Schizophrenia is conceptualized as a disorder with functional deficits in many areas, including the interrelated domains of attention, cognition, and information processing. Various measures have been used to identify and assess the core cognitive and attentional deficits present in schizophrenia patients
(1). One such indicator is P50 suppression, an operational measure of sensory gating. The P50 is a small-amplitude, positive event-related potential that occurs about 50 msec after an auditory stimulus. P50 suppression is assessed by measuring electroencephalographic (EEG) responses to repeated pairs of clicks separated by about 500 msec, typically presented with interpair intervals of about 10 seconds
(2). The percentage reduction in the amplitude of the P50 response from the first to the second click is the dependent variable labeled “P50 suppression.” In the P50 suppression paradigm, normal subjects typically exhibit robust (i.e., 50%–70%) suppression
(3), while patients with schizophrenia exhibit significantly lower suppression
(2). Deficient P50 suppression in schizophrenia patients has been confirmed repeatedly
(4–
15).
The deficient P50 suppression observed in schizophrenia subjects has prompted further studies
(16) to clarify the clinical and neural substrates of this finding. Poor P50 suppression also occurs among nonpsychotic family members of patients with schizophrenia
(8,
17–
21), indicating that these deficits are not sufficient to produce the syndrome of schizophrenia but may reflect an intermediate phenotypic marker. In this context, Freedman et al.
(18) have reported a linkage between P50 gating and the a7 nicotinic receptor.
The effects of medication on P50 suppression were studied initially in order to assess dopaminergic involvement in deficient P50 suppression among schizophrenia patients. The initial study
(22) contrasted unmedicated patients with those taking typical antipsychotics and with normal subjects. P50 suppression was lower in the schizophrenia patients than in the normal subjects, and in addition, there were no significant differences in P50 suppression between the medicated and unmedicated patients. In order to investigate the specificity of P50 suppression failure, some studies have also compared schizophrenia patients to bipolar disorder patients with acute psychosis. Franks et al.
(23) observed deficits in P50 gating in the acutely ill psychotic bipolar patients, similar to the deficits observed in the patients with schizophrenia. With treatment, this low suppression returned to normal among the patients with mania but not the schizophrenia patients. This finding pointed to both a psychosis-linked, state-related P50 suppression deficit and a more enduring schizophrenia-linked, trait-related P50 suppression deficit, similar to the trait-related deficit in “unaffected” family members of patients with schizophrenia.
We recently reported
(24) that amphetamine, an indirect dopaminergic, noradrenergic, and serotonergic agonist, disrupted P50 suppression in normal subjects. This decrement in suppression is similar to the deficit observed in patients with schizophrenia in our laboratory
(6) and elsewhere
(22) and is consistent with data obtained from animal models of the effects of amphetamine on neural gating and central inhibition
(25–
28). Thus, monoaminergic influences appear to modulate critical components of the neural systems underlying P50 suppression.
Atypical antipsychotic medications appear to have superior efficacy in treating cognitive symptoms
(29). This superiority is associated with a generally more favorable response among patients who have not responded to typical antipsychotics and with fewer extrapyramidal symptoms
(30). With the introduction of atypical antipsychotic medications into the mainstream treatment of schizophrenia, it is important to understand the neurobiological and clinical effects of these drugs. Clozapine may improve P50 suppression in schizophrenia patients
(31,
32), but the generalized effects of atypical antipsychotics on P50 suppression remain unknown. Nagamoto and colleagues conducted a within-subjects examination of P50 suppression in treatment-resistant schizophrenia patients at baseline, after 1 month of clozapine treatment
(31), and again after 15 months
(32). After 1 month of treatment, six patients demonstrated a clinical response to clozapine and had significantly improved P50 suppression, whereas three patients who did not respond continued to have abnormal P50 suppression. After 15 months, nine out of 10 patients had normal levels of P50 suppression, suggesting that the normalization of P50 suppression paralleled sustained clinical improvement in the clozapine-treated patients.
In clinical intervention studies, a distinction has been made between “efficacy” and “effectiveness” studies. In general, efficacy studies examine carefully selected patients who are assigned to a manualized treatment, an alternative treatment, or a no-treatment condition. Typically, only one or very few variables are manipulated, as this design is used to assess the effect of the manipulation with as few confounds as possible. In contrast, effectiveness studies examine a more diverse patient population by using the relatively uncontrolled manipulations seen in clinical practice and are often used in the context of health services research
(33). Thus, patients may be receiving a variety of treatments, and the specific intervention under examination is less regimented and more flexible, to suit the treatment needs of the patients. With effectiveness studies, there is a diminished ability to infer underlying causal mechanisms, but the results may be more generalizable to the heterogeneous patients (and treatment approaches) seen in clinical practice. In the present study, we examined the omnibus “effectiveness” of medication status (atypical versus typical antipsychotic medications) in a heterogeneous group of schizophrenia patients treated with a variety of atypical and conventional psychotropic medications. P50 suppression was assessed in these two groups to determine whether conducting a more controlled (and expensive) within-subjects, longitudinal study of the effects of atypical antipsychotic medications on P50 suppression is warranted. Deficient P50 suppression has been observed in several different laboratories among schizophrenia patients treated with typical antipsychotic medications. Given the evidence of normalization of deficient P50 suppression by clozapine
(31,
32), we anticipated that the patients treated with atypical antipsychotic medications would have greater P50 suppression than would patients treated with typical antipsychotics.
Method
Participants
Twenty-six patients (13 men, 13 women) with a diagnosis of schizophrenia according to the Structured Clinical Interview for DSM-IV Axis I Disorders, Patient Edition
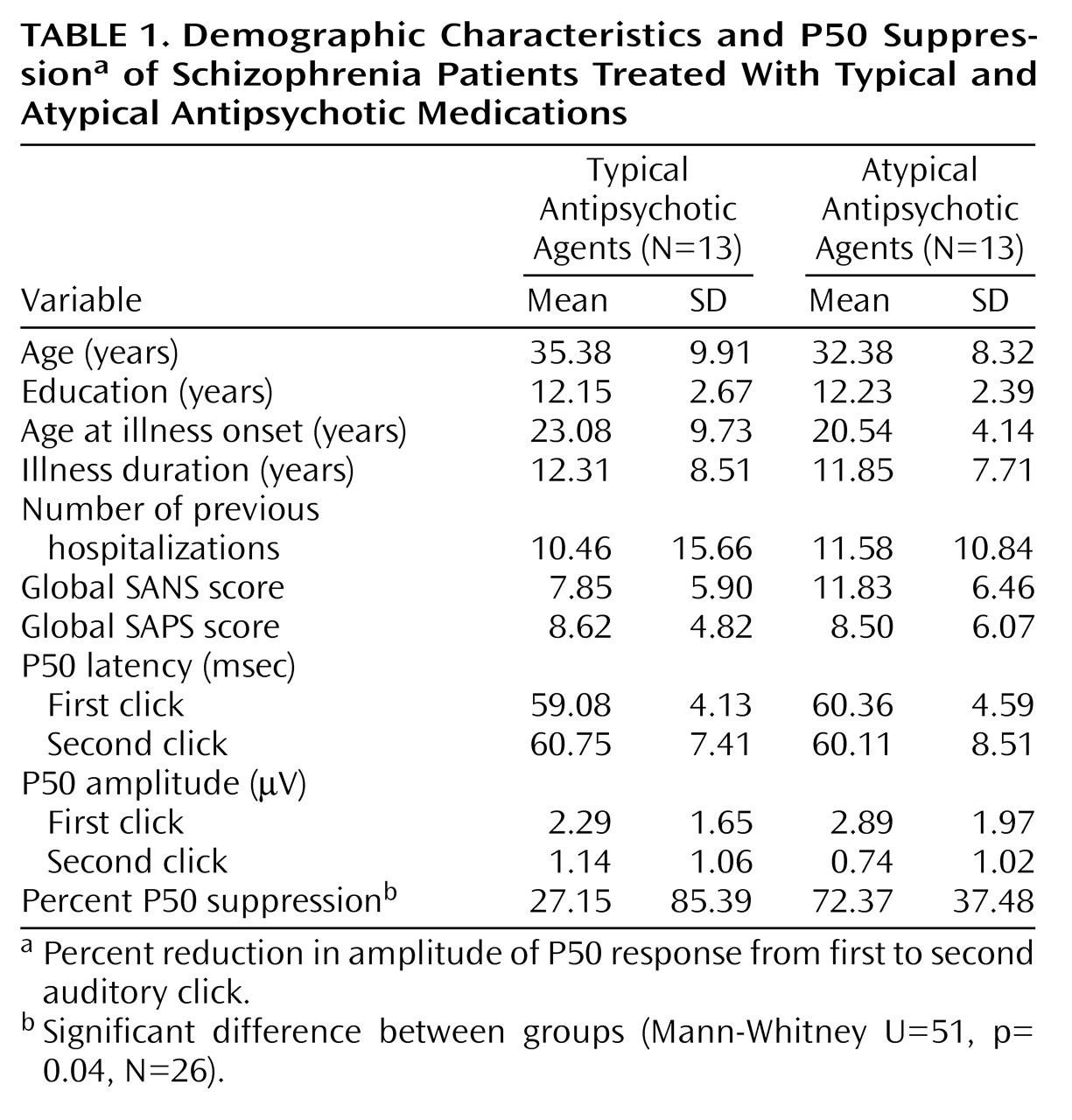
(34), were recruited from a long-term chronic care inpatient facility and were divided into two groups on the basis of their current medications in a between-subjects design. Thirteen patients (six men, seven women) receiving clozapine (N=5), olanzapine (N=6), or risperidone (N=2) were compared to a second group of 13 patients (seven men, six women) receiving conventional neuroleptic medications. While there are differences among the atypical antipsychotics, we sought to use a liberal inclusion criterion for the purposes of this preliminary study testing the generalized, omnibus effect of atypical antipsychotic medications. The patient groups were equivalent on the following demographic variables: age, gender, years of education, age at illness onset, illness duration in years, and number of previous psychiatric hospitalizations (
Table 1). The Schedule for the Assessment of Negative Symptoms (SANS)
(35) and the Schedule for the Assessment of Positive Symptoms (SAPS)
(36) were administered within 1 week of P50 testing. Written informed consent was obtained from all study participants after the procedures had been fully explained.
P50 Measures
The P50 testing was conducted as described previously
(6–
8). Briefly, each participant was seated in a comfortable recliner and instructed to relax with his or her eyes open and to focus on a fixation point. The testing took place in a quiet, lighted, but not electrically shielded room. During the testing the subject was monitored visually and by EEG for signs of sleep or slow wave activity, which, if present, prompted the experimenter to speak briefly with the subject. The 120 pairs of auditory clicks were presented every 8–12 seconds, with a 500-msec interclick interval. The stimuli were generated by means of computer-driven, 89-dB pulses of 1-msec duration produced by using a signal generator and data acquisition system for the recording of EEG and event-related potential waveforms. Recordings were performed at the Fz, Cz, Pz, F3, F4, C3, and C4 sites with a forehead ground and linked earlobe reference. Data will be presented from the Cz site only because when so few sites are used, Cz alone is best for discriminating schizophrenia patients from normal subjects
(5,
7,
37). Eye movements and blinks were monitored with electro-oculographic (EOG) recording. The resistance of all electrodes was less than 5 kW . The evoked responses were amplified with a Grass Model 12 Neurodata Acquisition System (Quincy, Mass.) with a bandpass of 0.1 to 300 Hz, with no 60-Hz notch filter. The response was digitized at 1000 Hz, and the results of the individual trials were stored to disk for analysis. Subsequently, the data were digitally low-pass filtered at 100 Hz before artifact screening to eliminate any residual electrical noise. The EEG and EOG channels were then screened for postacquisition artifacts, and trials containing artifacts (50 mV EOG or EEG channel) were not included in the waveform averaging. The artifact-free epochs were averaged and digitally bandpass-filtered (5 to 50 Hz) in the frequency domain. The filter had 12-dB/octave high- and low-pass slopes similar in gain characteristics to those reported by Jerger et al.
(38).
The P50 component was identified as described in previous reports
(6,
14,
24,
37). The P50 was defined as the most positive deflection 40 to 80 msec after stimulus presentation. P50 amplitude was defined as the absolute difference between the P50 peak and the preceding negative trough. The evoked potential peaks, amplitudes, and latencies were first screened with an automated computer algorithm and then manually verified off-line by investigators blind to subject and condition. The percentage of P50 suppression was calculated by using the following formula: (1 – [second click amplitude/first click amplitude])× 100.
Results
P50 Measures
In addition to statistical tests, two measures of effect size were used: mean difference and standardized mean difference ([mean
1 – mean
2]/standard deviation)
(39,
40). According to Cohen
(40,
41), an effect size of 0.2 is considered small, while 0.5 is a moderate effect, and an effect size larger than 0.8 is large. Homogeneity of variance was assessed by using the Levene test. Where appropriate, nonparametric comparisons were used if unequal variances were present. P50 variables are shown in
Table 1. No statistically significant differences were observed with respect to P50 latencies (first click: t=–0.75, df=24, p=0.46; second click: t=0.20, df=24, p=0.84) or P50 amplitudes (first click: t=–0.83, df=24, p=0.41; second click: t=0.98, df=24, p=0.34). In this cohort, first-click amplitude was not significantly correlated with P50 suppression (r=0.09, df=26, p=0.67). Given the specific directional nature of the a priori hypothesis and the skewed distributions associated with P50 suppression, a one-tailed Mann-Whitney test was performed in the comparison of the P50 suppression of the patients taking atypical versus typical antipsychotic medications. In keeping with the methods of Nagamoto et al.
(37) and other laboratories
(9,
42), P50 suppression ratios below –100% were truncated to –100%. The patients treated with typical antipsychotic medications had significantly lower P50 suppression (
Table 1); the mean difference was 45%, and the standardized mean difference was –0.74. The degrees of P50 suppression were 82.55%, 74.95%, and 39.19%, respectively, for the patients receiving clozapine, olanzapine, and risperidone.
Symptom Ratings
The SANS and SAPS scores of the patients receiving typical and novel antipsychotic medications were compared. According to independent samples t tests, the patient groups did not differ on the global SAPS (t=0.05, df=24, p=0.96), global SANS (t=1.61, df=24, p=0.12), or any of the subscales. Nevertheless, given the noticeably higher mean SANS score of the patients receiving atypical antipsychotic medications (
Table 1), we examined the relationship between SANS score and P50 suppression and found that the global SANS rating accounted for only 2% of the variance in P50 suppression (r=0.16, N=26, p=0.46). When we used an analysis of covariance with SANS score as a covariate, the difference in P50 suppression between groups was unchanged (F=3.74, df=2, 23, p=0.03).
Discussion
These results indicate that schizophrenia patients who are receiving atypical antipsychotic medications have P50 suppression scores that are in the normal range (mean=72%). In contrast, schizophrenia patients receiving typical antipsychotic medications exhibit deficient P50 suppression (mean=27%). Gating deficits in patients receiving typical antipsychotic medications have been well established in previous studies and are consistent with our data. Despite the differences in P50 suppression between the groups receiving atypical and typical antipsychotic medications, the groups of schizophrenia patient were grossly equivalent on global and subscale SANS and SAPS symptom ratings, minimizing the possibility that symptom state accounts for these results.
The results of the present investigation are consistent with reports that clozapine improved P50 suppression in a study of patients with treatment-resistant schizophrenia
(31,
32) and that risperidone reduced second-click amplitude (but not P50 suppression ratios) in patients with recent-onset schizophrenia
(43). The normal range of P50 suppression in our schizophrenia patients receiving atypical antipsychotic medications is similar to the improvement of P50 suppression in manic patients after successful medication treatment and the associated improvement in clinical state
(23).
In a similar between-subjects study of sensory inhibition in patients with schizophrenia, Kumari et al.
(44) examined prepulse inhibition of the startle reflex in 11 patients taking typical antipsychotic medications and in nine patients receiving clozapine. Although deficits in prepulse inhibition have been repeatedly confirmed in patients with schizophrenia receiving typical neuroleptics
(16,
45–
47), the patients receiving clozapine had normal-range prepulse inhibition and were similar to the patients receiving typical neuroleptics on demographic and clinical characteristics
(44).
A key issue regarding the present results is the possibility of preexisting differences between the patients who were selected for treatment with atypical antipsychotic medications and those receiving typical antipsychotics. In addition, the medications received by the patients in this study may simply reflect the wider range of medication options now available to psychiatrists. Our data indicate, however, that the patient groups were equivalent on illness variables (e.g., age at illness onset, duration of illness, and number of psychiatric hospitalizations) and on symptom measures (e.g., SANS, SAPS, Global Assessment of Functioning Scale) at the time of testing. While the patients receiving atypical antipsychotic medications were rated as having higher levels of negative symptoms, it remains unclear whether the patients had equivalent symptom levels in the years before they received their current medication regimens. This issue needs to be addressed in a longitudinal, controlled study.
Although the “effectiveness” design used in this study is limited because causal inferences cannot be drawn, the heterogeneous group of patients studied is typical of patients seen in clinical settings and may suggest directions for additional investigations. The present findings provide justification for carefully controlled longitudinal studies of specific medications (e.g., those described in references
31,
32, and
43) that would examine the unique pharmacological effects of medications used in the treatment of schizophrenia and to assess their differential effects on sensory gating, symptom change, neurocognition, and functional outcome.