obtained by providing a qualified answer to the question of why only one of two genetically identical twins, who are seemingly exposed to the very same prolonged labor, develops both schizophrenia and apparently associated structural brain changes lasting into adulthood.