The familial nature of attention deficit hyperactivity disorder (ADHD) has been recognized since the turn of the last century
(1). Subsequent twin studies from several countries have estimated the heritability of ADHD to be between 0.6 and 0.9 (reviewed in references
2,
3). Despite the overwhelming evidence for genetic influences on ADHD, there is controversy regarding how to conceptualize ADHD symptoms in genetic studies (for example, references
2,
4,
5). Because of high rates of comorbidity and concerns about the validity of DSM-IV ADHD subtypes
(2,
3,
6), it is possible that alternative ways of conceptualizing the ADHD phenotype may identify more “pure” phenotypes.
In previous studies we have attempted to address whether DSM-IV ADHD subtypes are an appropriate nosology for ADHD by applying clustering techniques to population- and family-based data on the prevalence of individual ADHD symptoms
(5,
10,
11). One such technique is latent-class analysis, which assumes categorical rather than continuous latent variables (“classes”)
(12). In this approach the observed pattern of symptom clustering is assumed to be explained by the existence of discrete groups with different symptom profiles. This approach has three specific advantages for analysis of the nature of ADHD. First, if there are multiple independent types of ADHD, then the patterns of endorsement of the 18 DSM-IV ADHD symptoms associated with each independent ADHD subtype will be grouped together within independent classes. Second, the probability of endorsement of individual symptoms given membership in a latent class is quantified. If the underlying nature of the phenotype is a continuum of problems with inattention, hyperactivity/impulsivity, or both, then symptom endorsement profiles of the observed classes will reflect differences in severity or frequency of the reporting of symptoms only. Finally, on the basis of the most likely class, individuals can be assigned to individual latent classes to allow the identification of specific groups for further analyses, such as analyses of family clustering. With this approach we have been able to demonstrate that latent class analysis results in a limited number of classes of ADHD symptoms in both general population twin
(5) and family-based
(10) samples. The observed latent classes to some extent recapitulate the DSM-IV categorization because classes resembling DSM-IV inattentive, hyperactive/impulsive, and combined subtypes of ADHD are identified. However, these classes do not contain all individuals with DSM-IV ADHD and also include many individuals who do not meet DSM-IV criteria for ADHD. More recently, we have been able to demonstrate that the majority of comorbid problems associated with ADHD are found in a single latent class corresponding to, but defined somewhat more broadly than, the DSM-IV combined subtype of ADHD
(11). Our initial conclusion about the underlying nature of ADHD on the basis of these analyses was that there were three continua representing domains of problems with inattention, problems of hyperactivity/impulsivity, and combined problems
(5). However, the observed concordance for same-class membership between monozygotic and dizygotic twins is also compatible with there being discreet clinically significant subtypes that have high heritability in each of these domains
(10).
Results
The data consist of parent reports on 4,036 adolescent female twins in 1,127 monozygotic pairs and 891 dizygotic pairs identified through birth records of the state of Missouri. African Americans constituted 13.3% of the sample. The majority of the sample was European American; less than 1% were Hispanic, Asian American, Native American, or of other self-identified ancestries. The average age of the twins at time of the parental interview was 14.9 years (SD=2.7).
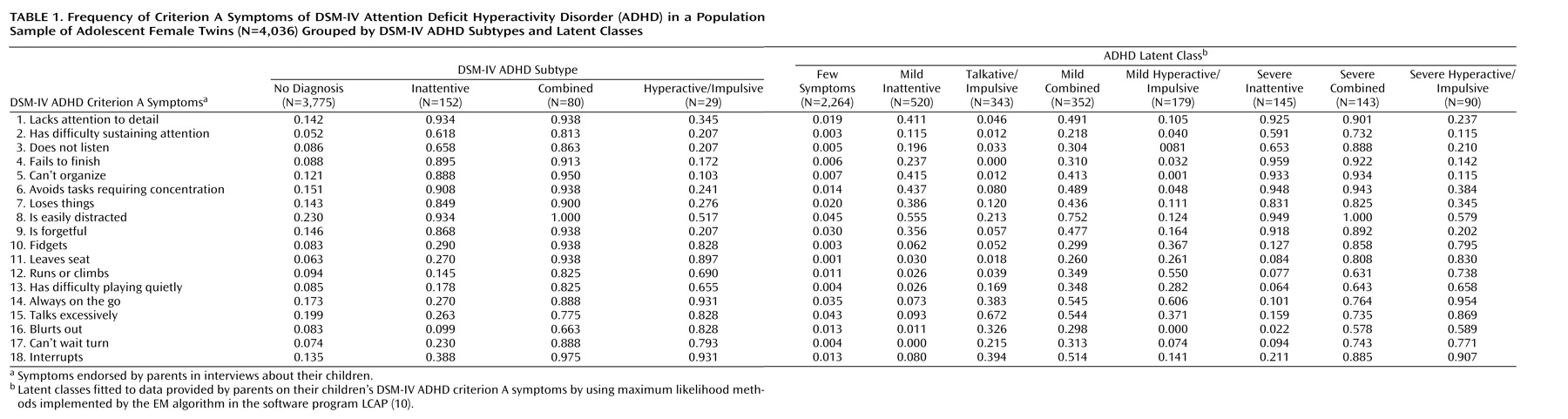
Table 1 presents the frequencies of the DSM-IV and latent-class ADHD subtypes as well as the frequencies with which parents endorsed the DSM-IV inattention and hyperactive/impulsive symptoms for their children. The prevalences of DSM-IV inattentive, combined, and hyperactive/impulsive ADHD subtypes were 3.8%, 2.0%, and 0.7%, respectively. Latent-class models of one to 10 classes were fitted, with significant improvement in likelihood ratios as additional classes were added (data available on request). Estimated prevalences of latent classes became stable while progressing from an eight- to a nine-class solution, with additional classes representing less than 1% of the study population. Similarly, few twins were reassigned to different classes when the number of classes increased from an eight- to a nine-class solution. Consequently, the eight-class solution was selected as the best-fitting model for further analyses. The class prevalences and the endorsement frequencies of inattentive and hyperactive/impulsive symptoms are remarkably similar to those in our previous latent-class analysis, which included a smaller sample
(5). There are classes that have mild or marked endorsement frequencies of inattentive symptoms (mild inattentive and severe inattentive classes), hyperactive/impulsive symptoms (mild hyperactive-impulsive and severe hyperactive-impulsive classes), or both types of symptoms (mild combined and severe combined classes). The talkative/impulsive class was characterized by frequent endorsement of the symptom of “talks excessively” (67.2%) but relatively low levels of endorsement of inattentive and hyperactive ADHD symptoms. The “few symptoms” class was characterized by infrequent (<5%) endorsement of all symptoms.
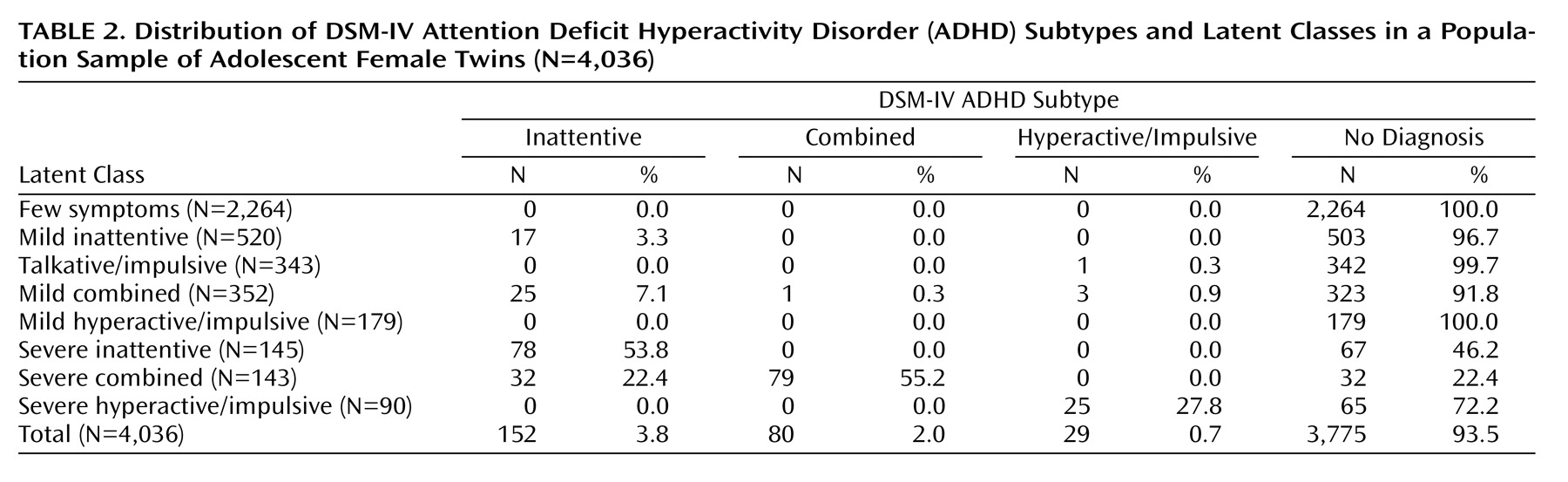
Table 2 displays the cross-tabulation of DSM-IV and latent-class ADHD subtypes. As in our previous latent-class analysis with a smaller sample
(5), there was almost complete assignment of the DSM-IV combined subtype to the severe combined latent class (79 of 80 subjects with the DSM-IV ADHD combined subtype). However, approximately 21% (N=32 of 152) of those diagnosed with the DSM-IV inattentive subtype were also assigned to this latent class as were 32 individuals with no DSM-IV ADHD diagnosis (0.8% of 3,775). About 63% of DSM-IV inattention subtype diagnoses were assigned to either mild or severe inattention classes, and about 37% were assigned to either mild or severe combined classes. About 86% of the subjects with the DSM-IV hyperactive/impulsive subtype were assigned to the severe hyperactive/impulsive latent class, and 14% were assigned to other latent classes. In contrast to the severe combined latent class, which included subjects with both the DSM-IV inattentive and the DSM-IV combined ADHD subtypes, the severe inattentive latent class contained only subjects with the DSM-IV inattentive subtype and the severe hyperactive/impulsive latent class contained only subjects with the DSM-IV hyperactive/impulsive subtype. The three severe latent classes also contained many individuals with no DSM-IV ADHD diagnosis. Individuals with no DSM-IV ADHD diagnosis constituted 46% of the subjects in the severe inattentive latent class, 22% in the severe combined class, and 72% in the severe hyperactive/impulsive class. For the severe inattentive and the severe hyperactive/impulsive latent classes, there were no significant differences in the average number of endorsed inattentive and hyperactive/impulsive symptoms or in probability of class assignment for class members with and without a DSM-IV ADHD diagnosis. Compared with the severe combined latent class members without an ADHD diagnosis, class members with a DSM-IV ADHD diagnosis had somewhat more inattentive symptoms (a mean of 8.3 [SD=0.9] versus 7.4 [SD=1.1]) (Wilcoxon-Mann-Whitney χ
2=16.9, df=1, p<0.001) and a slightly higher probability of class assignment (0.95 versus 0.90) (Wilcoxon-Mann-Whitney χ
2=15.6, df=1, p<0.001).
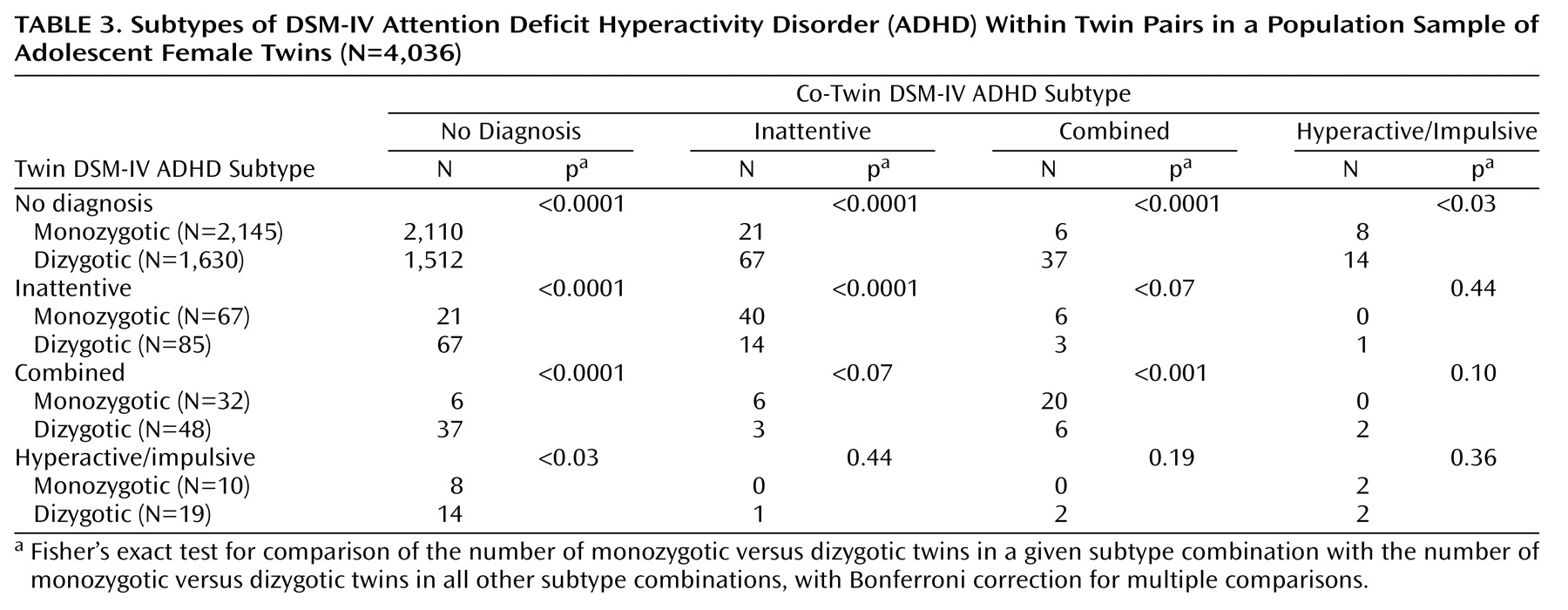
In its most general form, the familiality of DSM-IV ADHD can be estimated by comparing the concordance of sibling pairs for the presence or absence of any ADHD subtype. Since this study included a population sample, each subject with ADHD was treated as a proband in this analysis. Sixty-eight percent of monozygotic twin pairs and 22% of dizygotic twin pairs were concordant for DSM-IV ADHD of any subtype (
Table 3). These proportions represent an odds ratio of having a second sibling with ADHD of 127.5 (95% CI=75.6–215.0, p<0.001, Fisher’s exact test) and 3.7 (95% CI=2.4–5.6, p<0.001, Fisher’s exact test) for monozygotic and dizygotic siblings, respectively. Familiality was also significant when DSM-IV subtypes were individually analyzed. The odds ratios of having a sibling with any type of DSM-IV ADHD were 73.9 (95% CI=41.6–131.1, p<0.001, Fisher’s exact test) and 3.1 (95% CI=1.8–5.4, p<0.001, Fisher’s exact test), for monozygotic and dizygotic siblings, respectively, for the inattentive subtype; 111.7 (95% CI=44.8–278.6, p<0.001, Fisher’s exact test) and 3.4 (95% CI=1.7–6.7, p<0.001, Fisher’s exact test), respectively, for the combined subtype; and 5.0 (95% CI=1.1–23.8, p<0.02, Fisher’s exact test) and 3.9 (95% CI=1.4–11.1, p<0.005, Fisher’s exact test), respectively, for the hyperactive/impulsive subtype.
The hypothesis of a lack of familial specificity of DSM-IV subtypes can be tested by comparing the concordance of sibling pairs for ADHD subtype. In more than 75% of the instances when an affected monozygotic twin had an affected co-twin, the twins had the same DSM-IV ADHD subtype. Co-twins of a twin with the inattentive subtype were significantly more likely to have the inattentive and the combined subtypes (p<0.0001, Fisher’s exact test, for both comparisons) but not the hyperactive/impulsive subtype (p=0.99, Fisher’s exact test). Similarly, co-twins of a twin with the combined subtype were significantly more likely to have the combined subtype (p<0.0001, Fisher’s exact test) and the inattentive subtype (p<0.001, Fisher’s exact test) but not the hyperactive/impulsive subtype (p<0.99, Fisher’s exact test). Monozygotic twins with the hyperactive/impulsive subtype were more likely to have a co-twin with the hyperactive/impulsive subtype (p<0.0001, Fisher’s exact test) but not the inattentive or the combined subtype (p=0.14 and p=0.54, respectively, Fisher’s exact test). For dizygotic pairs, concordance for same subtype was significantly more likely for the inattentive DSM-IV subtype (p<0.005, Fisher’s exact test), but there was no significant concordance for the combined or the hyperactive/impulsive subtypes (p=0.11 and p=0.14, respectively, Fisher’s exact test). These findings are compatible with a lack of family specificity for the DSM-IV combined and inattentive subtypes and suggest that the hyperactive/impulsive subtype may be independent of the other two subtypes.
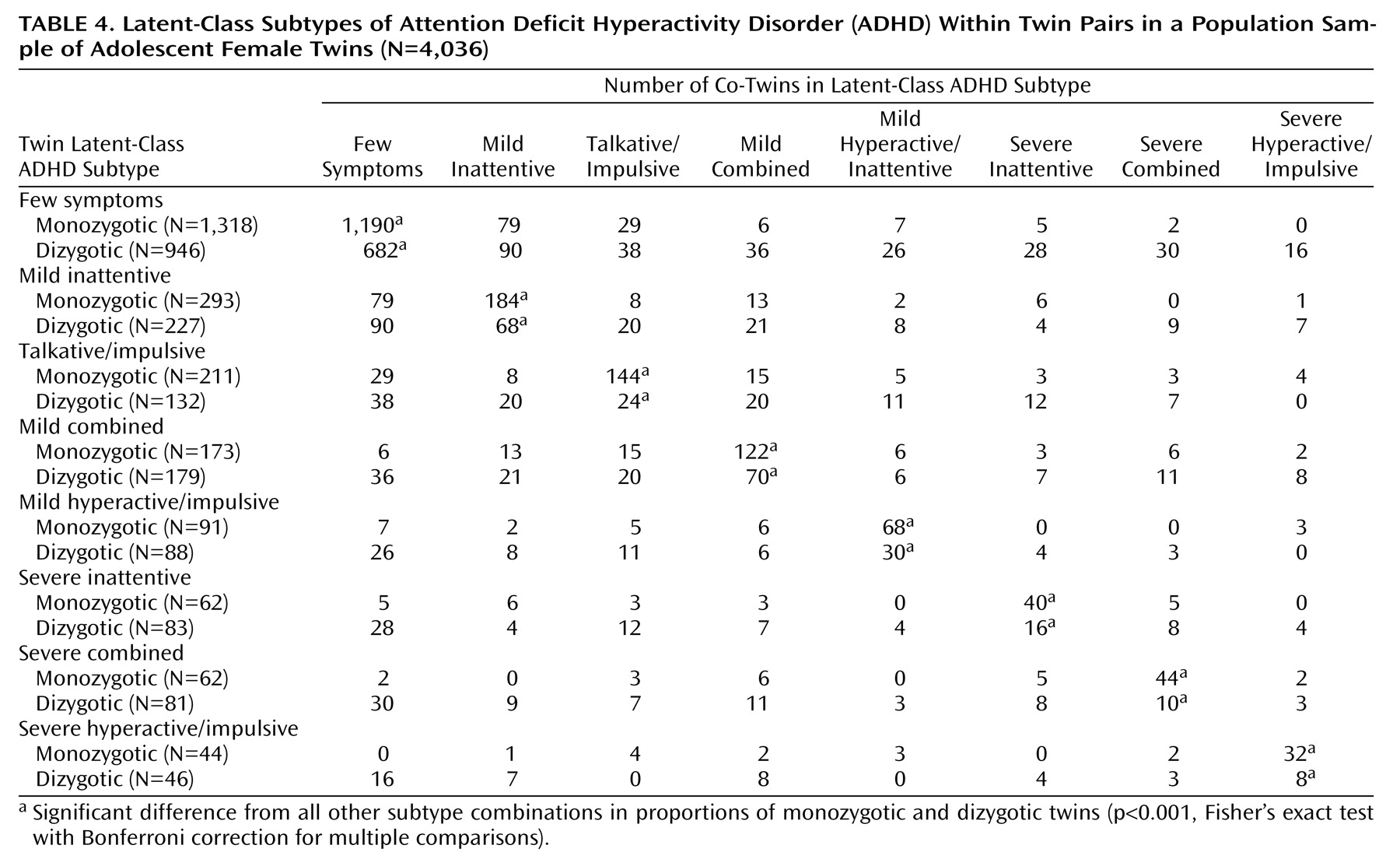
The hypothesis that latent-class ADHD subtypes are family specific can also be tested by comparing the concordance of sibling pairs for the same or different latent-class ADHD subtypes. The probability that co-twins are of the same latent-class ADHD subtype ranged from 63% to 90% for monozygotic pairs (range of odds ratios=28.7–488.4) and from 12% to 72% for dizygotic pairs (range of odds ratios=3.2–14.6) (
Table 4). The concordance rates were highly significant (p≤0.001, Fisher’s exact test) for all monozygotic and dizygotic same-class comparisons (analyses not shown but easily computable from the data in
Table 4). There were no significant positive associations for cross-class pairs for either monozygotic or dizygotic twins (p>0.1, Fisher’s exact test). These findings are compatible with a high level of family specificity for all of the latent-class ADHD subtypes.
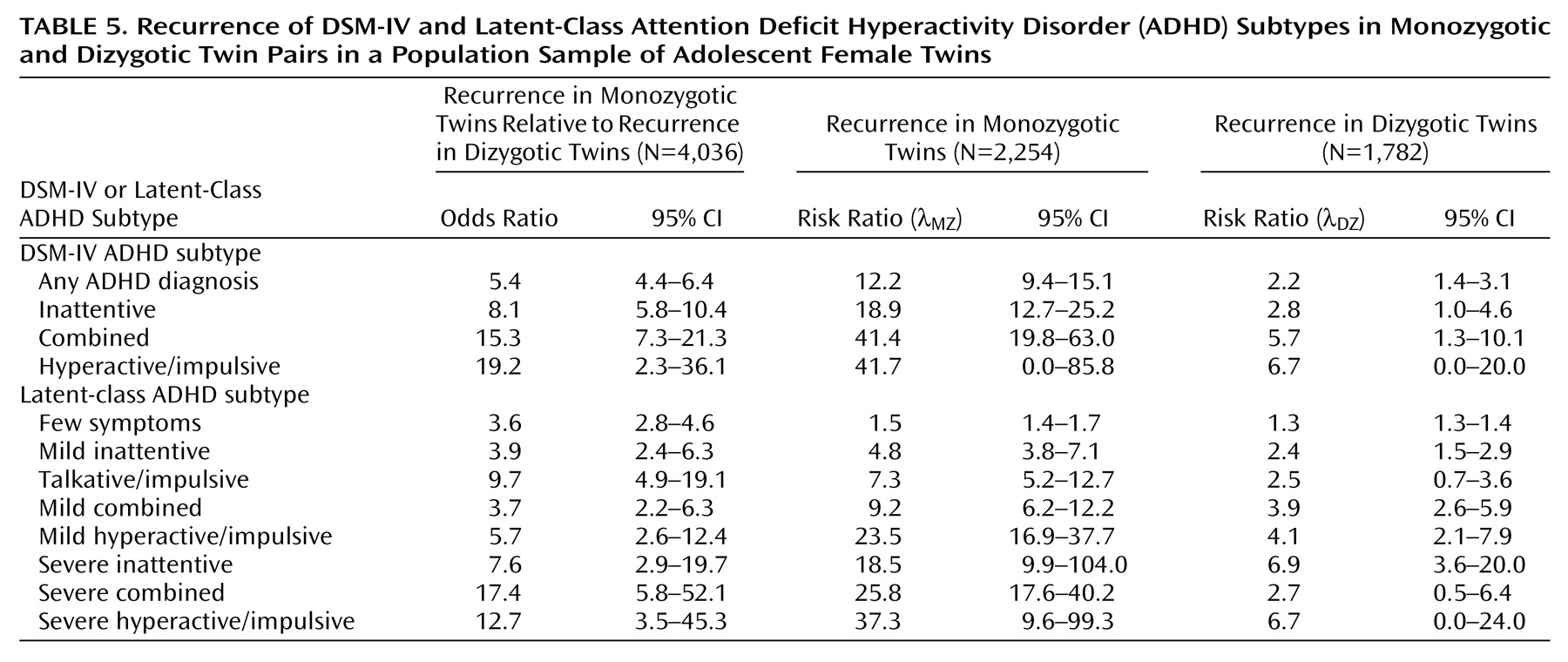
To test whether the phenotypically distinct DSM-IV and latent-class ADHD subtypes represent independent genetic forms of ADHD phenotypes, we compared the frequencies of the same subtype in monozygotic versus dizygotic twins (
Table 3,
Table 4, and
Table 5). For all eight latent classes and for the inattentive and combined DSM-IV ADHD subtypes there were significantly more monozygotic twins in the same class than dizygotic twins in the same class (
Table 3 and
Table 4). As shown in
Table 5, the odds ratios for monozygotic twins in the same class versus dizygotic twins in the same class ranged from 3.6 to 17.4. These results are consistent with a genetic basis for membership in both DSM-IV and latent-class ADHD subtypes. We similarly compared frequencies and odds ratios for monozygotic versus dizygotic twins for all six possible DSM-IV ADHD cross-subtype combinations and all 28 possible cross-subtype combinations of latent-class subtype. For DSM-IV subtypes, there was a significant cross-subtype odds ratio greater than 1 for the inattentive and combined subtypes (odds ratio=6.9, 95% CI=1.6–29.1). All other cross-subtype comparisons were nonsignificant or had odds ratios less than 1. Of the 28 possible latent-class combinations, only the combination of the mild inattentive subtype with the few symptoms subtype had an odds ratio above 1 (odds ratio=2.2, 95% CI=1.6–3.2). This later finding is of questionable significance owing to the number of comparisons across latent classes. These findings suggest that ADHD latent classes approximate pure genetic categories and that the inattentive and combined DSM-IV ADHD subtypes do not.
To allow comparison of our findings with those of other studies, we calculated the sibling recurrence risk ratio (λ
S)
(16) for the three DSM-IV ADHD subtypes and the eight latent-class subtypes (
Table 5). This ratio is an estimate of familiality adjusted for the population prevalence of a given disorder. For both DSM-IV and latent-class analysis approaches, the values of λ
S are greater for monozygotic than for dizygotic twins, consistent with a genetic contribution to liability. The magnitudes of the observed values for λ
DZ for the DSM-IV ADHD subtypes are similar to those reported for nontwin siblings
(18). It should be noted, however, that because of the low base rate of ADHD in girls, even in a population sample of this size, the 95% confidence intervals for several DSM-IV subtypes and latent classes in dizygotic twins are large and include 1.
Discussion
The current study of a large sample of female twins selected from birth records replicates and expands on our previous findings
(5,
10,
11). The inclusion of a larger sample allowed us to estimate the familiality and heritability of latent-class and DSM-IV ADHD subtype membership. In contrast to our previous findings
(5), the current data are most compatible with the presence of distinct and heritable ADHD phenotypes that differ in the relative contributions of individual inattentive and hyperactive/impulsive symptoms.
The analyses of DSM-IV ADHD subtypes in this population-based sample replicate the findings of the nonspecificity of DSM-IV subtypes in families from clinically referred or volunteer samples
(7–
9). In a study of families recruited through clinics, Faraone et al.
(7,
8) refuted the prediction of specificity of the DSM-IV inattentive and combined subtypes. In contrast, for the hyperactive/impulsive subtype of DSM-IV ADHD in boys they found almost complete exclusivity of hyperactive/impulsive subjects among relatives of hyperactive/impulsive probands
(8). Smalley et al.
(9) also found no specificity of the inattentive and combined subtypes but could not test for specificity of the hyperactive/impulsive subtype since they pooled together data from the families of probands with the combined and hyperactive/impulsive subtypes. In the current study we support the lack of family specificity of the DSM-IV inattentive and combined subtypes and also support the specificity of the DSM-IV hyperactive/impulsive subtype. When twin families were subtyped with latent-class criteria, however, the nonspecificity of the DSM-IV subtypes was resolved into specific familial conditions. These results are most compatible with the presence of independent, familial forms of ADHD that are approximated by latent-class analysis and are imperfectly operationalized by DSM-IV criteria.
A variety of previous studies have also attempted to define more heritable forms of ADHD by examining comorbid psychiatric disorders or other medical conditions (reviewed in references
2,
3,
6). In particular, Faraone et al.
(18) suggested that restriction of cases to persistent ADHD (the full diagnosis persists into young adulthood) or restricting cases to ADHD with comorbid conduct disorder or bipolar affective disorder leads to findings of a higher prevalence of recurrence of the illness among family members, relative to the general population. Although conduct disorder was rare and mania was not assessed in the current population sample of female twins, the majority of subjects with mood disorders and other disruptive behavior disorders that were comorbid with DSM-IV ADHD were included in the combined latent-class subtype
(11).
These results have implications for the design of molecular genetic studies to identify specific DNA sequences involved in the etiology of ADHD. Most ADHD candidate gene and genetic linkage studies use probands identified through clinical sampling or advertisement who meet DSM-IV criteria for ADHD. If the results of the current study are correct, then such recruitment strategies combine several genetically independent forms of ADHD while excluding many individuals with heritable ADHD subtypes who do not meet DSM-IV criteria. Such sampling strategies greatly reduce the power of both association and linkage studies to detect causative genes. Such mixing of heritable types of ADHD may explain the equivocal reports of the association of ADHD with candidate genes. It is interesting to note that two studies have reported that restricting findings to inattentive symptoms or subtypes increases the association of ADHD with polymorphisms of the DRD4 locus
(19,
20). Such family samples could be divided into more homogenous groups by application of the current types of analyses.
Although the ADHD classes described here have been demonstrated in both family
(10) and community twin samples
(5), the current study has several limitations, including the use of a twin sample, the restriction of data to parents’ reports about their children, and the restriction of the sample to adolescent females. The observed distribution of DSM-IV ADHD subtypes and the risk ratios for female dizygotic twins, as previously reported for male and female siblings in nontwin families
(7–
9,
18), suggests that any biases introduced by including only female twins are minor. In addition, the frequencies of dizygotic twins being in the same latent class are similar to those found for male and female nontwin siblings
(10). Most studies of the heritability of ADHD have used parents’ reports about male children. It is of obvious interest to expand the current findings by including twins’ self-reports and teachers’ reports. Critical tests of the familiality of these classes in male subjects, as well as the prevalence of individual classes in a nontwin community sample, await the application of these analytic approaches to other data sets.