Dysthymic disorder is a low-grade, chronic, depressive condition that is defined and distinguished from major depressive disorder primarily on the basis of course
(1). Dysthymic disorder is common, affecting 3%–6% of individuals in the community
(2,
3) and 22%–36% of outpatients in mental health settings
(4,
5). However, given its high prevalence and the central role of chronicity in its definition, there are surprisingly few data on the naturalistic course of dysthymic disorder.
Compared to patients with episodic major depressive disorder, patients with dysthymic disorder are less severely depressed at initial examination but exhibit higher levels of symptoms in follow-ups conducted 6–30 months later
(9,
13,
14). A small proportion of adults and children with dysthymic disorder develop bipolar disorder during the course of follow-up, although the risk may not differ from that of individuals with major depressive disorder
(10,
15). Individuals with dysthymic disorder are at high risk of developing superimposed major depressive episodes
(10,
16). Although there is a high probability of recovering from a superimposed major depressive episode, there is a substantial risk of relapsing into another episode
(7–
10,
14). Comparisons of the rates of recovery from, and relapse into, major depressive episodes between patients with dysthymic disorder and patients with episodic major depressive disorder have been inconsistent
(7–
10,
14).
For chronic conditions such as dysthymic disorder, short-term follow-ups are of limited value, because it takes a number of years to determine the probability of recovery and even longer to ascertain relapse or recurrence rates. We recently reported the results of a 30-month follow-up of a cohort of 86 outpatients with early-onset dysthymic disorder, contrasting them to a “near-neighbor” comparison group of 39 patients with episodic major depressive disorder
(9). We focused on the early-onset (less than 21 years) subtype because it is the prototypical and most common form of dysthymic disorder
(1,
13,
15). We have continued to follow this study group, and in this article we report the major findings from our 5-year follow-up study. This article presents data regarding eight issues related to patients with dysthymic disorder: 1) the 5-year rate of recovery; 2) the rate of relapse among patients who had recovered; 3) the risk of developing bipolar disorder; 4) the risk of developing a first lifetime major depressive episode for patients with no prior history of major depressive disorder; 5) the rates of recovery from, and relapse into, superimposed major depressive episodes; 6) a comparison of course and outcome between patients with dysthymic disorder and patients with episodic major depressive disorder; 7) mortality and suicide attempts; and 8) the study group’s naturalistic treatment experience. In future reports, we will describe the course of social adjustment and comorbid conditions in this study group and examine the impact of a broad range of clinical, psychosocial, familial, and treatment variables on the course of dysthymic disorder.
Results
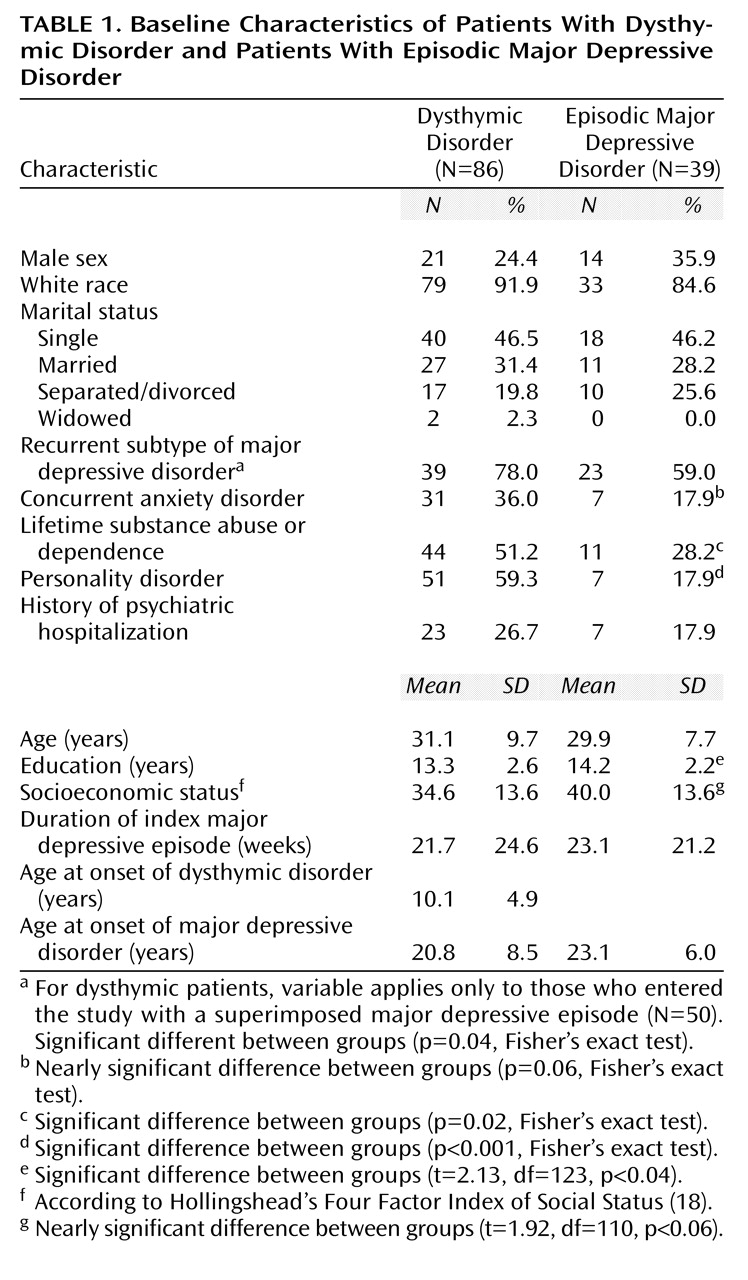
Patients’ baseline characteristics appear in
Table 1. Patients with episodic major depressive disorder had significantly more education than patients with dysthymic disorder. Significantly greater proportions of patients with dysthymic disorder than episodic major depressive disorder had a lifetime history of substance abuse or dependence and a comorbid personality disorder. Finally, patients with both dysthymic disorder and a lifetime history of major depressive disorder were significantly more likely to have recurrent major depressive episodes than were patients with episodic major depressive disorder.
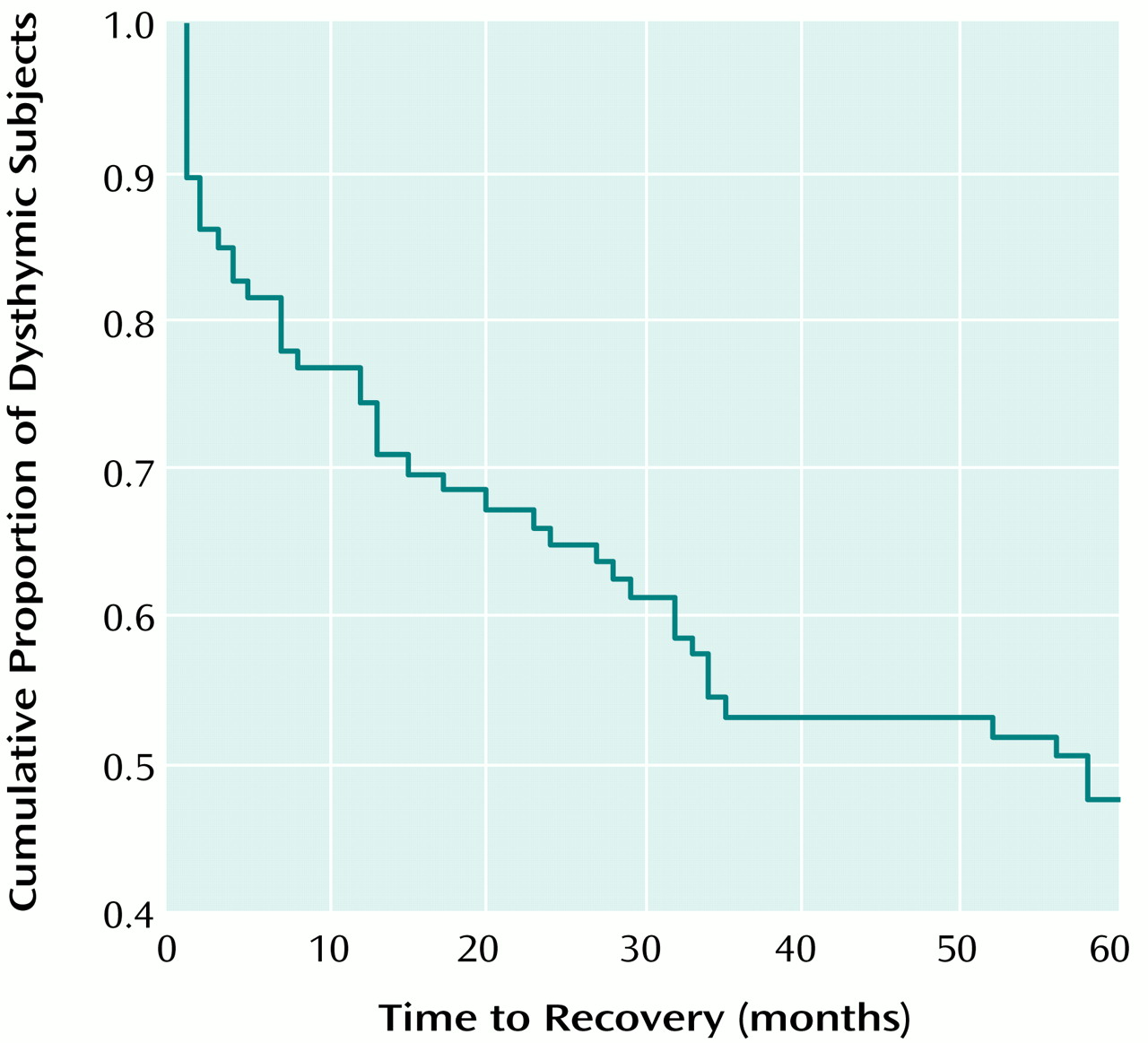
Recovery From Dysthymic Disorder
Forty-three (50.0%) of the 86 patients with dysthymic disorder recovered during the course of the follow-up. After adjustment for censored observations, the estimated 5-year recovery rate was 52.9%, with a median time to recovery of 58 months (
Figure 1). The rate of recovery was steepest in the first 7 months of follow-up, with an estimated 22.1% of the study group recovering during this period. Recoveries continued at a steady pace through month 34, with an estimated 46.5% of the study group recovering by this point. The recovery rate slowed substantially after month 35, with only an additional 7.0% of the study group recovering in the last 25 months of follow-up. The recovery rates of patients with dysthymic disorder who entered the study with and without a superimposed major depressive episode did not differ. When we used more stringent criteria for recovery (26 weeks, rather than 8), 33 (38.4%) of the 86 patients with dysthymic disorder recovered, for an estimated 5-year recovery rate of 40.0%.
Relapse Into Dysthymic Disorder
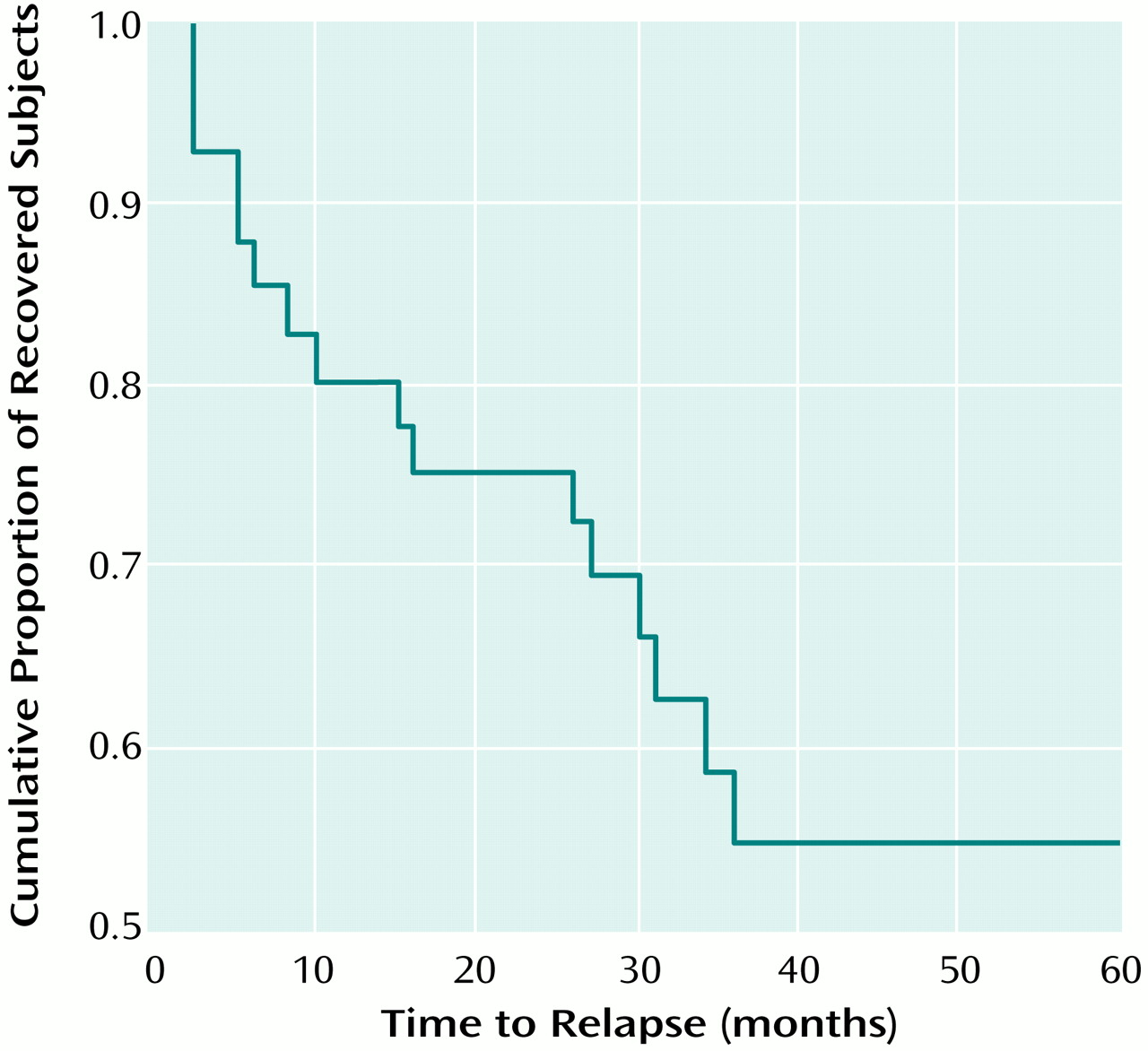
Next, we examined relapse into dysthymic disorder for the 43 patients who had recovered. Relapse was defined as meeting the full DSM-III-R criteria for dysthymic disorder. The median interval between recovery from dysthymic disorder and the last follow-up was 47 months. By definition, the relapse had to begin at least 24 months before follow-up; hence, the median risk period for relapse was 23 months. Sixteen (37.2%) of the 43 patients relapsed during this period. After adjustment for censored observations, the estimated relapse rate was 45.2% (
Figure 2). Relapse rates did not differ as a function of whether or not the patients entered the study with a superimposed major depressive episode. Finally, we examined relapse in the subset of 33 patients who met our more stringent (26-week) criteria for recovery. Requiring a longer period of recovery had little effect: 11 (33.3%) of these patients relapsed, yielding an estimated relapse rate of 39.1%.
Risk of Mania or Hypomania and First Major Depressive Episode
Five (5.8%) of the patients in the dysthymic disorder group but no patients in the episodic major depressive disorder group developed manic or hypomanic episodes during follow-up (p=0.32, Fisher’s exact test). Two patients exhibited mood-congruent psychotic features during manic episodes and were hospitalized during the first year of follow-up. Three patients had hypomanic episodes, with the onsets of the first episodes distributed evenly across the follow-up period. The onset of manic or hypomanic episodes was not associated with the initiation of antidepressant medication in any case.
Nineteen of the 86 patients in the dysthymic disorder group reported never having had a major depressive episode in their lives at the initial evaluation. During the course of the 60-month follow-up, 14 (73.7%) of these patients experienced a first lifetime major depressive episode, yielding an estimated risk of 76.9% (median time to onset=33 months). The onsets of first lifetime major depressive episode were evenly distributed across the follow-up period.
Course of Superimposed Major Depressive Episodes
We previously reported that most patients who entered the study while in the midst of a major depressive episode had recovered by the 30-month follow-up
(9). This pattern continued through the 60-month follow-up. Of the 50 patients with dysthymic disorder and a concurrent major depressive episode at entry into the study, 45 (90%) recovered from the major depressive episode, yielding an estimated recovery rate of 92.9% (median time to recovery=4 months). Two of the 39 patients with episodic major depression were partially recovered when they entered the study. All of the other 37 patients with episodic major depression recovered by 60 months (median time to recovery=3 months). Recovery rates did not differ significantly between groups.
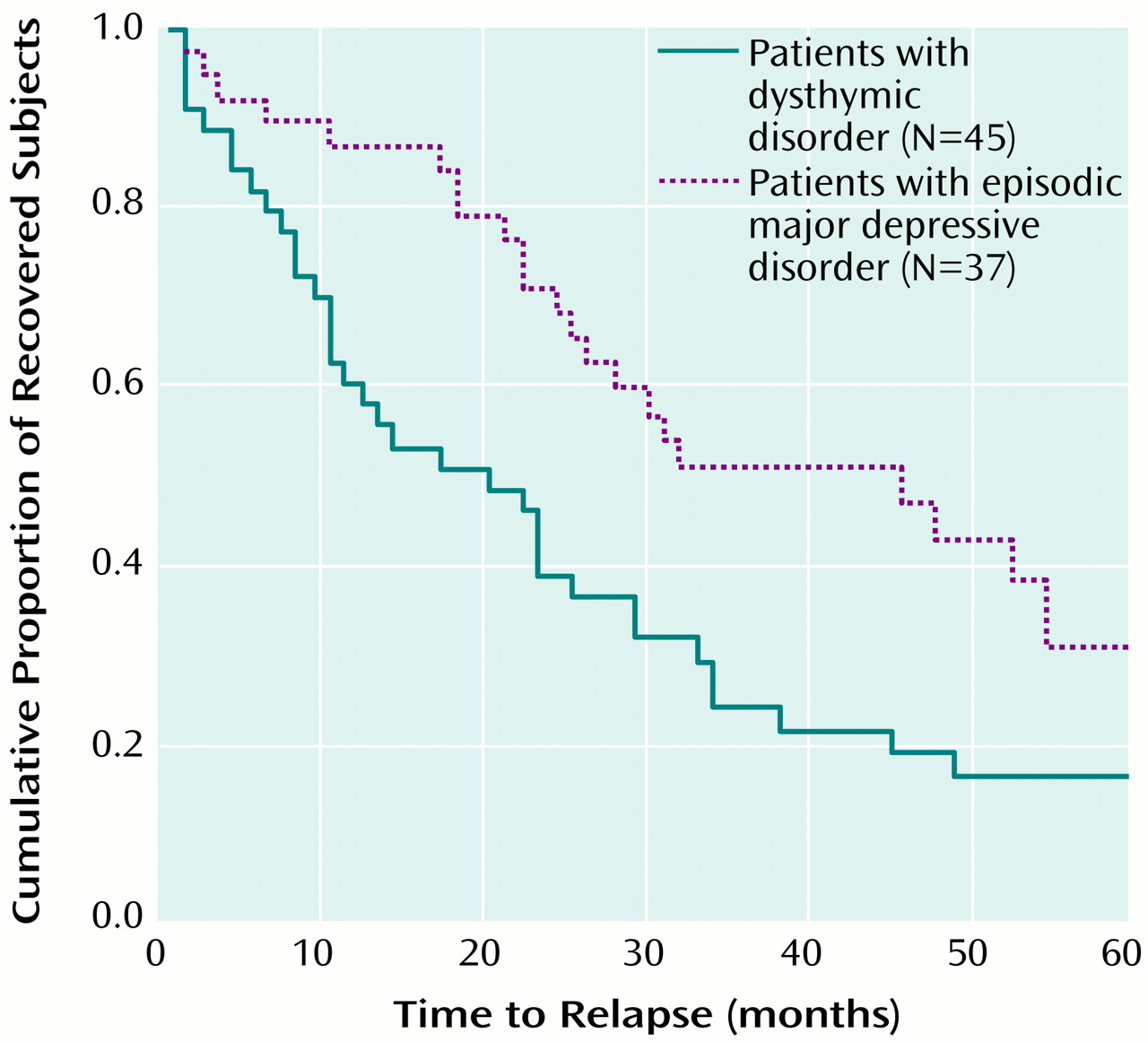
The median period of risk for relapse into another major depressive episode (i.e., the interval between recovery from the index major depressive episode and the last follow-up) was 55 months for both the dysthymic disorder group and the episodic major depressive disorder group. Among the 45 patients with dysthymic disorder who recovered from their index major depressive episode, 35 (77.8%) relapsed by the 60-month follow-up, for an estimated relapse rate of 84.4% (median time to relapse=21 months) (
Figure 3). Of the 37 patients with episodic major depressive disorder, 22 (59.5%) relapsed, for an estimated relapse rate of 70.2% (median time to relapse=47 months). The relapse rate was significantly higher among the patients with dysthymic disorder than among the patients with episodic major depressive disorder (log rank=6.72, df=1, p<0.01).
Although the numbers were small, we also examined the rates of a second prospectively observed recovery from, and relapse into, a major depressive episode. Among the 35 patients with dysthymic disorder and a superimposed major depressive episode at study entry who recovered and then relapsed into another major depressive episode, 27 (77.1%) recovered for a second time, for an estimated recovery rate of 88.6% (median time to recovery=5 months). Among the 22 patients with episodic major depressive disorder who recovered and then relapsed into another major depressive episode, 20 (90.9%) recovered for the second time, for an estimated recovery rate of 100% (median time to recovery=3 months). This difference was not quite significant (log rank=3.46, df=1, p=0.06).
Of the 27 patients with dysthymic disorder who recovered from a major depressive episode for the second time, 20 (74.1%) experienced another relapse, for an estimated relapse rate of 93.2% (median time to relapse=9 months). Of the 20 patients with episodic major depressive disorder who recovered from a major depressive episode for the second time, nine (45.0%) experienced another relapse, for an estimated relapse rate of 67.1% (median time to relapse=30 months) (log rank=8.52, df=1, p<0.004).
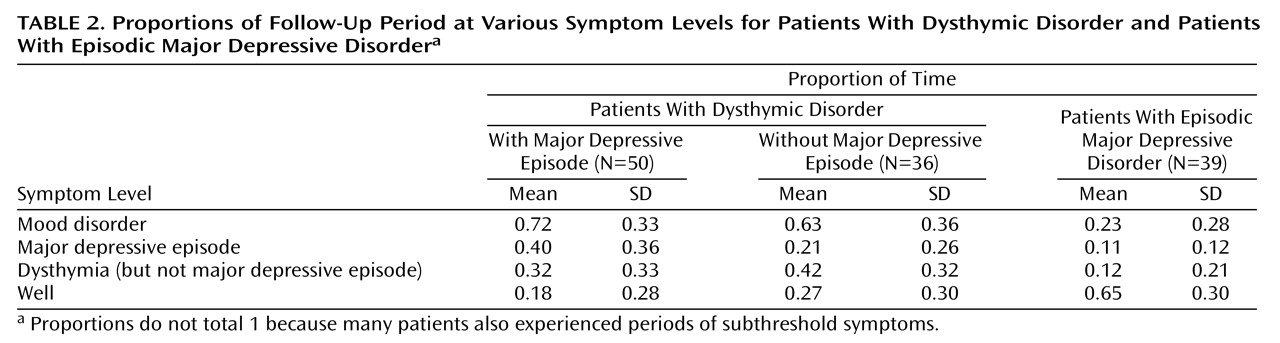
Proportion of Follow-Up Period at Various Symptom Levels
To summarize the patients’ course across the entire follow-up period, we computed the proportion of time that they met the full symptom criteria for a mood disorder, major depressive disorder, or dysthymic disorder (but no superimposed major depressive episode) and were completely recovered from all mood disorders (
Table 2). Patients with dysthymic disorder who entered the study with a superimposed major depressive episode, patients with dysthymic disorder who did not have a superimposed major depressive episode at study entry, and patients with episodic major depressive disorder differed significantly on the proportions of the follow-up period they spent meeting the symptom criteria for a mood disorder (F=27.14, df=2, 122, p<0.001), major depressive disorder (F=12.69, df=2, 122, p<0.001), dysthymic disorder (F=10.04, df=2, 122, p<0.001), and on the time spent recovering from all mood disorders (F=29.58, df=2, 122, p<0.001). Pairwise comparisons indicated that both subgroups of patients with dysthymic disorder spent a significantly greater proportion of the follow-up period with a mood disorder or meeting the symptom criteria for dysthymic disorder and significantly less of the follow-up period recovered from all mood disorders than did patients with episodic major depressive disorder. Patients with dysthymic disorder who entered the study in a superimposed major depressive episode also spent a significantly greater proportion of the follow-up period in a major depressive episode than did patients with dysthymic disorder without superimposed major depressive episodes at entry into the study and patients with episodic major depressive disorder.
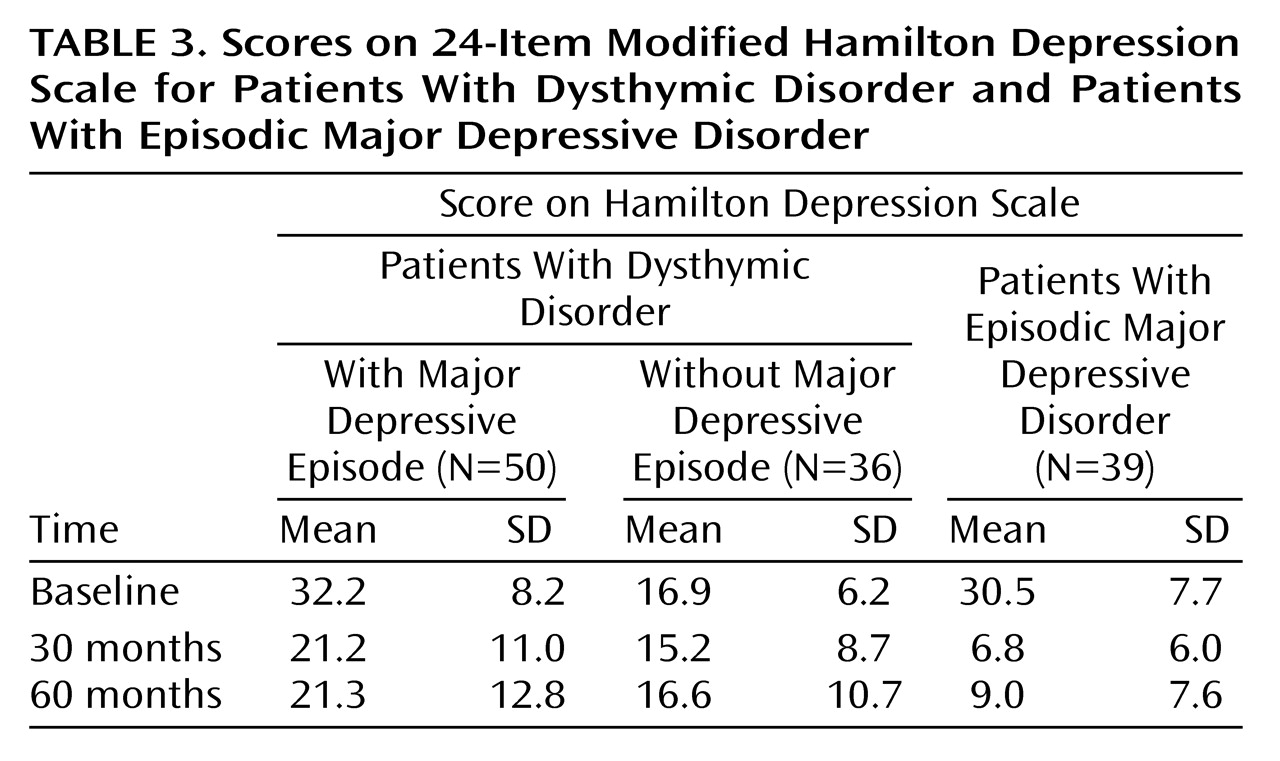
Modified Hamilton Depression Scale
The three groups’ scores on the modified Hamilton depression scale at baseline and at the 30- and 60-month assessments appear in
Table 3. There were significant effects for group (F=28.64, df=2, 139, p<0.001), time (F=94.66, df=2, 218, p<0.001), and interaction of group and time (F=25.24, df=4, 218, p<0.001). Pairwise comparisons indicated that patients with dysthymic disorder with a superimposed major depressive episode and patients with episodic major depressive disorder both entered the study with significantly higher scores on the modified Hamilton depression scale than did patients with dysthymic disorder without a superimposed major depressive episode. At 30 months, scores on the modified Hamilton depression scale for patients with dysthymic disorder with a superimposed major depressive episode at baseline and patients with episodic major depressive disorder had decreased significantly, whereas scores on the modified Hamilton depression scale for patients with dysthymic disorder without a superimposed major depressive episode at baseline were unchanged. Although the difference between the two dysthymic disorder groups was no longer significant at 30 months, both dysthymic disorder groups were significantly more depressed than the patients with episodic major depressive disorder. Finally, none of the groups exhibited significant changes in scores on the modified Hamilton depression scale between the 30- and 60-month follow-ups. At 60 months, the two dysthymic disorder groups did not differ on scores on the modified Hamilton depression scale, but both continued to experience significantly higher levels of depression than did patients with episodic major depressive disorder.
Mortality and Suicide Attempts
Three patients died during the 60-month follow-up period. Two patients with episodic major depressive disorder died of natural causes, and one patient with dysthymic disorder committed suicide. During the follow-up, suicide attempts were made by 19.0% (16 of 84—data were missing for two subjects) of the patients with dysthymic disorder but none of the 37 patients with episodic major depressive disorder (p=0.003, Fisher’s exact test). The patients with dysthymic disorder with and without superimposed major depressive episodes at entry into the study did not differ on numbers of suicide attempts.
Hospitalization
During the follow-up, 22.4% (19 of 85) of the patients with dysthymic disorder had one or more psychiatric hospitalizations compared to 2.7% (one of 37) of the patients with episodic major depressive disorder (p=0.007, Fisher’s exact test). Patients with dysthymic disorder with and without superimposed major depressive episodes at entry into the study did not differ on the number of hospitalizations.
Outpatient Treatment
At the end of the first year of follow-up, 50.0% (43 of 86) of the patients with dysthymic disorder were receiving outpatient mental health treatment. This proportion declined slightly over the follow-up period, with 45.3% (N=39) receiving outpatient treatment at the end of the third year and 40.7% (N=35) receiving treatment at the end of the fifth year of follow-up. Only a minority of the patients received a definitely or probably adequate level of antidepressant medication: 25.6% (N=22), 24.4% (N=21), and 30.2% (N=26) at the end of years 1, 3, and 5, respectively. The number of patients receiving psychotherapy on a weekly or biweekly basis declined gradually over the course of the follow-up, from 38.4% (N=33) at the end of the first year to 27.9% (N=24) at the end of the third year to 23.3% (N=20) at the end of the fifth year.
To analyze these data more formally, we compared the groups’ mean treatment scores for antidepressant medication and psychotherapy for each 12-month interval throughout the follow-up. For medication, there was a significant effect for group, with the patients with dysthymic disorder (mean=0.72, SD=0.85) receiving significantly higher levels of medication than the patients with episodic major depressive disorder (mean=0.27, SD=0.57) (F=8.63, df=1, 109, p=0.004). Neither the main effect for time nor the interaction of group and time was significant. For psychotherapy, the main effect for group was marginally significant, with the patients with dysthymic disorder (mean=1.06, SD=0.93) receiving more psychotherapy than the patients with episodic major depressive disorder (mean=0.72, SD=0.76) (F=3.90, df=1, 109, p=0.05). In addition, there was a significant main effect for time (F=9.73, df=4, 436, p<0.001), reflecting a linear decrease in the mean level of psychotherapy in both groups over the course of the follow-up. The interaction of group and time was not significant. The subgroups of patients with dysthymic disorder with and without superimposed major depressive episodes at entry into the study did not differ on levels of pharmacotherapy and psychotherapy during the follow-up period.
Discussion
This article describes the 5-year course and outcome of early-onset dysthymic disorder. To our knowledge, this is the longest prospective, naturalistic follow-up study of adults with dysthymic disorder in the literature. It extends our previous 30-month follow-up
(9) by providing the first published data on the risk of relapse in dysthymic disorder and provides an additional 30 months of data on recovery, outcome, the risk of bipolar disorder and first major depressive episode, the course of superimposed major depressive episodes, suicidality, and treatment.
The probability of recovery from dysthymic disorder increased slowly throughout the first 35 months of follow-up and then leveled off. Even after 5 years, only about half of the patients had recovered, according to the liberal criteria of the Longitudinal Interval Follow-Up Evaluation of at least 8 consecutive weeks with minimal or no symptoms. When we used more stringent criteria for recovery (26 weeks), the estimated recovery rate was 40.0% after 5 years.
Although we had only a median of 23 months to observe relapse, an estimated 45.2% of the study group relapsed, meeting the full criteria for dysthymic disorder. This is probably an underestimate, because several additional patients experienced a recurrence of symptoms that appeared to be persistent but had not lasted the required 24 months at the time of follow-up. The high relapse rate is not attributable to brief remissions, because requiring a recovery of 6 (rather than 2) months did not produce a substantially lower relapse rate. These data indicate that patients who recover from dysthymic disorder are at high risk for relapse and highlight the importance of developing effective strategies for long-term treatment
(29,
30).
We contrasted the group with dysthymic disorder with a “near-neighbor” comparison group of patients with episodic major depressive disorder. The data indicated that although dysthymic disorder often presents with only mild to moderate symptoms, from a longitudinal perspective, it is more severe than episodic major depressive disorder, at least in outpatient settings, and constitutes a significant public health problem. Over the course of the 5-year follow-up, the patients with dysthymic disorder spent approximately 70% of the time meeting the criteria for a mood disorder compared to less than 25% of the time for the patients with episodic major depressive disorder. Consistent with these findings, the patients with dysthymic disorder exhibited clinically significant levels of depression on the modified Hamilton depression scale at both the 30- and 60-month follow-ups—differing significantly from the patients with episodic major depressive disorder. In addition, a significantly greater proportion of the patients with dysthymic disorder than the patients with episodic major depressive disorder attempted suicide and had psychiatric hospitalizations during the follow-up period. By the same token, these data indicate that purely episodic forms of major depressive disorder also exhibit a consistent, albeit more benign, course.
Another important finding was that an estimated 73.7% of the patients with dysthymic disorder who reported never experiencing a major depressive episode in the initial evaluation developed a first lifetime major depressive episode within 5 years of follow-up. Because 77.9% (67 of 86) of the dysthymic disorder group had already experienced a superimposed major depressive episode by the beginning of the study, 94.2% (81 of 86) of the group had at least one lifetime major depressive episode by the end of the 5-year follow-up. These data extend our previous finding that 42% of the patients with “pure” dysthymic disorder developed a first lifetime major depressive episode within 30 months of follow-up
(9) and suggest that almost all individuals with dysthymic disorder will eventually experience a major depressive episode at some point in their lives. At the same time, we found few differences in course and outcome between patients with dysthymic disorder with and without superimposed major depressive episodes at entry into the study. Taken together, these data indicate that dysthymic disorder and “double depression”
(8) should probably be conceptualized as the same condition viewed at different points in their course. Because double depression and chronic major depressive disorder are also similar with regard to most clinical characteristics, family history, and pharmacological response
(31), dysthymic disorder may be part of an even larger group of chronic depressive conditions with similar features and correlates.
A small number of patients with dysthymic disorder developed bipolar disorder during follow-up. Manias tended to develop early, whereas hypomanias were evenly distributed across the follow-up period. Although the proportion of patients developing bipolar disorder was higher in the dysthymic disorder group than in the episodic major depressive disorder group, the difference was not statistically significant.
Given the high comorbidity between dysthymic disorder and major depressive disorder, knowledge of the course of major depressive episodes in dysthymic disorder is important. We found that almost all patients with dysthymic disorder recovered from superimposed major depressive episodes, but most relapsed quickly. We extended the findings from our previous report
(9) to include second prospectively observed recoveries from, and relapses into, major depressive episodes. Rates of recovery from the first and second major depressive episodes were similar; however, second relapses tended to be faster than first relapses. This may be because of a progressive shortening of interepisode intervals over time, or it may reflect a differential sieve process, with the patients who had already relapsed once during follow-up comprising a subgroup with a particularly high propensity for relapse. Compared to the patients with episodic major depressive disorder, the patients with dysthymic disorder recovered nonsignificantly more slowly from major depressive episodes but relapsed significantly more quickly. It is notable that these findings were evident for both the first and second prospectively observed major depressive episodes.
Only a minority of the patients with dysthymic disorder were in treatment at any given time during the follow-up. Approximately 25%–30% of the dysthymic disorder group received adequate or probably adequate pharmacotherapy. This proportion was stable across the follow-up, although without further analyses, it is unclear whether this is because the same patients were taking medication for extended periods or because the number of patients dropping out of treatment was similar to the number reentering treatment in any given period. The number of patients with dysthymic disorder receiving weekly or biweekly psychotherapy declined over time. Further analyses are necessary to determine whether the patients terminated psychotherapy because they had remitted, were discouraged by a lack of improvement, or for other reasons (e.g., financial or insurance constraints). It is interesting that the patients with dysthymic disorder received significantly more treatment than did the patients with episodic major depressive disorder across the follow-up period. Thus, treatment probably cannot account for the poorer course and outcome of the dysthymic disorder group. Rather, it is likely that the patients with dysthymic disorder received higher levels of treatment because of their continuing symptoms.
This study has a number of strengths, including a larger study group and a longer follow-up period than those that have been previously reported, repeated follow-up evaluations using semistructured clinical interviews, comparisons of patients with dysthymic disorder with and without a superimposed major depressive episode, and the use of a near-neighbor comparison group of patients with episodic major depressive disorder. However, the study also has several limitations. First, we asked patients to report after relatively lengthy follow-up intervals. Although long follow-up intervals are appropriate for chronic conditions, it would be prudent to regard the data on patient recovery and relapse as approximations. Second, the study group was limited to patients with early-onset dysthymic disorder; hence, the results may not apply to late-onset cases. Finally, our treatment data were limited in that we could not assess the quality of psychotherapy and patients’ compliance with treatment. We are continuing to follow up this study group at 7.5 and 10 years after entry into the study to provide data on the long-term course and outcome of dysthymic disorder.