RESULTS
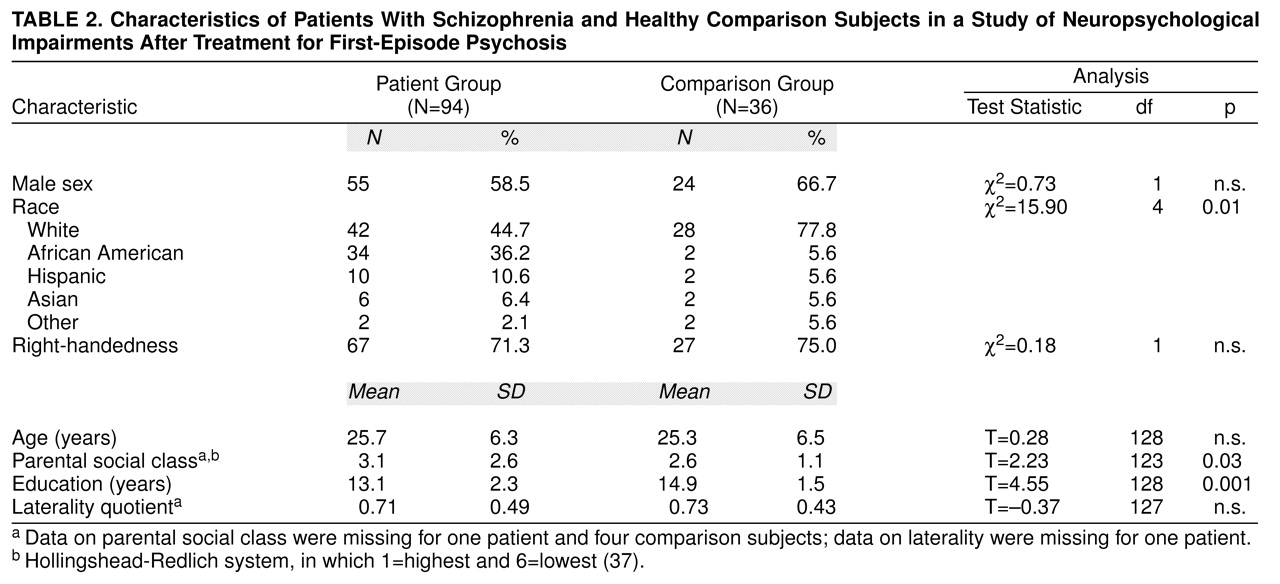
The 94 patients completing neuropsychological exams satisfied RDC for schizophrenia (N=70; subtypes included: paranoid=54, disorganized=4, catatonic=1, and undifferentiated=11) or schizoaffective disorder (N=24). Characteristics of the patient group and the comparison group are provided in
table 2 The groups were well matched on distributions of sex, age, and hand preference, but they differed in racial/ethnic group composition, parental social class, and education. Possible effects of these differences were examined in subsequent analyses.
The 94 patients, who completed at least one comprehensive neuropsychological examination, were a subset of the 118 patients described by Robinson et al.
(23,
24), reflecting an 80% completion rate. To determine if the 94 patients were representative of the larger group, we compared the 94 patients who completed the neuropsychological examinations with the 24 patients who did not. The two groups were similar in age, education, racial/ethnic group composition, parental social class, RDC diagnosis, duration of symptoms before study entry, measures of symptoms at baseline, and course/outcome characteristics (all p values >0.05). Compared to the patients who completed the neuropsychological examinations, those who did not were more likely to be women (75%, N=18, compared to 41%, N=39; χ
2=8.6, df=1, p=0.003) and to have been married (42%, N=10, compared to 16%, N=15; χ
2=24.0, df=3, p=0.00002).
Among the 94 patients, nine patients did not satisfy stabilization criteria at 6 months when they were initially scheduled for examination. They were reexamined during the next year, after they had achieved the criteria. Twelve patients who entered the study before the neuropsychological protocol was put in place (April 1988) were examined as soon as possible after the protocol was established. The modal time from the beginning of treatment to neuropsychological examination was 0.47 years (median=0.61 years); 79% (N=74) of the patients were seen within the first year of any treatment.
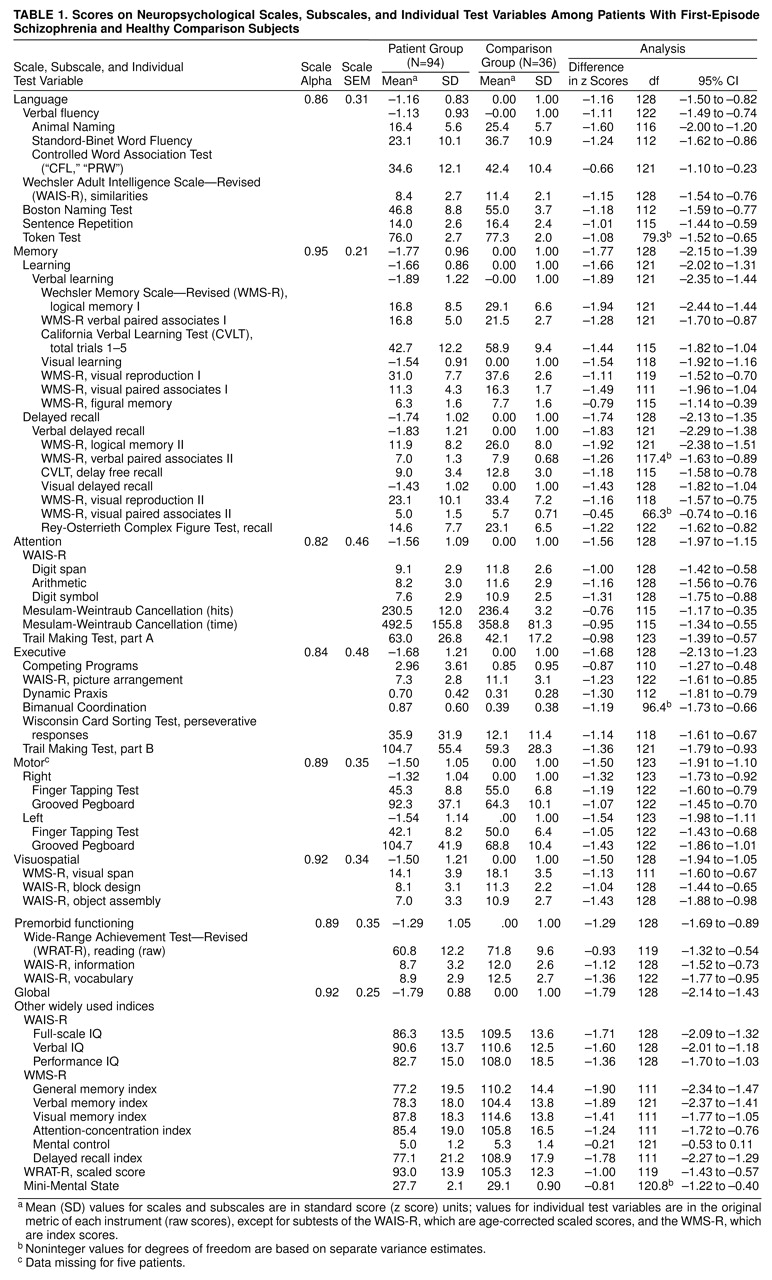
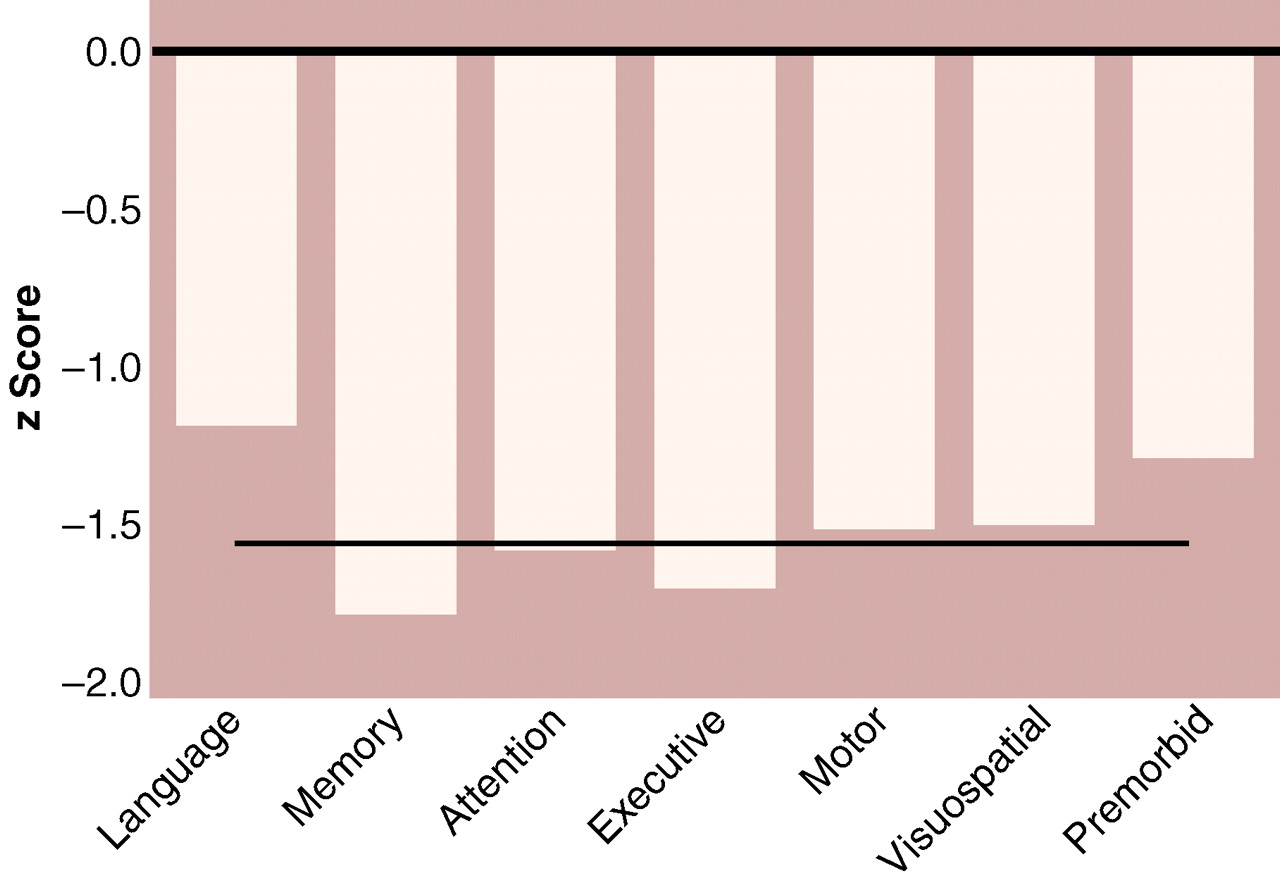
Figure 1 shows the mean neuropsychological profile for the patients relative to the healthy comparison group. The patient group was more impaired than the comparison group on every neuropsychological dimension measured. Mean effect sizes (in z score units, reflecting the number of standard deviations below the comparison group means) ranged from –1.11 to –1.75; 95% CIs ranged from a minimum deficit of –0.82 to a maximum deficit of –2.13 (main effect of group: F=87.2, df=1, 123, p<0.0001, N=125). The overall profile mean for the patients was –1.53, indicating a generalized deficit of approximately 1.5 standard deviations.
The patient profile deviated significantly from flatness; in other words, the means for some scales reflected more impairment than the means for other scales (group-by-scale interaction: Wilks lambda=0.91; F=2.39, df=5, 119, p<0.04, N=125). Specifically, the memory (paired t=3.44, df=88, p=0.001, N=90) and executive (paired t=–2.36, df=88, p=0.02, N=90) scales showed significantly more impairment, and the language scale (paired t=5.64, df=88, p<0.001, N=90) showed significantly less impairment, compared with the remaining scales.
Additional analyses examined possible effects of parental social class (by using MANCOVA), racial/ethnic group composition (by examining results for white subjects, the only racial/ethnic group large enough for analysis), and diagnostic subgroups (by examining results for patients with RDC schizophrenia only compared to the healthy subjects). None of these analyses produced findings that differed substantively from those of the original analyses. No significant differences in neuropsychological profiles were found between the patients with schizophrenia and those with schizoaffective disorder.
Analysis of standardized residual scores revealed a significant group effect (Wilks lambda=0.77, F=5.84, df=6, 118, p=0.001, N=125), with patients showing significant residual deficits on memory (F=5.70, df=1, 123, p=0.02, N=125) and motor (F=6.65, df=1, 123, p=0.01, N=125) scales. Further descriptive statistics and effect sizes for individual tests are provided in
table 1.
Because the generalized deficit of the patients was so large, we examined differences in neuropsychological profiles between groups of patients with low and high levels of general ability (median split on the global neuropsychological scale). The high-ability group (N=43) had a mean deficit of –0.83 standard deviations (95% CI=–0.98 to –0.70), and the low-ability group (N=46) had a mean deficit of –2.22 standard deviations (95% CI=–2.36 to –2.07), relative to the comparison group. MANOVA showed that these groups differed in profile (Wilks lambda=0.65; F=9.03, df=5, 83, p<0.001). The high-ability group showed relative deficits (compared to their own profile mean) only on the memory scale (mean deficit=–1.07, 95% CI=–1.26 to –0.87). The low-ability group showed relative deficits on both the memory scale (mean deficit=–2.48, 95% CI=–2.68 to –2.28) and the executive scale (mean deficit=–2.50, 95% CI=–2.75 to –2.25). The low-ability group also showed a higher mean language scale score than would be expected based on their profile mean (mean deficit=–1.60, 95% CI=–1.82 to –1.38).
Effects of sex were assessed using MANOVA with diagnostic group (patient group or comparison group) and sex as between-subject factors and the six neuropsychological scales as within-subject factors. The main effect of sex (F=0.69, df=1, 121, p=0.40, N=125), and all of the interactions involving sex were nonsignificant (all F values <1). The main effect of group and the effect of the interaction of group and scale were essentially identical to the original analysis. In addition, we examined the sex difference on the scale that measured premorbid functioning. Significantly greater impairment was found in the female patients compared to the male patients (t=2.89, df=92, p<0.005, N=94); no sex differences were observed in the comparison group.
Handedness effects could not be assessed using MANOVA due to a violation in the assumption of multivariate homogeneity of variance (Box’s M=121; approximate F=1.61, df=63, 3297, p<0.002). We therefore examined differences using t tests. No significant effects of handedness were found in the comparison group. In contrast, the 67 dextral patients performed approximately 0.5 standard deviations higher on each scale compared to the 27 nondextral patients. These groups differed in global neuropsychological scale score by 0.47 scaled score units (mean deficit for dextral patients=–1.65, SD=0.87; mean deficit for nondextral patients=–2.12, SD=0.84; t=2.4, df=92, p=0.02). Differences were also observed on the scales for the neuropsychological domains (range of differences on individual scales=0.35–0.63, range of t values=1.6–2.6, df=92, range of p values=0.11–0.01). No significant differences in the distribution of handedness were found among male and female patients.
To examine the possibility that a subgroup of patients with mixed hand preference might be particularly impaired
(38), we inspected scatterplots of neuropsychological scale scores with respect to the laterality quotient. We then examined the effects of adding a quadratic term to the linear relation between the laterality quotient and the global neuropsychological scale score within the patient group. The overall regression analysis was significant (F=6.2, df=2, 90, p<0.003, N=94), but the significance was mostly due to the linear term (beta=0.41, T=3.5, p<0.007), supporting the original analysis. The quadratic term contributed less (beta=–0.18, T=–1.5, p=0.13), and the sign of this term was opposite that predicted if patients with mixed handedness performed more poorly. There were no significant correlations of laterality quotient with neuropsychological scale scores in the comparison group.
We explored relationships between neuropsychological scale scores and demographic, historical, and clinical variables, including: 1) age at time of examination, 2) age at onset of first psychotic symptoms, 3) ratings on the NIMH modification of the Premorbid Adjustment Scale
(39), 4) global ratings of extrapyramidal symptoms made after 8 and 16 weeks of treatment, 5) global measures of course made by physicians after patients completed the first year of the study, 6) ratings on the Social Adjustment Scale made after 2 years in the study, 7) ratings of the deficit syndrome
(40), and 8) medications prescribed at the time of testing. Further descriptions and operational criteria are published elsewhere
(16,
23–
26,
41,
42). Because the goal of these analyses was descriptive, and given the large number of tests conducted, only relations with an effect size equivalent to r>0.30 were interpreted as significant. Use of this threshold protected against type I error and helped ensure that reported findings are likely to be replicated. A sample size of 94 yields 85% power to detect an effect of this size with alpha set at 0.05 (two-tailed). The probability of observing r>0.30 in this sample is approximately 0.005 (two-tailed). The standard error of these correlations is approximately 0.10. Thus we interpreted only effects with probability less than 0.005 (two-tailed), and we can be 95% confident that the true population correlations were within 0.2 of those reported. Some of these results are described below, and others are shown in
table 3.
There were significant correlations between lower neuropsychological scores and poorer Premorbid Adjustment Scale ratings, which were most consistent for social-personal adjustment (e.g., with global neuropsychological scale score, r=–0.34, df=88, p=0.0009) but were not specific to any single neuropsychological function. There were moderate relations of neuropsychological impairment with extrapyramidal symptoms assessed over the first 16 weeks of treatment; patients who did develop extrapyramidal symptoms (N=51) had slightly poorer functioning than those who did not develop extrapyramidal symptoms (N=40) (global neuropsychological scale score: F=5.26, df=1, 89, p=0.01), but did not differ in profile. There were no significant correlations of neuropsychological scales with age in either the patient group or the comparison group, with age at onset in the entire patient sample, or with age of onset among men or women patients.
We examined correlations of scores on each neuropsychological scale with symptom ratings at two time points: 1) at study entry, before treatment (baseline ratings); and 2) close to the time of the neuropsychological examination (typically within 2 weeks of the examination). Ratings on the SADS-C psychosis and disorganization dimensions and on the SANS were examined. There were no correlations greater than 0.30 between neuropsychological scale scores and ratings of symptoms in the SADS-C psychosis and disorganization dimensions at baseline. Correlations with baseline SANS ratings were somewhat more robust; specifically, the SANS global score for affective flattening had correlations >0.30 with scores on the neuropsychological scales for memory (r=–0.31) and attention (r=–0.36) and on the global neuropsychological scale (r=–0.30) (df=91; all p values <0.01, two-tailed). Neuropsychological scale scores correlated more strongly with symptom ratings at the time of the neuropsychological examination (
table 3). Neuropsychological scale scores tended to correlate most with global clinical assessments and ratings of negative symptoms. Neuropsychological deficits explained approximately 5% to 25% of the variance in ratings of course and general social/vocational outcome after 2 years (
table 3).
Scores on the executive scale, compared to other neuropsychological scales, appeared to correlate strongly with several functional indices. Given the theoretical implications of differential associations with executive compared to memory deficits, we tested differences between the size of these correlations
(43). Compared to memory deficits, executive deficits were more strongly correlated with the Global Assessment Scale rating (for the difference between correlations, t=2.33, df=91, p<0.01, N=94) and the mean of SANS global ratings (for the difference between correlations, t=1.66, df=91, p<0.05, N=94).
We examined relationships between neuropsychological scores and treatments prescribed and cumulative antipsychotic dose at the time of testing. Doses of antipsychotics were converted into chlorpromazine equivalents, and doses of antiparkinsonian agents were converted into benztropine equivalents. The median chlorpromazine-equivalent dose was 500 mg/day (mean=712, SD=730, with a range from 0 mg/day [nine patients were receiving no medication] to 3750 mg/day). The median benztropine-equivalent dose among the 71 patients receiving antiparkinsonian agents was 4 mg/day (mean=4.56, SD=2.11, with a range from 0 to 11.5 mg/day).
Scores on neuropsychological scales showed moderate correlations with chlorpromazine-equivalent doses (
table 3). (Correlations involving medication doses excluded data for patients who were not receiving medications.). However, chlorpromazine-equivalent dose also correlated significantly with a variety of symptom ratings, including severity of hallucinations (r=0.55, df=83, p<0.001) and the CGI score (r=0.43, df=83, p<0.001). After statistically controlling for both of these clinical variables, correlations of chlorpromazine-equivalent dose with neuropsychological scale scores were partially attenuated (e.g., r=–0.30, df=80, p<0.005, for the correlation with the memory scale score, and r=–0.28, df=80, p=0.009, for the correlation with the global neuropsychological scale score; correlations with scores on other neuropsychological scales ranged from r=–0.14 to r=–0.26, df=80, p values >0.02).
Benztropine-equivalent dose was significantly correlated with poorer performance on the memory scale (
table 3), but benztropine-equivalent dose was also significantly correlated with the CGI score (r=0.30, df=69, p=0.01) and had similar correlations with scores on SANS items reflecting decreased spontaneous movement (r=0.28, df=69, p=0.02) and poverty of speech (r=0.25, df=69, p=0.04). After controlling for the CGI scores and scores on these two SANS items, the correlation of benztropine-equivalent dose with memory impairment was attenuated only slightly (r=–0.25, df=66, p<0.04).
DISCUSSION
This study characterized the neuropsychological function of patients after initial stabilization of the first episode of schizophrenia or schizoaffective disorder. The patients showed a generalized deficit of approximately 1.5 standard deviations relative to the comparison group. This effect is large in both statistical and clinical terms. In the context of this generalized deficit, language function was relatively spared, memory was most impaired, and executive and motor dysfunctions also emerged as relative deficits (see below). Although these fluctuations are statistically significant, their magnitude pales in contrast to the size of the generalized deficit, prompting questions about their pathophysiological and clinical significance, as noted recently by Mohamed and colleagues
(4).
Classical neuropsychological interpretation of the mean patient profile suggests a relatively nonspecific deficit pattern, which could reflect either diffuse dysfunction or disturbances in key systems (mesencephalic, diencephalic, limbic, or frontal functional systems) that have modulatory efffects on broadly distributed neural networks. Given the caveat that neuropsychological inference based on adult, focal lesion studies may be invalid in the study of schizophrenia
(14,
44), the findings are nevertheless consistent with current conceptualizations of the prevailing neuropsychological deficits in schizophrenia as either “widespread” (i.e., affecting intrinsic cortical circuitry) or as affecting frontolimbic and/or brainstem systems.
The neuropsychological profile observed in this study is similar to results obtained elsewhere in groups of first-episode patients, despite major differences in treatment conditions and more subtle differences in neuropsychological tests and data analytic methods
(4,
7,
17). The combined results suggest that this profile is a relatively constant feature of the syndrome early in its course. The pattern of deficit is also generally consistent with studies of chronic schizophrenia
(6,
45), but the overall severity of the deficit is about 0.3 to 1.0 standard deviations greater in the groups of chronic patients compared to first-episode patients
(16,
46). It remains unclear whether this discrepancy reflects sampling bias (i.e., as many first-episode patients will not go on to have chronic illness) or a deteriorating course and associated cognitive decline in some patients. Recent reports have shown little change and some improvement in first-episode groups followed up to 5 years
(47,
48), but it is difficult to rule out subgroup effects given that only 15%–25% of patients are expected to decline
(44). Further, despite improvement of scores, patients may not show normal gains on retesting, which might reflect functional decline
(47).
Some investigators have focused on relative deficits in learning and memory to implicate mesiotemporal pathology
(6,
49), but comparison of memory impairment in schizophrenia to the amnestic syndrome may be misleading. First, memory deficit was not selective enough to resemble amnesia
(50); other domains (executive, motor) were equally affected. Second, the discrepancy between immediate and delayed memory was not comparable to that observed in amnesia (
table 1; for detailed analysis of these discrepancies, see reference
51). Third, memory dysfunction overlapped statistically with other deficits. Memory tests thus appear sensitive to the cognitive pathology of schizophrenia, but probably tap more complex and multifactorial pathology for most patients. Despite these findings across the group, 28% of the patients may satisfy objective criteria for amnesia based on discrepancies between IQ and memory
(52), and this subgroup merits further attention.
The contrast between patients of high and low neuropsychological ability indicates that learning/memory deficit is present even in patients with a less severe generalized deficit. But in more severely affected individuals, relative deficits in executive functions are also present, and these deficits may be more severe than that for memory. These findings are consistent with the hypothesis of dysfunction in an integrated frontolimbic system, with less severely affected patients showing only learning/memory deficit and more severely affected patients manifesting deficits in executive functions as well
(10).
Motor dysfunction emerged as a relative deficit in analysis of residual scores (i.e., after statistically controlling for all the other scores for that subject). Our finding that motor deficits are statistically independent from memory and other deficits is similar to that of Sullivan and colleagues
(53). Motor deficits may reflect in part adverse medication effects, as seen in studies of acute neuroleptic treatment
(54,
55). This idea is further supported by previous findings of less severe motor deficits in studies of mostly neuroleptic-naive patients
(4,
7). Although an iatrogenic contribution is possible, it is unlikely to be the sole cause of the motor deficits. First, motor dysfunction was neither highly correlated with current or cumulative antipsychotic dose, nor with extrapyramidal symptoms during early treatment. Second, longitudinal analyses in our sample show that motor deficits are present before treatment, are exacerbated acutely by antipsychotic treatment (i.e., over the first few months), and then gradually return to baseline levels with continued treatment
(56). Third, motor abnormalities have been observed in high-risk samples
(57–
60) and in home movies of children who later developed schizophrenia
(61). Although it will be important to examine motor function in patients who receive new antipsychotics with less adverse extrapyramidal effects, the motor impairments reported here likely reflect persistent deficits. Because these motor deficits are statistically independent from other neuropsychological deficits, they may reflect a distinct pathologic process.
Correlations of neuropsychological measures with clinical measures had small-to-medium effect sizes; the strongest indicate approximately 25% shared variance (
table 1). Neuropsychological performance had little relation to symptoms at the time of study entry, but it was correlated with symptoms after clinical stabilization. This finding suggests that symptom assessments of drug-naive patients may offer little insight about persistent deficits. Neuropsychological scales tended to correlate more strongly with negative symptoms than with positive symptoms or symptoms of conceptual disorganization, but the neuropsychological correlations with some positive symptoms were not smaller than the correlations with negative symptoms. This observation suggests that persistent, treatment-resistant positive symptoms may also index a trait-like deficit. The lack of neuropsychological correlations with disorganization symptoms should be considered with caution: this sample had low levels of these symptoms, and language function was relatively well preserved. These observations stand in contrast to findings obtained by using similar methods in a group of chronic patients with both prominent disorganization symptoms and prominent language impairment, where these domains were strongly correlated
(32). Patients with these features may be underrepresented in groups of first-episode patients that include more individuals with good outcome, or these features may emerge later in the illness.
Neuropsychological measures correlated significantly with both childhood adjustment and current global functioning indices, suggesting an early developmental origin of enduring deficits. Executive deficits were the strongest predictors of impairment on the global functioning indices, while memory and attention deficits were the strongest predictors of premorbid adjustment and social-vocational outcome 2 years after study entry. These results are generally consistent with those reviewed by Green
(15).
Recent attention has focused on possible sex differences in neuropsychological functioning, and the implications of these differences for models of etiology and/or pathophysiology
(44,
62–
64). After controlling for normal differences in motor speed (men are faster), we found no neuropsychological differences. We found, however, that within the patient group, women performed more poorly than men on the premorbid index. Because the premorbid index was loaded highly on certain tests (i.e., the information subtest of the WAIS-R) that show normal advantages for men over women
(65), this finding may be an exaggeration of a normal sex difference, or fewer high-functioning women may have participated in testing. In either case, the results fail to support the hypothesis of more severe pathology among men with schizophrenia.
Handedness effects were prominent. Nondextral patients performed approximately 0.5 standard deviations below dextral patients, and the profile shape was similar. These results were not due to a subgroup with mixed-hand preference
(38). We previously noted in a study of WAIS-R results that only strongly dextral first-episode patients had IQ scores above the range of chronic patients
(16). These strongly dextral first-episode patients may be less likely to go on to a chronic course, or they may be more likely to show cognitive deterioration if and when their illness progresses. In either case, our results reveal a major association of nondextrality with global neuropsychological deficit. We previously hypothesized that this association might reflect a generalized failure in cerebral anatomic specialization
(9), but so far there is little direct evidence linking neuropsychological deficits to absence or reversal of normal structural brain asymmetries.
To what extent can findings of neuropsychological deficit in schizophrenia be attributed to medication effects? This question is intractable outside the context of a controlled treatment trial
(55), but it remains important to assess relations of treatment with neuropsychological performance to guide future studies. We found significant correlations between antipsychotic dose and impairment on every neuropsychological scale, but higher dose also correlated with severity of hallucinations and the CGI score. We are no more inclined to suggest that antipsychotic drugs cause neuropsychological deficit than to suggest that antipsychotic drugs cause hallucinations. The results indicate that patients with more severe, treatment-refractory symptoms had greater neuropsychological impairment and received higher doses. Further, given that the association of higher dose with neuropsychological impairment was reduced but not eliminated by statistically controlling for symptom severity, neuropsychological deficits may either prompt dose escalation or result from it.
A similar pattern of results was observed with antiparkinsonian agents. In line with the literature
(66,
67), benztropine-equivalent dose correlated significantly with poorer performance on the memory scale, although it also correlated with poorer performance on executive, motor, and global scales, suggesting little specific effect of anticholinergic load. But benztropine-equivalent dose also correlated with global clinical ratings and items reflecting decreased spontaneous movement and poverty of speech. These findings suggest that patients with persistent akinesia and more neuropsychological deficit tend to receive more antiparkinsonian medication. Because memory deficit was still associated with benztropine-equivalent dose after controlling for extrapyramidal symptoms, there may be a separate anticholinergic effect on memory that deserves further study. Such studies must now consider the overall anticholinergic burden of regimens involving both antipsychotic agents and adjunctive treatments with high levels of anticholinergic activity.