Community surveys carried out over the past decade document that more than one-third of Americans use complementary and alternative medicinal treatments in a given year
(1–
4). There is reason to believe that the use of complementary and alternative therapies is more common among people with psychiatric problems than the rest of the population because fatigue, insomnia, chronic pain, anxiety, and depression are among the most commonly reported reasons for the use of complementary and alternative therapies in community surveys
(1,
4,
5). Results from the few previous studies of the use of complementary and alternative therapies among psychiatric outpatients reported in the literature are consistent with this speculation in showing high rates of complementary and alternative therapy use
(6–
8). Consistent with this evidence, a recent national survey of complementary and alternative therapies use
(4) reported that the use of such treatments is more common among people with self-defined anxiety and depression than among people with any other commonly occurring chronic condition other than back or neck problems. However, that report did not present data on the details of complementary and alternative therapies use among respondents with anxiety or depression, such as the types of users and the overlap of the use of complementary and alternative therapies with the use of conventional mental health services. This more detailed information is presented in the current report, which is based on the recent national survey.
Method
Sample
The survey was carried out between November 1997 and February 1998 among a sample of nationally representative telephone households by using random-digit dialing to select households and a random selection method to select one respondent age 18 or older for interview in each sample household. Verbal informed consent was obtained from all respondents before they began the interview. Eligibility was limited to English speakers without cognitive or physical impairments that prevented completion of an interview. The average administration time was 30 minutes. The Beth Israel Deaconess Committee on Clinical Investigations, Boston, Mass., approved the survey methods.
A total of 2,055 interviews were completed, representing a 60% weighted response rate. Weighting was used to adjust the data for geographic variation in cooperation (i.e., by region of country and urbanicity) and variation in probability of selection within each household. Another weighting adjusted for aggregate discrepancies between the sample distributions and Census population distributions on a variety of sociodemographic variables
(9,
10). More details on the sample design are presented elsewhere
(4). Owing to missing age data for six respondents, analyses are limited to the remaining 2,049 respondents.
Measures
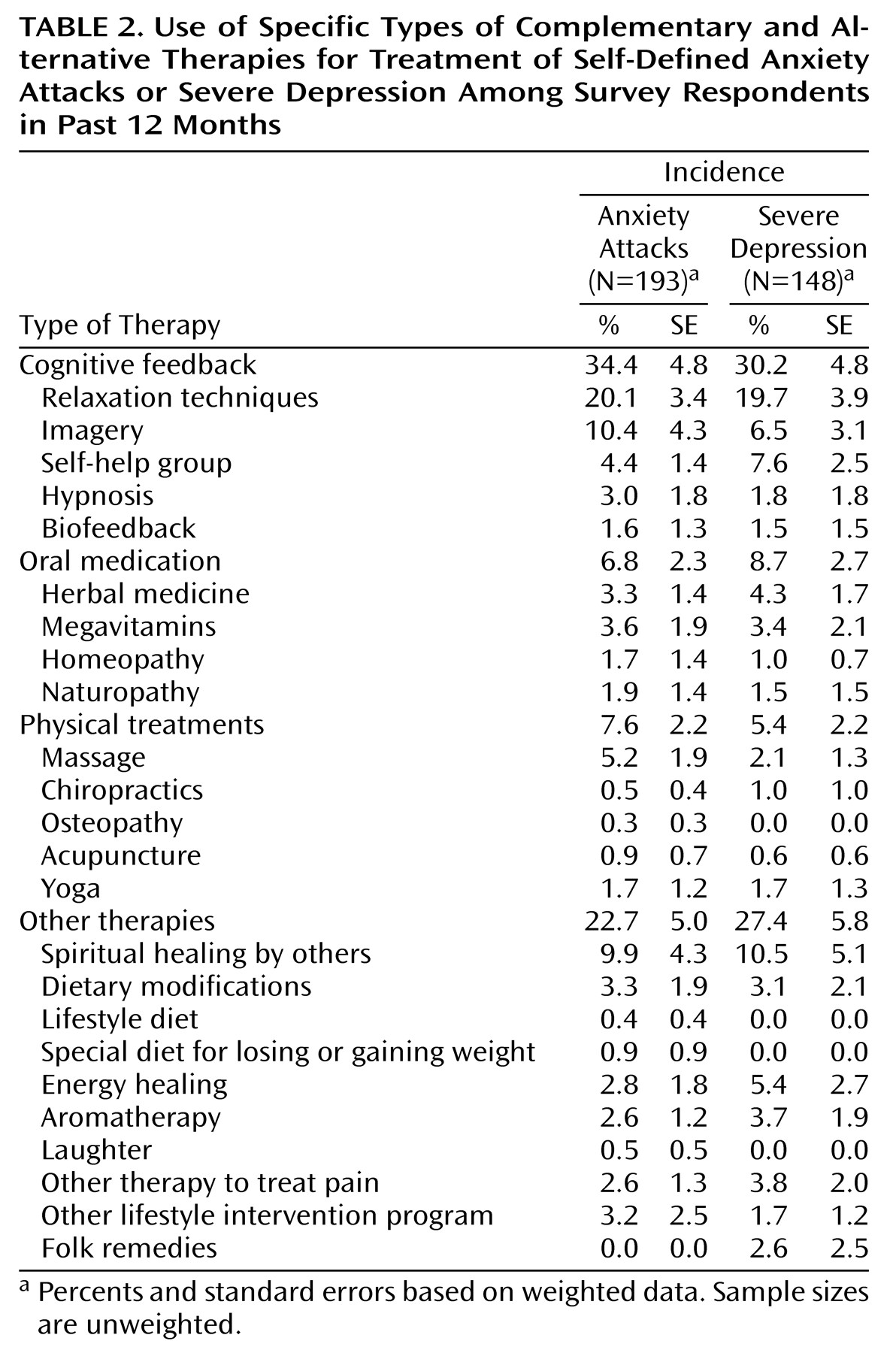
The interview was described to respondents as a survey about the health care practices of Americans carried out by investigators from Harvard Medical School. No mention was made of complementary and alternative therapies in characterizing the study. The first substantive questions concerned perceived health, functional impairment due to health problems, and interactions with medical doctors. The next questions asked about approximately two dozen chronic conditions on the basis of a checklist. The categories “anxiety attacks” and “severe depression” were included in this checklist. Interviewers then queried respondents about their lifetime and 12-month use of 24 complementary and alternative therapies that we subsequently divided into four larger subcategories for purposes of analysis: cognitive feedback (relaxation techniques, imagery, self-help groups, hypnosis, and biofeedback), oral medication (herbal medicine, megavitamins, homeopathy, and naturopathy), physical treatments (massage, chiropractics, osteopathy, yoga, and acupuncture), and other therapies (spiritual healing by others, dietary modifications, lifestyle diet, special diet for losing or gaining weight, energy healing, aromatherapy, folk remedies, laughter, other therapy to treat pain, and other lifestyle intervention programs).
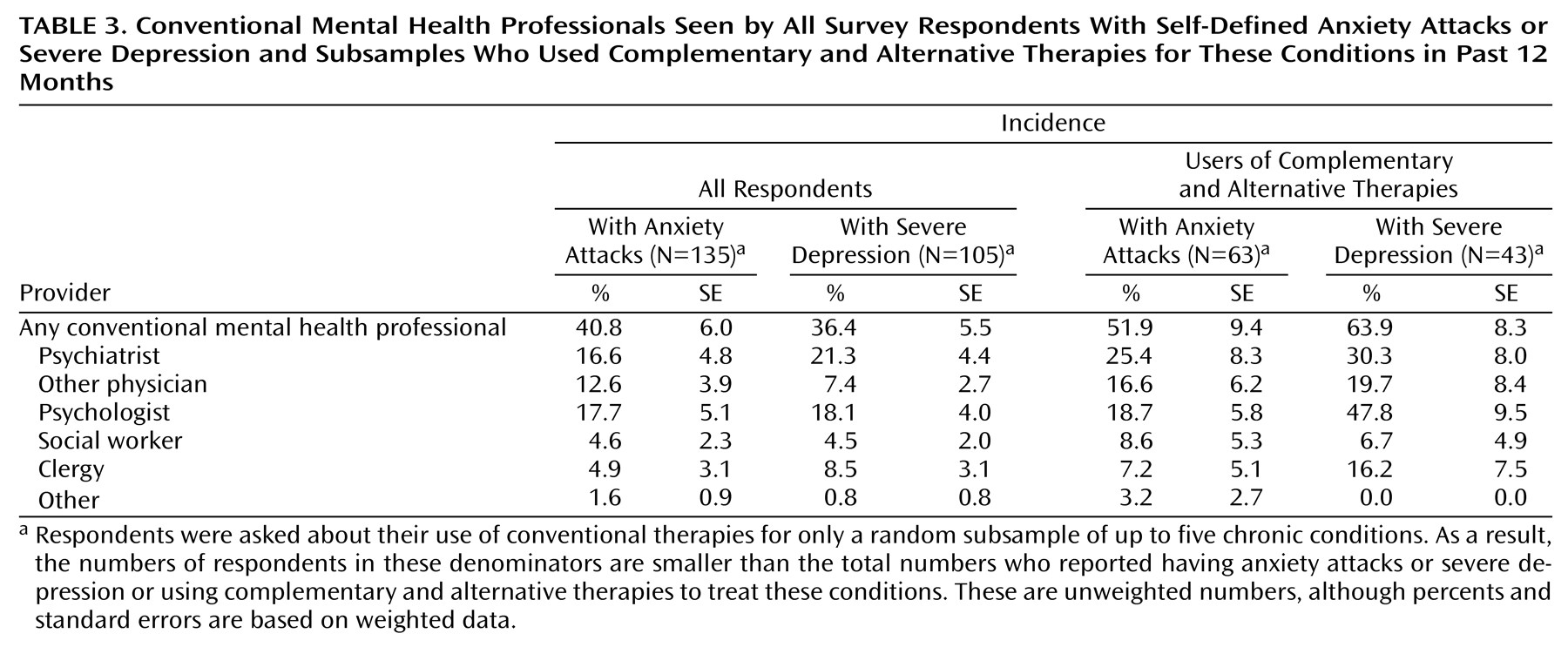
Lifetime users of each complementary and alternative therapy were then asked their age at first use, their time of use, whether their complementary and alternative treatment was supervised by a professional trained in their use, and their reasons for recent use. Respondents who reported chronic conditions were asked about their use of complementary and alternative therapies in the past 12 months for each of these conditions. Use of conventional therapies for chronic conditions in the past 12 months was assessed for up to five chronic conditions for each respondent. When an individual respondent reported having more than five conditions, a random five were selected for questioning, and condition-specific data were weighted to adjust for differential probabilities of selection. Respondents with chronic conditions were asked to rate the perceived helpfulness of complementary and alternative therapies and conventional therapies. The final questions dealt with sociodemographics.
Statistical Analysis
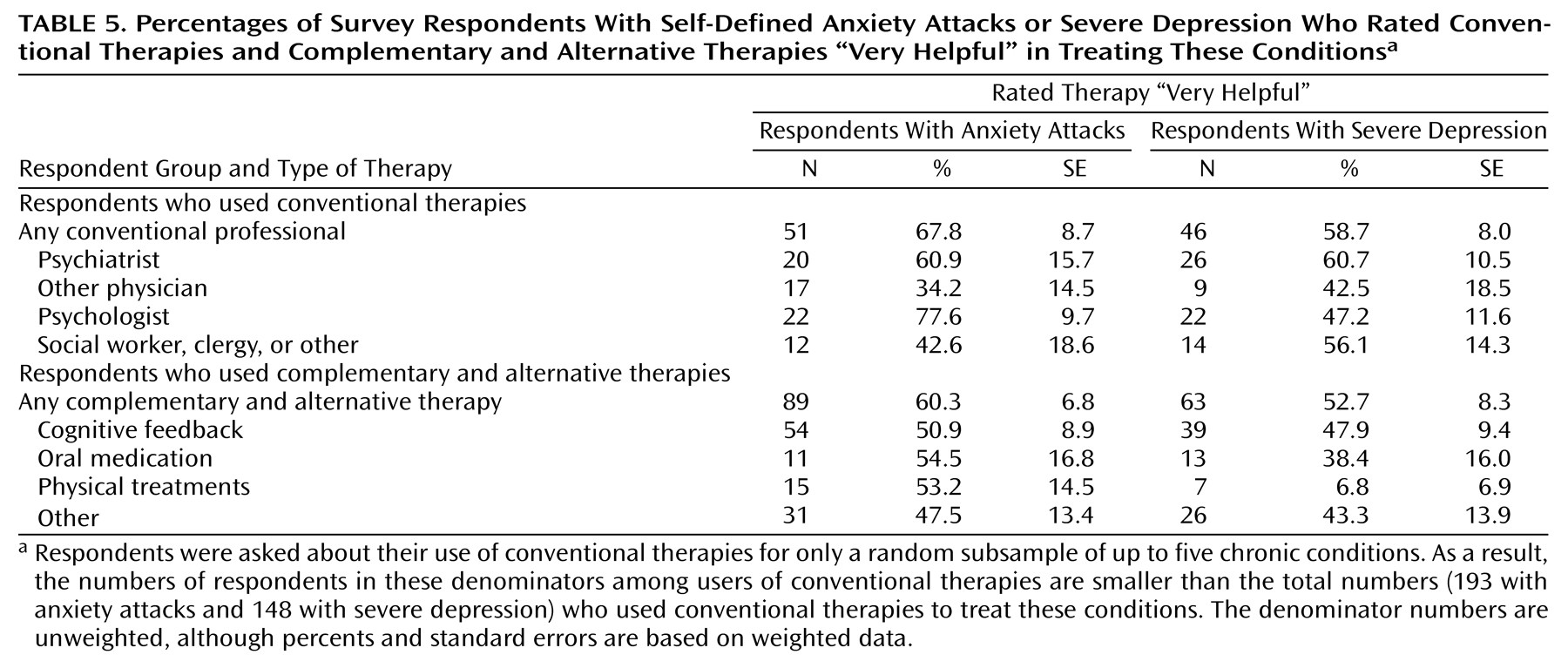
Cross-tabulations were used to estimate the proportions of respondents who had, in the 12 months before the interview, used conventional and complementary therapies and alternative therapies for self-defined “anxiety attacks” and “severe depression.” Cross-tabulations were also used to estimate the proportions of respondents who perceived these therapies to be helpful. Finally, logistic regression analysis was used to study the sociodemographic predictors of 12-month complementary and alternative therapies use among respondents with anxiety attacks and severe depression.
All results are based on analyses using weighted data. To adjust for the design effects introduced by this weighting, jackknife repeated replications simulations
(11) were used to estimate standard errors. Jackknife repeated-replications simulations are one of several methods that use simulations of coefficient distributions in subsamples to generate empirical estimates of standard errors and significance tests. The ratios of the coefficients to these adjusted standard errors were used to compute the 95% confidence intervals of estimates. Tests for the significance of sets of predictors taken together were computed by using Wald chi-square tests from coefficient variance or covariance matrices on the basis of jackknife repeated-replications simulations.
Discussion
The results reported here are limited by the restriction of the sampling frame to people who spoke English and lived in households with telephones, as well as by the relatively low response rate (60%)
(1). An additional limitation is that we have no independent confirmations of respondent characterizations of themselves as having “anxiety attacks” or “severe depression.” Finally, the omnibus nature of the survey made it impossible to probe a variety of issues regarding complementary and alternative therapies use for anxiety and depression as deeply as would have been done in a survey that focused exclusively on mental disorders. For example, no information was obtained on the types of herbal therapies used to treat these conditions or the extent to which conventional providers either recommended or provided complementary and alternative therapies.
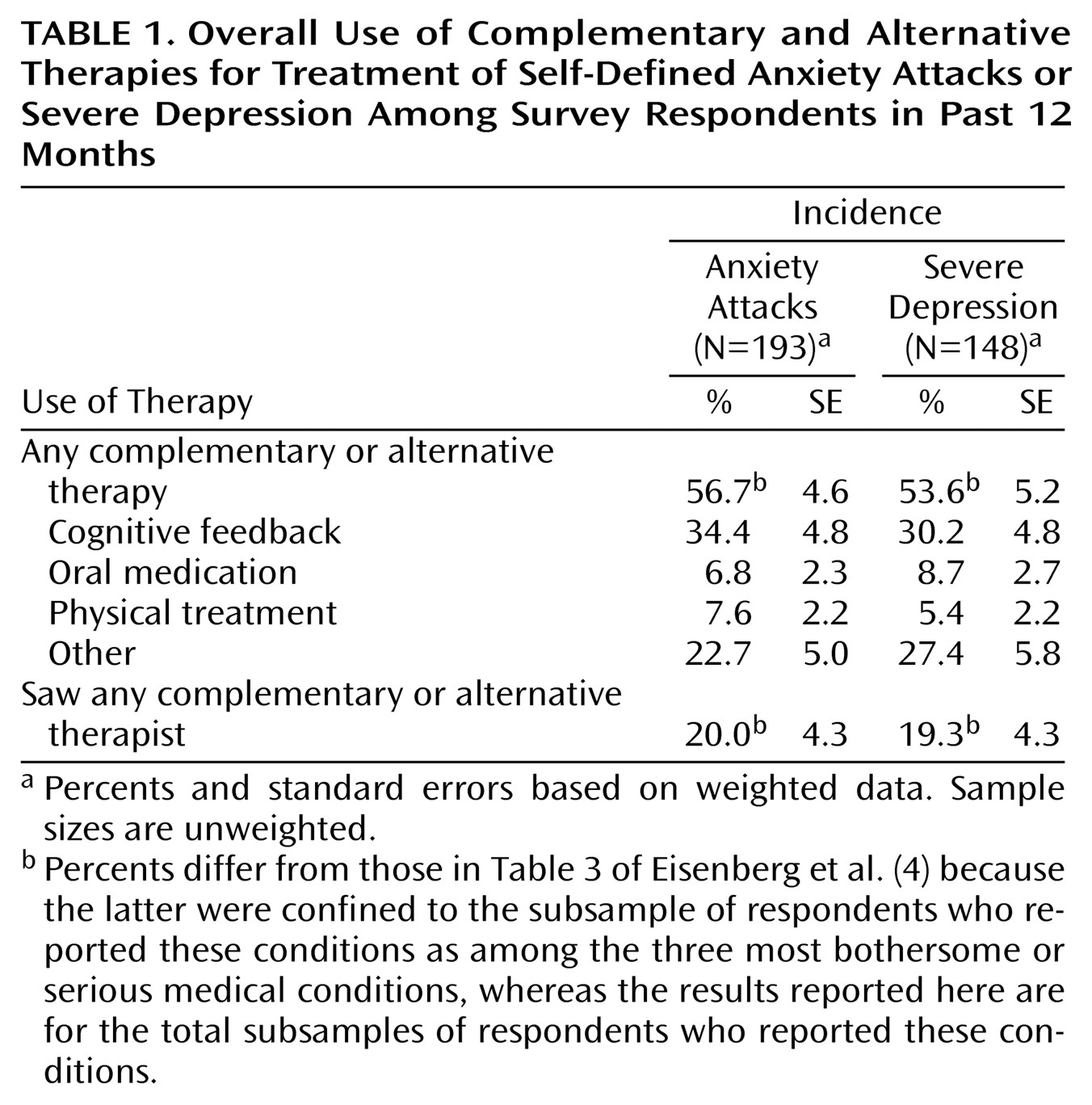
Within the context of these limitations, the results suggest that the majority of people in the United States with self-defined anxiety attacks or severe depression use some form of complementary and alternative therapy to treat these conditions. This means that people with these conditions are considerably more likely to use complementary and alternative therapies than conventional medical or mental health treatments.
Some evidence exists regarding the efficacy of certain complementary and alternative therapies in treating depression and, to a lesser extent, anxiety. The most extensive evidence comes from nearly 30 controlled trials that have evaluated St. John’s wort (
Hypericum perforatum) in the treatment of depression. Two separate meta-analyses of these studies
(13,
14) concluded that St. John’s wort is superior to placebo and comparable to conventional pharmacotherapy in the treatment of various severities of depression. The first U.S., large-scale, controlled clinical trial to study the effect of St. John’s wort on major depression is currently underway with funding from the National Institutes of Health’s National Center for Complementary and Alternative Medicine
(15). Another fairly extensive series of studies has evaluated the effects of various types of exercise in treating depression. Two meta-analyses of these studies
(16,
17) concluded that both aerobic and nonaerobic exercise are superior to results obtained from control groups on waiting lists in treating mild to moderate depression. Less extensive evidence exists from two controlled trials
(18,
19) showing positive effects of relaxation (the complementary and alternative therapy most commonly used to treat anxiety and depression) and meditation on the reduction of depression and from one controlled trial
(20) showing positive effects of relaxation on the reduction of anxiety. At least seven randomized controlled trials have evaluated the effects of the herb kava (
Piper methysticum) for the symptomatic treatment of mild anxiety
(21–
27). The results have been positive but have been criticized because of methodological flaws. Finally, two trials have evaluated the effects of acupuncture in treating depression by using sham or nonspecific acupuncture as a control. One of these
(28) found positive effects, and the other
(29) did not.
Contrary to the results of Knaudt et al.
(6) in a survey of psychiatric outpatients in North Carolina, who found that herbal therapies made up a substantial proportion of total complementary and alternative therapies use, our national data found that herbal therapies made up only a small proportion of all complementary and alternative therapies use for self-defined anxiety attacks and severe depression. However, this is such a rapidly changing area of treatment, due in large part to substantial increases in direct-to-consumer advertising of herbal therapies and expansion of sales into grocery stores and pharmacies in recent years, that the situation might well be different at present. No information was collected on the types of herbal therapies used to treat anxiety or depression, making it impossible for us either to confirm or refute data from less representative studies on the types of herbal therapies most often used to treat these conditions.
The high proportions of self-defined anxious and depressed patients who use complementary and alternative therapies are especially striking because insurance coverage for these therapies has only recently begun
(30). On the basis of the plausible assumption that demand for complementary and alternative treatments is similar to demand for conventional health care in sensitivity to how much patients are willing to pay out of pocket
(31), it seems likely that the proportion of people using complementary and alternative therapies will increase as insurance coverage for these treatments expands in the future.
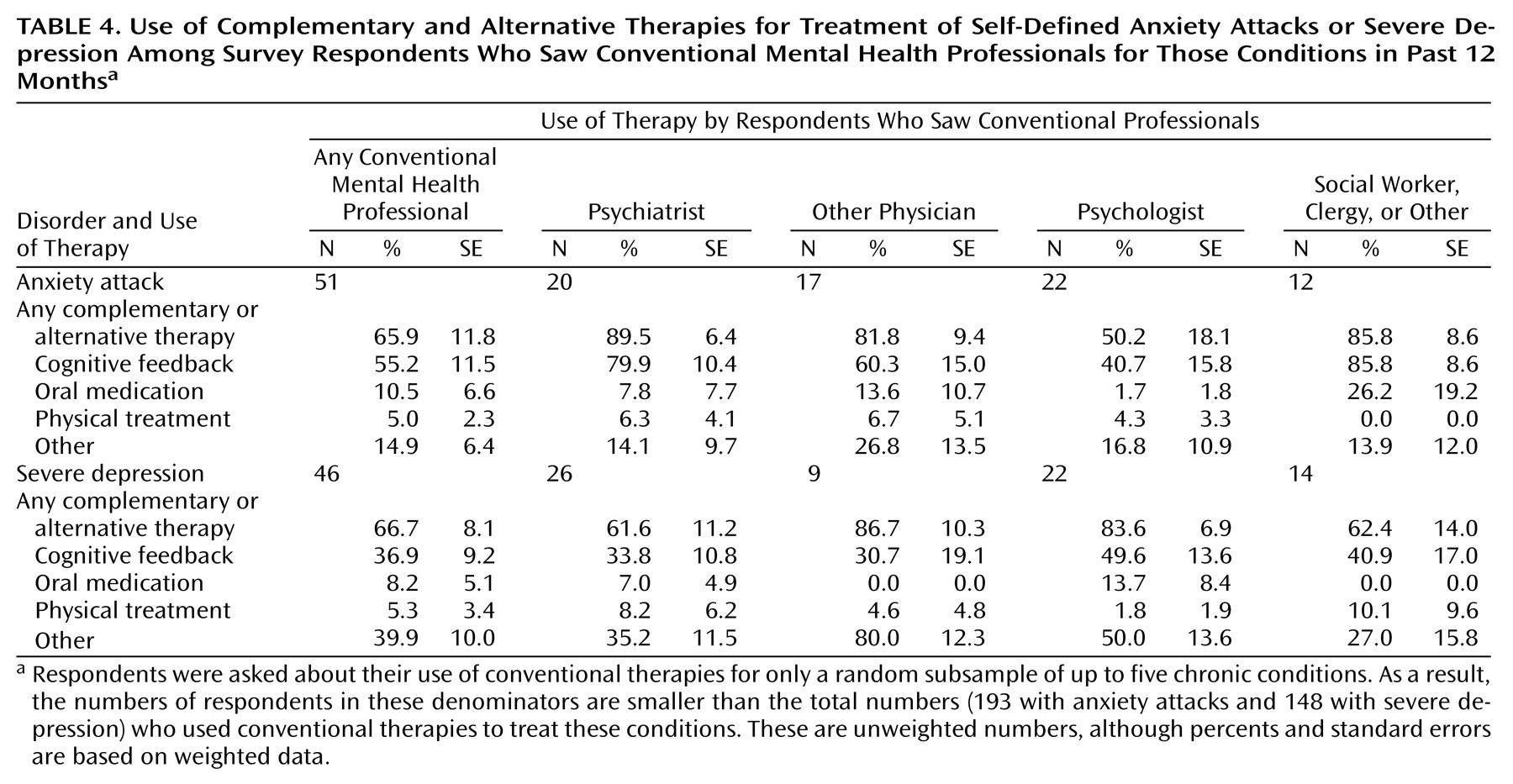
We found that there is a positive association between complementary and alternative therapies use and use of conventional therapy. Close to nine out of every 10 patients with self-defined anxiety attacks who are seen by a psychiatrist also use some type of complementary and alternative therapy to treat anxiety, while more than six out of every 10 patients with self-defined severe depression who are seen by a psychiatrist also use some type of complementary and alternative therapy to treat depression. These rates hold regardless of the wide range of sociodemographic characteristics of patients.
It is important to recognize that this combined use of complementary and alternative therapies and conventional therapy can be dangerous, because case studies show that some types of complementary and alternative therapies can create potentially dangerous interactions with pharmacotherapies
(32,
33). For example, recent case reports suggest that mixing St. John’s wort with selective serotonin reuptake inhibitors can induce a mild serotonin syndrome
(34). In vitro studies also suggest that hypericum extracts are potent inducers of hepatic enzymes and are therefore capable of reducing the plasma concentrations of a variety of concomitant prescription medications, such as indinavir for patients with HIV
(35,
36).
We know from our previous analyses of other parts of the survey reported here that only a minority of patients who use complementary and alternative treatments inform their doctors
(3,
4). As this is the case, and in light of the potential risks of some complementary and alternative therapies, mental health professionals need to adopt a more proactive posture than they have up until now to discuss complementary and alternative therapies use with their patients. Opening up lines of communication could help prevent adverse clinical effects, as well as maximize the usefulness of any complementary and alternative therapies subsequently proven to be effective
(32).