Schizotypal personality disorder is characterized by oddities in appearance, perception, and behavior that appear to represent a milder variant of schizophrenia
(1). A biological relationship between chronic schizophrenia and schizotypal personality disorder has been supported by genetic and family studies
(2), by similarities in performance on measures of attention and information processing
(3), and by neurochemical similarities
(4).
Similarities between schizophrenia and schizotypal personality disorder have also been demonstrated on clinical measures of neuropsychological function. Generally, the neuropsychological deficits evident in schizophrenia include impaired abstraction, attention, language, and verbal learning and memory, which are thought to reflect involvement of frontal and left temporal-limbic brain regions
(5–
9). Until recently, neuropsychological function in schizotypal personality disorder was relatively poorly understood, since few studies included subjects who met full diagnostic criteria for the disorder, and few cognitive domains were evaluated. The few extant studies that examined cognitive performance in patients with clinically defined schizotypal personality disorder
(10–
12) have suggested deficit patterns similar to, but less severe than, those seen in schizophrenia. Similar results were reported in nonclinical “psychosis-prone” populations
(3).
We previously studied the neuropsychological profile of schizotypal personality disorder by examining a wide range of cognitive functions in right-handed male subjects who met full DSM-IV criteria for schizotypal personality disorder and found significant deficits on measures of verbal learning and abstraction
(13). These deficits were apparent against a background of general mild impairment in other cognitive domains. This profile was similar to that found in subjects with schizophrenia, albeit less severe, and we suggested it might reflect similar involvement of frontal and left temporal brain areas. As measured by the California Verbal Learning Test
(14), verbal learning in patients with schizotypal personality disorder was characterized by a reduced number of words learned over five trials but not by an increased rate of forgetting. This is consistent with a disturbance in encoding or retrieval from memory but not storage of information. The learning deficit was further compounded by an impairment in semantic organization or “clustering” of the word list to facilitate learning, similar to that reported in first-degree relatives of patients with schizophrenia
(15). In contrast, nonverbal learning skills were relatively preserved. Within the context of impaired performance on a measure of abstraction, it was unclear if our finding of a deficit in verbal learning reflected a primary deficit in language processes, in learning, or in concept formation and organization.
The purpose of the current study was to further examine the verbal learning deficit in DSM-IV-defined schizotypal personality disorder by evaluating selected components of verbal and nonverbal attention, learning, and memory. On the basis of results from our previous study, we hypothesized that 1) subjects with schizotypal personality disorder would show a general impairment on these measures relative to comparison subjects, 2) memory retention (i.e., rate of forgetting) would be relatively preserved, and 3) subjects with schizotypal personality disorder would show more impairment on verbal than nonverbal analogs of these various measures.
Discussion
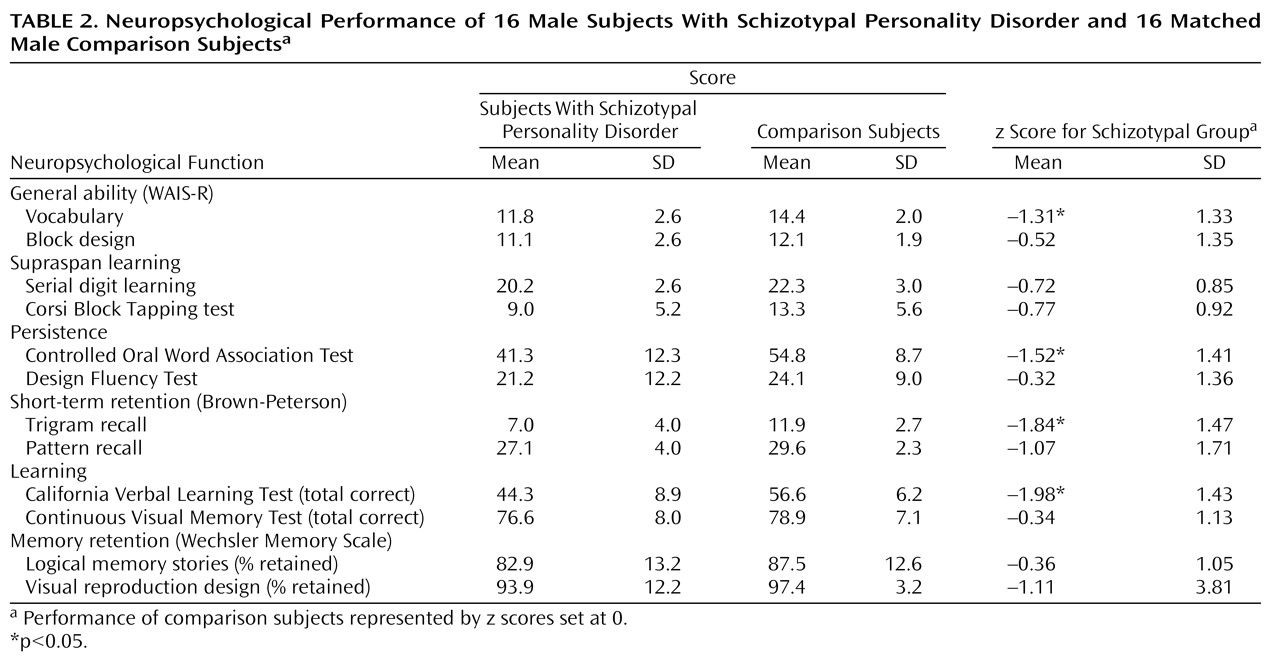
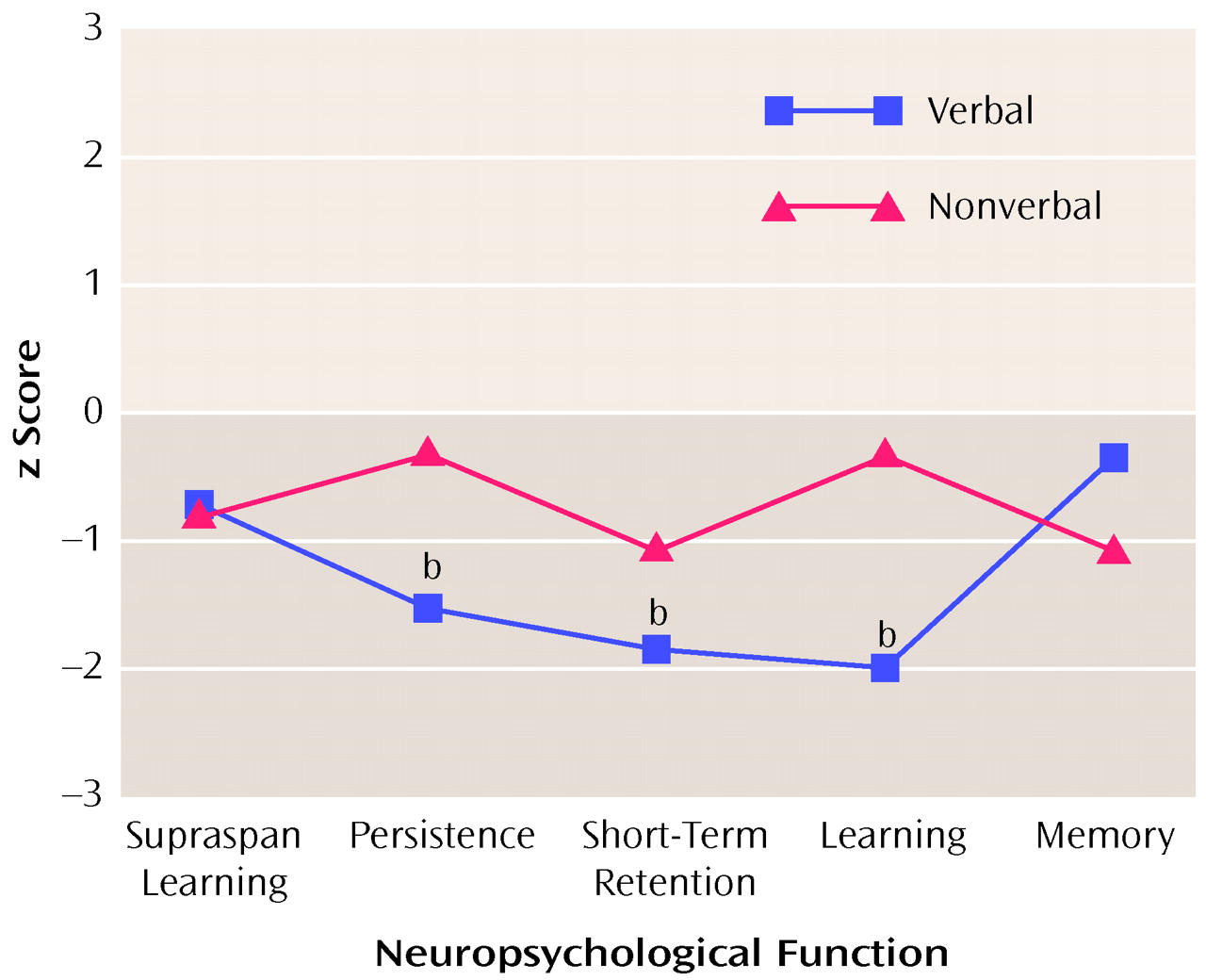
In the current study, subjects with schizotypal personality disorder showed a mild general cognitive deficit as well as a more specific deficit on measures of verbal fluency, short-term verbal retention, and verbal learning. Nonverbal forms of these tests, simpler supraspan learning, and long-term retention of newly learned information were relatively preserved. The results are consistent with our previous findings of a significant verbal learning deficit in patients with schizotypal personality disorder
(13). The findings are also supportive of the hypothesis that reduced performance on these tests is at least in part the result of a deficit in early processing (encoding) stages of verbal learning, rather than solely due to a primary deficit in organization or conceptualization.
Memory is a complex function that includes various components of attention, working memory, encoding, consolidation, storage, and retrieval
(35). The current results suggest that the breakdown in verbal learning in patients with schizotypal personality disorder may occur in the early stages of verbal memory processing. Regarding attention processes, in our previous study
(13), subjects with schizotypal personality disorder did not show a primary attention deficit. Similarly, subjects with schizotypal personality disorder in the current study did relatively well on simpler measures of supraspan learning, which involve repetition of discrete bits of information (digits, spatial location). However, as the tasks became more difficult—involving sustained behavioral output and interference or requiring further encoding of verbal information—a more specific deficit in verbal attention and memory processing became apparent. Subjects with schizotypal personality disorder showed significant deficits on verbal measures of persistence, short-term retention, and word list learning. In contrast, once information was stored, there was no specific deficit in memory retention. This replicates our previous results on the California Verbal Learning Test with two different measures of memory (the logical memory stories and visual reproduction design tasks from the Wechsler Memory Scale). In contrast, subjects did relatively well on the nonverbal versions of these measures of attention and memory.
There are several caveats to interpretation in this study. One possible limiting factor is that the verbal and nonverbal tests were not matched for level of difficulty or reliability. Without controlling for differences in these psychometric test properties, more difficult tests might be expected to show more of an effect, and less reliable tests might be expected to show less of an effect. In this study, we attempted to control for this by using standardized scores
(33), and difficulty level may have been further mediated by covarying a nonverbal measure of general ability. It is true that the results were no longer significant when estimated IQ
(19), a measure heavily weighted by vocabulary skills, was covaried from the analyses, but this is difficult to interpret. It is unclear if general deficits in verbal ability caused the reduced performance on certain verbal measures, or conversely, if inherent verbal learning deficits have resulted in deficient vocabulary.
The current results are consistent with the latter explanation or with a combination of these possibilities. A general verbal deficit alone would be expected to result in a general reduction in performance on all verbal tasks, but in the current study, verbal supraspan learning and verbal long-term memory retention skills were relatively preserved, even before IQ was taken into account. Thus, in male subjects with schizotypal personality disorder, a primary verbal learning deficit may account for reduced vocabulary, IQ scores, and verbal fluency. This raises another caveat for interpretation in that only male subjects were included in the current study to control for gender effects. Sex differences in neuropsychological test performance have been found in schizophrenic subjects and in the general population
(36). It is unknown if the current results would differ in female subjects with schizotypal personality disorder.
Finally, the results of this study must be tempered by the small study group size and resultant reduction in power. Use of small study group sizes and multiple variables can result in a failure to produce significant and potentially meaningful results. In the current study, limited power resulted in the loss of significant findings when potentially confounding variables (e.g., years of education, Beck Depression Inventory score) were covaried from the analyses, and reduced power may have accounted for other negative findings.
The pattern of cognitive deficits apparent in subjects with schizotypal personality disorder in this study is consistent with hypotheses suggesting involvement of left hemisphere frontotemporal networks in schizophrenia and schizotypal personality disorder (e.g., references
6,
37). Deficits in auditory trigram recall have been associated with left-temporal hippocampal excision
(38,
39) and frontal lobe dysfunction
(40). Reduced performance on measures of verbal fluency has been associated with frontal lobe dysfunction, especially on the left
(41). Finally, fewer words learned and reduced use of semantic clustering strategies by subjects who take the California Verbal Learning Test
(14) have been associated with left temporal lobe dysfunction
(42).
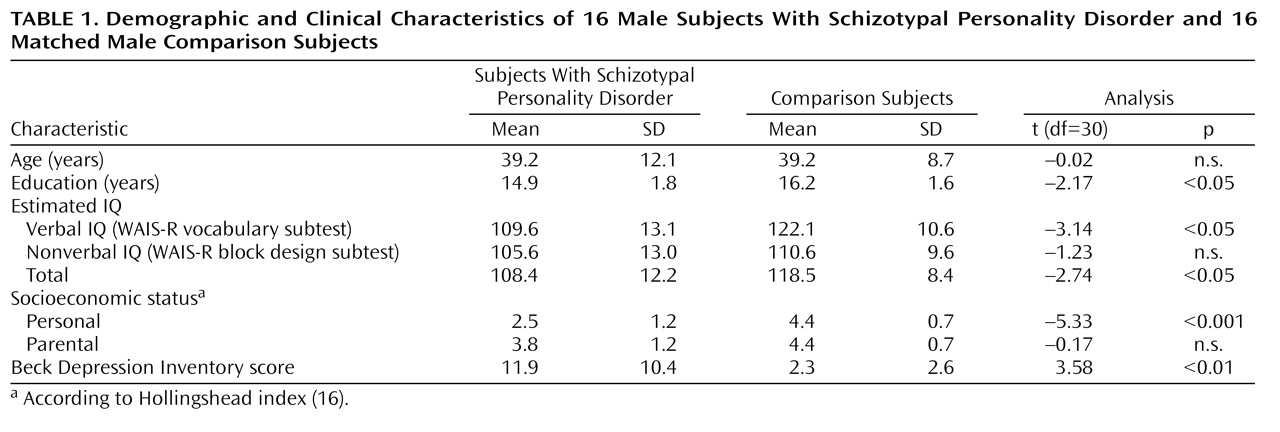
Finally, the results underscore the cognitive deficits and treatment needs of individuals with schizotypal personality disorder. Behaviorally, limitations in the early stages of verbal learning could result in problems in social, academic, and occupational performance (e.g., limited comprehension of verbal information, slow learning) and may eventually result in reduced vocabulary, verbal fluency, and IQ test scores. This may contribute to the low socioeconomic status of our subjects with schizotypal personality disorder. Selected primarily from the general population, this group has at least average intelligence and came from middle-class families, yet personal socioeconomic status was significantly lower than parental socioeconomic status, whereas this was not true in the comparison subject group. Further study of the cognitive, physiological, and structural correlates of brain function in schizotypal personality disorder populations is warranted to examine the cognitive and clinical features of this disorder, as well as to help shape our understanding of the pathophysiology of schizophrenia.