Obstetric complications have been found to be associated with schizophrenia in numerous studies involving many different types of samples, including patients with childhood-onset schizophrenia
(1,
2), siblings
(3–
5) and twins
(6–
8) discordant for schizophrenia, adopted individuals with schizophrenia
(9), offspring of schizophrenic parents
(10,
11), adult patients with schizophrenia and matched comparison subjects
(12,
13), and representative birth cohorts
(14–
16). However, questions remain as to the nature of the mechanism(s) underlying this association and whether obstetric complications are related to a particular type or course of schizophrenia.
Because genetic factors play a substantial role in schizophrenia
(19), it is also possible that a given obstetric risk factor is itself a consequence of genetic liability for the disorder, in which case the influences of genetic and obstetric factors on risk for schizophrenia would be confounded. Family studies provide a basis for examining this question: if such genotype-environment covariation exists, one would expect a higher rate of an obstetric factor in the first-degree relatives of schizophrenic probands than in the general population. While prior studies have produced conflicting evidence of fetal growth retardation as a cofamilial trait
(20,
21), we know of no study thus far that has found evidence of a higher than normal rate of fetal hypoxia in the offspring or siblings of schizophrenic patients
(18). To our knowledge, this issue has not yet been examined in regard to prenatal exposure to infection.
The association of obstetric complications and schizophrenia is one line of evidence implicating neurodevelopmental disturbances in the etiology of the disorder. Because obstetric complications suggest brain damage acquired during the pre- or perinatal period, it is reasonable to suspect that they are related to a form of schizophrenia positive for other indicators of neurodevelopmental compromise, such as delayed motor and cognitive development, poor premorbid social adjustment, and early onset. In support of this view, a meta-analysis
(22) of individual patient data from 11 different research groups that used the Lewis and Murray obstetric complication scale
(23) showed that schizophrenic patients with onsets before age 22 were about 52% more likely to have a history of obstetric complications than those with later onsets.
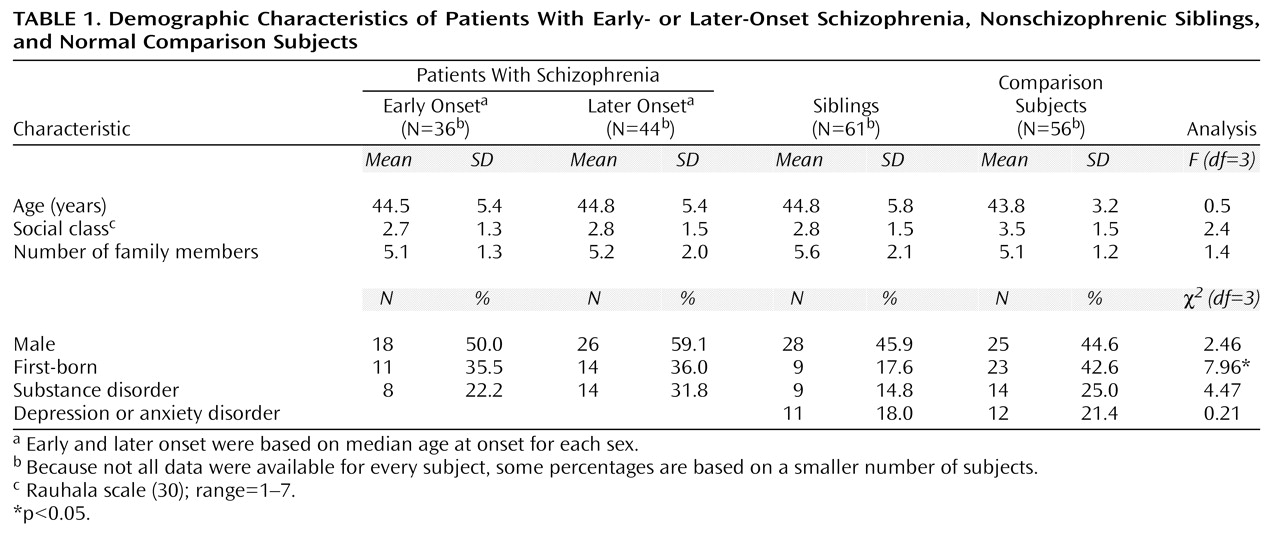
In this study we coded information from the original obstetric hospital records of 80 schizophrenic probands, ascertained so as to be representative of all such probands in a Helsinki birth cohort, along with 61 of their nonschizophrenic full siblings and 56 demographically similar comparison subjects without a personal or family history of treated psychiatric illness. On the basis of the foregoing, we hypothesized that after we controlled for prenatal infection and fetal growth retardation, complications associated with fetal hypoxia would predict increased risk for early-onset schizophrenia but would not be related to risk for later-onset schizophrenia or to sibling status.
Results
Hypoxia-Associated Obstetric Complications
In the initial regression analysis of the score on the scale for hypoxia-associated obstetric complications as a predictor of group assignment, none of the two-way interactions between hypoxia and demographic variables met the p£0.10 criterion for inclusion, nor did the main effects of gender, birth order, or mother’s age at birth. After exclusion of these variables, there was a statistically significant effect of hypoxia-associated obstetric complications (χ2=10.83, df=3, p=0.01) and nonsignificant effects of prenatal infection (χ2=5.39, df=3, p=0.15), fetal growth retardation (χ2=1.86, df=3, p=0.60), and social class (χ2=6.64, df=3, p=0.08). Contrast analysis revealed that hypoxia-associated obstetric complications significantly increased the risk for early-onset schizophrenia (χ2=9.27, df=1, p=0.002, odds ratio=2.16, 95% CI=1.31–3.53) but were not associated with later-onset schizophrenia (χ2=0.15, df=1, p=0.70, odds ratio=0.89, 95% CI=0.48–1.63) or with being an unaffected sibling of a schizophrenic patient (χ2=0.93, df=1, p=0.33, odds ratio=1.25, 95% CI=0.80–1.96). That is, the odds of early-onset schizophrenia increased by 2.16 times per hypoxia-associated obstetric complication, such that the subjects with three or more such obstetric complications were 10 times more likely to develop early-onset schizophrenia as were those with none.
Specificity of Perinatal Hypoxia
When the previous analyses were repeated with the score on the perinatal hypoxia subscale, there was a statistically significant effect of perinatal hypoxia on group assignment (χ2=10.90, df=3, p=0.01), while the effects of prenatal infection (χ2=5.44, df=3, p=0.15) and fetal growth retardation (χ2=1.52, df=3, p=0.70) remained nonsignificant. Contrast analysis showed that perinatal hypoxia predicted early-onset schizophrenia (χ2=8.06, df=1, p=0.005, odds ratio=2.58, 95% CI=1.34–4.96) but not later-onset schizophrenia (χ2=0.78, df=1, p=0.38, odds ratio=0.66, 95% CI=0.27–1.65) or unaffected sibling status (χ2=1.84, df=1, p=0.18, odds ratio=1.51, 95% CI=0.83–2.73). Conversely, prenatal hypoxia alone was not significantly associated with group outcome (χ2=5.05, df=1, p=0.17) after we controlled for prenatal infection (χ2=5.89, df=1, p=0.12) and fetal growth retardation (χ2=1.81, df=1, p=0.61).
Individual Obstetric Complications
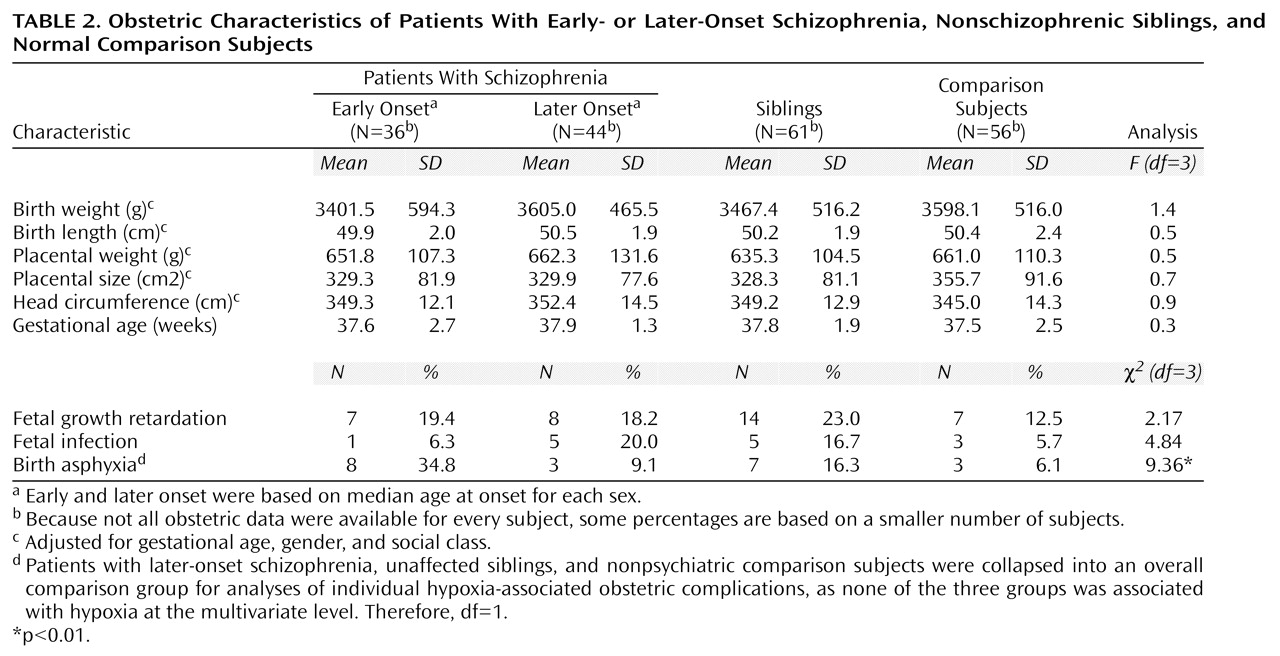
Since none of the later-onset, sibling, or normal comparison groups was associated with fetal hypoxia at the multivariate level, they were collapsed into a single comparison group for univariate contrasts. The individual hypoxia-associated obstetric complications found to be significantly more frequent among the patients with early-onset schizophrenia than among these comparison subjects were birth asphyxia (χ
2=9.36, df=1, p=0.002, odds ratio=4.55, 95% CI=1.62–12.79), prematurity (χ
2=4.10, df=1, p=0.04, odds ratio=2.13, 95% CI=1.02–4.44), and anorexia during pregnancy (χ
2=7.35, df=1, p=0.007, odds ratio=8.73, 95% CI=1.38–55.25). Placental infarcts were also more frequent among the patients with early-onset schizophrenia, but this effect did not reach statistical significance (χ
2=2.73, df=1, p=0.10, odds ratio=2.58, 95% CI=0.81–8.23). Only birth asphyxia retained a statistically significant association with early-onset schizophrenia after Bonferroni correction (
Table 2).
Association Within Families
The odds of early-onset schizophrenia increased by 2.9 times per unit increase on the hypoxia-associated obstetric complication scale within families, although this fell slightly short of statistical significance (χ2=3.06, df=1, p=0.08, odds ratio=2.86, 95% CI=0.88–9.27).
Discussion
The principal finding of this study is that hypoxia-associated obstetric complications, but not prenatal exposure to infection or fetal growth retardation, are associated with a higher than normal risk for early-onset schizophrenia. Further, there were no differences in rates of exposure to hypoxia-associated obstetric complications or other complications between patients with later-onset schizophrenia, nonschizophrenic siblings of patients, and demographically similar comparison subjects at low genetic risk for schizophrenia.
A lack of difference in siblings indicates that the occurrence of fetal hypoxia is independent of genetic risk for schizophrenia. In other words, the current results are not consistent with hypotheses holding that hypoxia-associated obstetric complications are the consequence of an inherited predisposition to schizophrenia, as these complications were not more frequent among the patients’ unaffected biological siblings—a proportion of whom are expected to carry genes associated with susceptibility to schizophrenia
(33). Rather, our findings converge with other reports of a higher incidence of obstetric complications in schizophrenia patients than in their nonpsychotic siblings
(4,
5) and with evidence that the frequency of obstetric complications does not rise with increasing genetic loading for schizophrenia
(3,
11,
20). Further, since the majority of subjects with a history of hypoxia-associated obstetric complications did not become schizophrenic, our results also exclude familial-sporadic theories in which obstetric complications are sufficient causes of schizophrenia acting independently from genetic risk
(23). It is also important that obstetric complications were not a necessary condition for developing schizophrenia or an early-onset form of schizophrenia, as 33% of the patients with schizophrenia (22% of those with early-onset schizophrenia) had a score of 0 on the scale for hypoxia-associated obstetric complications. Because liability for schizophrenia appears to conform to a polygenic mode of inheritance
(19), it is possible that the patients without hypoxia possessed a greater number of predisposing genes, such that an additional contribution of obstetric complications was not necessary for the onset of psychosis. Nonetheless, we are left with two competing etiologic models in which obstetric complications act either additively or in interaction with genetic factors in increasing liability for schizophrenia
(18). While epidemiologic methods cannot differentiate these latter two alternatives, we believe that the results of studies using quantitative indicators of genetic liability are consistent with a model of schizophrenia involving interaction of genes and obstetric complications (
20 and unpublished manuscript by Cannon et al.).
That most studies have shown schizophrenia to be associated with an aggregation of obstetric complications, rather than specific ones in isolation, could reflect the involvement of a common mechanism that can be produced by a variety of different conditions, or it could indicate involvement of multiple different mechanisms. In the present study, birth asphyxia was the only individual complication that was significantly associated with early-onset schizophrenia, a finding that is consistent with oxygen insufficiency as a primary obstetric mechanism. Also in accord with this interpretation are the results of a recent Swedish cohort study
(16), in which three categories of obstetric complications (malnutrition, prematurity, and perinatal hypoxia) that have hypoxia as a common mechanism were significantly more prevalent among a group of schizophrenic patients with early onsets. Further, the null results of two previous cohort studies are not inconsistent with a specific involvement of hypoxia. One of these studies
(14) had only eight schizophrenic patients. In the second cohort study
(15) an obstetric complication scale constructed to predict stillbirth and neonatal mortality did not predict schizophrenia. However, when individual obstetric complications were examined in this cohort, bleeding during pregnancy and low birth weight, which both imply heightened risk of hypoxia, were significantly related to schizophrenia
(34). Together, the results of the present and previous cohort studies therefore point to fetal hypoxia as an important and perhaps primary obstetric influence in the development of schizophrenia. We should note, however, that etiologic factors can be identified only tentatively with clinical epidemiologic methods and that research using direct biochemical indicators of blood oxygenation is needed to confirm the relationship between fetal hypoxia and schizophrenia.
Our findings are consistent with converging epidemiologic evidence that obstetric complications, hypoxia in particular, increase the risk for neurodevelopmental compromise and for a form of adult schizophrenia with an early onset
(22). There have also been reports of high rates of obstetric complications in childhood-onset schizophrenia, although most come from a time period when diagnostic boundaries with the adult disorder were unclear
(1,
2). In this study, by using gender-specific medians of age at onset, we were able to determine whether there was an association between obstetric complications and early-onset forms of schizophrenia in both genders, without the confound of different distributions of ages at onset in male and female patients. In fact, we found a robust association between fetal hypoxia and early-onset schizophrenia for both genders, which strengthens the hypothesis that obstetric complications relate specifically to a neurodevelopmental form of the disorder. In addition, our findings suggest that the specificity of fetal hypoxia may relate in part to its time of occurrence, since perinatal but not prenatal oxygen deprivation predicted early-onset schizophrenia. Taken together, the increasing evidence for the specificity of obstetric complications to early-onset schizophrenia suggests that data in previous studies that did not separate patients by age at onset may need to be reanalyzed.
While we can only speculate as to the mechanism(s) involved in the timing of schizophrenia onset, a prominent candidate may be the rate of cortical synaptic pruning. Some investigators
(35,
36) have proposed that schizophrenia arises because of excessive pruning, such that a reduction of neuronal synapses below a certain threshold produces psychotic symptoms. Within this framework, variations in the rate of synaptic pruning would vary the age at clinical onset of schizophrenia. It is interesting that excessive pruning is consistent with several brain abnormalities documented in schizophrenia, including prominent reductions in neuropil volume
(37), numbers of pyramidal dendritic spines
(38), and synaptic protein levels
(39). Furthermore, since synaptic pruning involves predominantly glutamatergic synapses
(36), exaggerated pruning could result in glutamate receptor hypofunction, a possible cause of striatal dopaminergic hyperactivity and psychotic symptoms in schizophrenia
(40,
41).
We propose that the neurotoxic effects of hypoxia-associated obstetric complications may reduce the amount of synaptic pruning required in late adolescence to cross the psychosis threshold, leading to an earlier onset of schizophrenia. This hypothesis is supported by the fact that temporal lobe brain regions particularly vulnerable to fetal hypoxia
(42) have also been consistently implicated in schizophrenia
(43). Thus, hippocampal neurons are reduced in number or density following fetal hypoxia
(44,
45), as they appear to be in the schizophrenic brain
(46,
47). These cellular findings are consistent with recent in vivo data from our laboratory indicating an association between fetal hypoxia and temporal gray matter deficits in both patients with schizophrenia and their unaffected siblings but not in comparison subjects at low genetic risk for schizophrenia (unpublished manuscript by Cannon et al.). Preschizophrenic individuals with a history of fetal hypoxia may therefore have a lower baseline number of neurons and synapses in temporal brain regions than those without such a history. With this reduced neuronal reserve, less further synaptic pruning would be required to cross the psychosis vulnerability threshold, resulting in earlier clinical onset in individuals with the schizophrenia genotype. Indeed, neuronal loss in temporal brain structures should decrease striatal glutamatergic efferents and enhance postsynaptic dopamine receptor sensitivity
(48). Subsequent postnatal pruning of temporal-striatal projections would then be expected to produce exaggerated mesolimbic reactivity and psychotic symptoms at an earlier age in preschizophrenic individuals positive for fetal hypoxia.
Several strengths of this study’s design merit explicit mention. Foremost is the use of original pregnancy and birth records, which can be more accurate and reliable sources of obstetric history than retrospective parental interviews
(23). In addition, the studied probands were a random and representative sample drawn from a Helsinki birth cohort and were directly interviewed according to strict diagnostic criteria. Finally, the inclusion of both unaffected siblings and a normal comparison group allowed for the evaluation of competing gene-environment etiologic models of schizophrenia.
This study was limited, however, by its inability to explore all obstetric variables that might be implicated in schizophrenia. The obstetric records used were not developed for research purposes and therefore may not have included all variables associated with schizophrenia. In addition, the statistical power was not sufficient to examine the association between obstetric complications and family history of schizophrenia, or between all obstetric complications and schizophrenia at the level of individual complications.