Although it is commonly accepted that individuals with alcohol dependence sleep poorly
(1–
3), few studies have investigated the rate of insomnia in alcoholic patients. Baekeland et al.
(4) reported that 36% of 294 alcoholic outpatients had high scores for sleep disturbance as measured by a clinic physician. Similarly, Feuerlein
(5) reported that 37% of 184 inpatients and outpatients with alcoholism had “sleep disturbance” as determined by a semistandardized interview. Caetano et al.
(6) investigated insomnia as a withdrawal symptom and found a 42% rate among 445 people referred to educational programs for driving under the influence of alcohol and a 67% rate among 748 men admitted to detoxification and residential treatment centers. These insomnia rates (36% to 67%) are higher than those found in the general population (17% to 30%)
(7). Nevertheless, comparisons of these studies are difficult, because different insomnia measures and time frames were used and because the study groups may have differed in demographic characteristics, drinking severity, presence of alcohol withdrawal, and diagnostic comorbidity.
To our knowledge, the occurrence of insomnia and its self-medication with alcohol has not been investigated simultaneously in alcoholic groups
(4–
6). Nevertheless, other studies provide useful frequency estimates of self-medication. Skoloda et al.
(8) reported that 62% of treated alcoholics believed that alcohol helped them sleep. Likewise, Mamdani et al.
(9) found that 60% of 92 male inpatients with alcoholism reported hypnotic use of alcohol. These self-medication rates are greater than rates reported for the general population (6% to 13%) and for people with initial insomnia (15% to 28%)
(10–
12). Perhaps the highest rate of self-medication was reported for a group of 155 older women (85 or more years old) with symptomatic insomnia, of whom 70% used alcohol for sleep
(13).
Given that insomnia during early recovery has been linked to relapse
(8,
14–
16), the frequency and correlates of insomnia in alcoholics are important areas of investigation. In the present study of patients with alcoholism, we investigated 1) the frequency and clinical correlates of insomnia, 2) the frequency of drinking to self-medicate insomnia, and 3) the relationships of insomnia and self-medication to subsequent relapse. We reasoned that patients with alcoholism who reported insomnia would be more likely to self-medicate insomnia with alcohol and, therefore, more likely to relapse than patients without insomnia. We also hypothesized that self-reported insomnia would be associated with female gender, older age, more severe alcohol dependence, more severe depression, and worse sleep continuity as measured by polysomnography.
Results
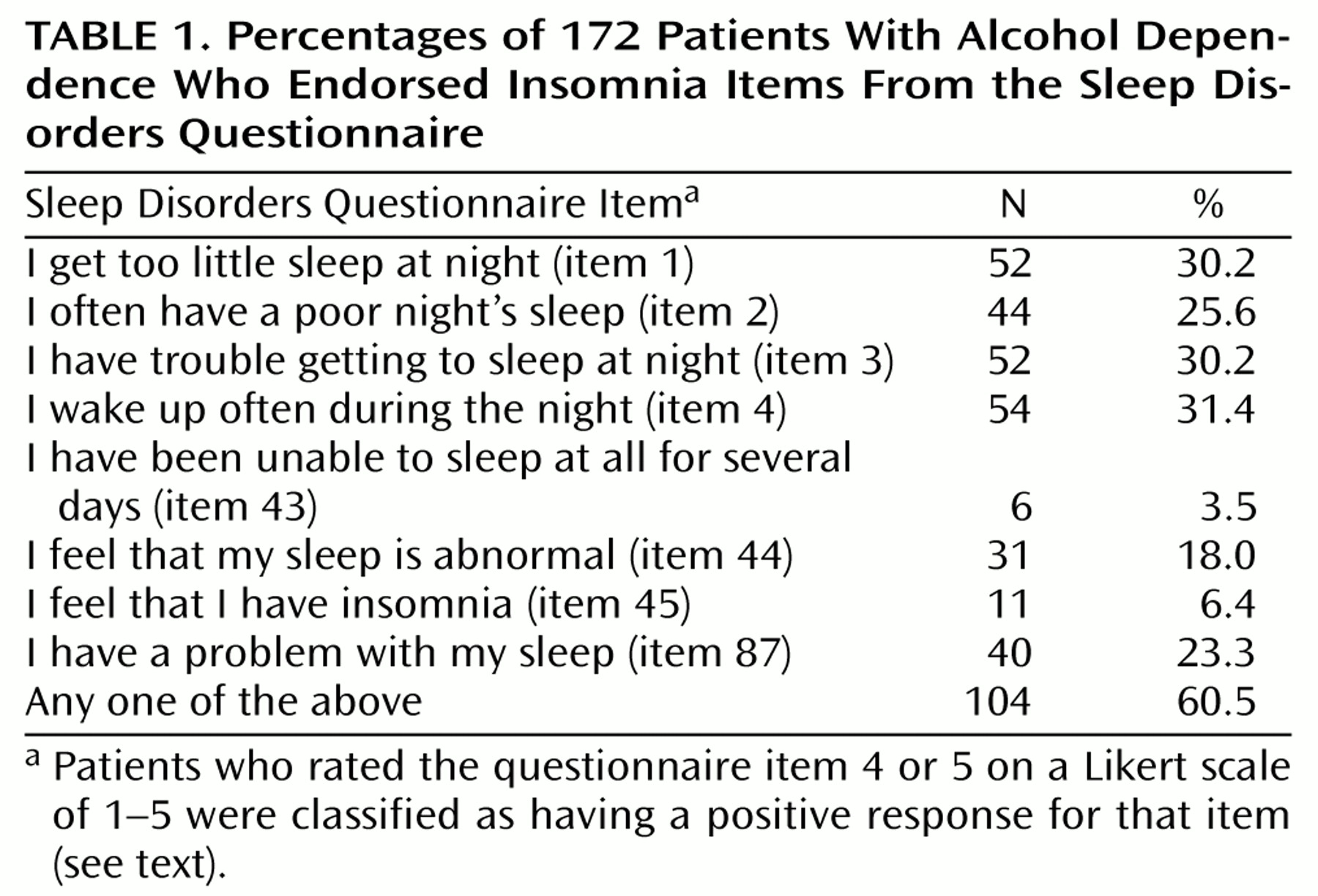
The percentage of subjects with a positive response to each of the eight insomnia-related Sleep Disorders Questionnaire items appears in
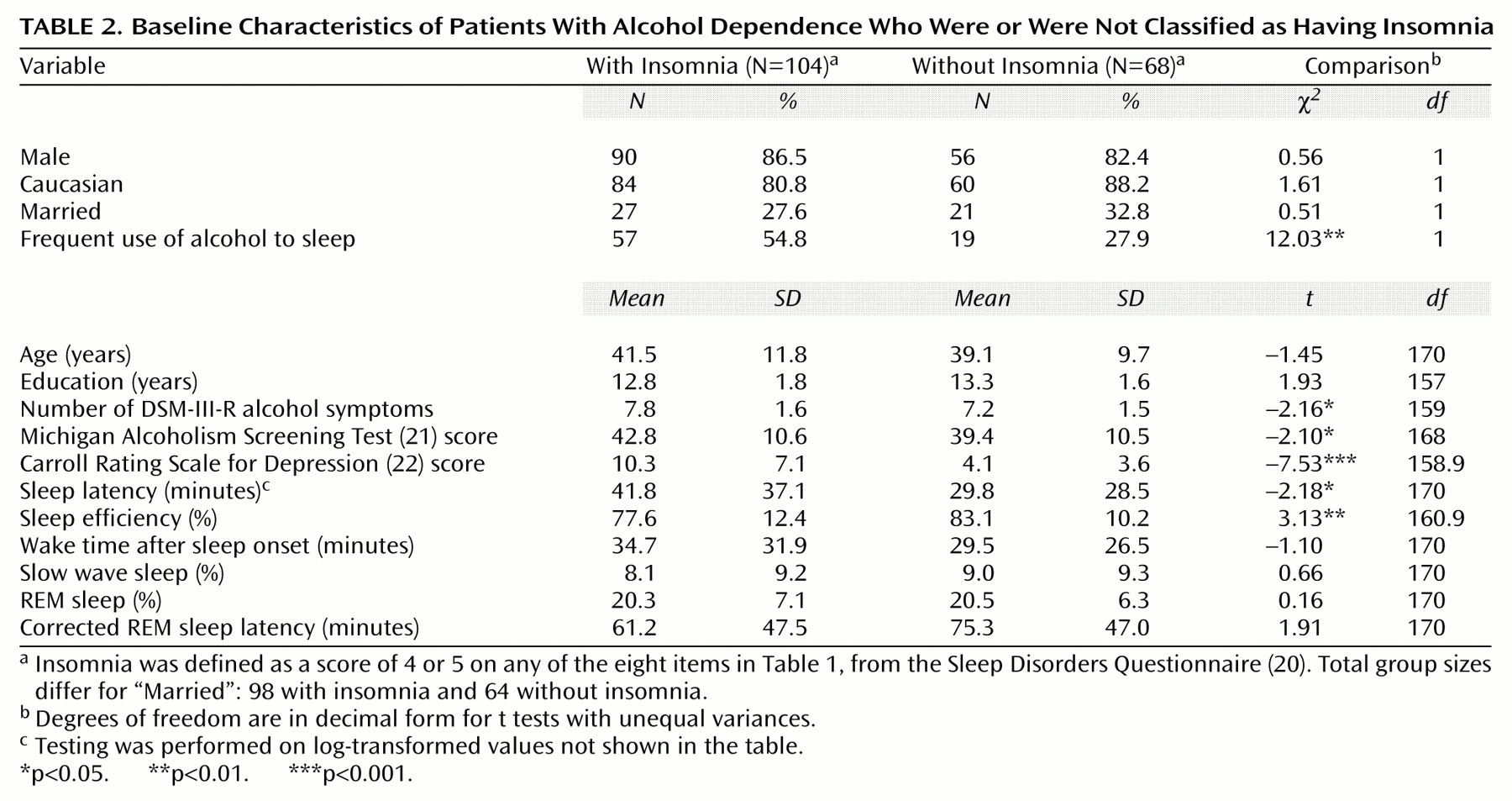
Table 1. Of the 172 alcoholic patients, 60.5% had a positive response on at least one of the eight items and were therefore classified as having insomnia. The patients classified as having insomnia had significantly longer sleep latency times and lower sleep efficiency values on polysomnography than patients without insomnia (
Table 2). The insomnia group had higher values for wake time after sleep onset than the group without insomnia, although the difference was not significant.
The patients with insomnia scored significantly higher on both measures of alcohol severity—DSM-III-R symptom count and MAST score—and on the Carroll Rating Scale for Depression than did the patients without insomnia (
Table 2). No significant differences were found for demographic variables. The patients with insomnia were more likely to report using alcohol often for sleep than were the patients without insomnia (
Table 2). Altogether, 76 (44.2%) of the 172 patients responded that they often used alcohol to get to sleep. We found no significant differences between groups in percentage of REM sleep, percentage of slow wave sleep, or corrected REM sleep latencies, although the patients with insomnia tended to have shorter corrected REM sleep latency than the patients without insomnia (
Table 2).
Of the 74 patients who were followed after treatment, 36 (48.6%) relapsed. Because the follow-up rate was only 43.0%, we compared the followed (N=74) and nonfollowed (N=98) patients on baseline characteristics. We found no significant differences between these two groups in terms of insomnia rate, age, gender, race, marital status, education, number of DSM-III-R alcohol dependence symptoms, MAST score, sleep efficiency, sleep latency, percentage of slow wave sleep, percentage of REM sleep, corrected REM sleep latency, or recruitment site. The followed patients had longer wake times after sleep onset than the nonfollowed patients (mean=38.1 minutes, SD=34.7, versus mean=28.5 minutes, SD=25.0) (t=–2.01, df=126.7, p=0.05) and also had higher depression scores (mean=9.0, SD=7.8, versus mean=6.9, SD=5.5) (t=–1.96, df=125.8, p=0.052). Therefore, these two variables were included in the regression analyses (to be described).
Within the subjects who were followed up, the patients with baseline insomnia were more likely to relapse (59.6%, 28 of 47) than those without baseline insomnia (29.6%, eight of 27) (χ2=6.16, df=1, p=0.02). The patients with and without insomnia had nearly identical follow-up durations (mean=142.9 days, SD=54.6, versus mean=142.4 days, SD=57.1) (t=–0.04, df=72, p=0.97), so they had similar risk periods for relapse. To determine the effect of insomnia on relapse after controlling for severity of alcohol dependence (MAST score and DSM-III-R alcohol dependence symptom count), depression severity (Carroll scale score), and wake time after sleep onset, we used a logistic regression analysis in which all variables were forced to stay in the model. This analysis included 70 subjects because data on some variables were missing for four patients. We found that baseline insomnia was the only significant predictor of relapse (Wald χ2=4.90, df=1, p=0.03). The collinearity was acceptable, with tolerance values ranging from 0.64 to 0.92.
The followed patients who used alcohol to self-medicate insomnia had a higher relapse rate (59.5%, 22 of 37) than the patients who did not self-medicate (37.8%, 14 of 37), a difference that approached significance (χ2=3.46, df=1, p=0.07). After we controlled for drinking severity, depression severity, and wake time after sleep onset using another forced-entry logistic regression analysis, the self-medication variable remained nonsignificant (Wald χ2=2.70, df=1, p=0.10). Again, the collinearity statistics were acceptable, with tolerance values ranging from 0.74 to 0.94.
Discussion
To our knowledge, the occurrence of symptomatic insomnia and drinking to self-medicate insomnia have not been simultaneously studied in alcoholic patients. According to a measure derived from the Sleep Disorders Questionnaire, over 60% of our study group reported high levels of insomnia symptoms during the 6 months before treatment. Also, nearly 45% of the alcoholic patients reported using alcohol often in order to get to sleep during the 6 months before treatment. The patients with insomnia were about twice as likely to report using alcohol to sleep as patients without insomnia were (55% versus 28%). Similar rates of insomnia
(4–
6) and its self-medication with alcohol
(8,
9) have been found in other studies of alcoholic patients in treatment, even though the frequency rates across studies vary according to subject characteristics, time frame, and measures of insomnia. A similar rate of self-medicating insomnia with alcohol among patients with schizophrenia (56%)
(28) suggests that some of our findings may generalize to other patient populations as well.
That alcohol-dependent patients use alcohol to self-medicate insomnia is both understandable and maladaptive. On the one hand, if insomnia is a withdrawal symptom, either acute or protracted
(6,
29), then relief drinking is a likely strategy, especially given that alcohol has a reinforcing effect in individuals with insomnia
(30). On the other hand, there is general scientific consensus that both acute and chronic alcohol use disrupt sleep patterns
(1–
3,
31,
32). Therefore, self-medication of insomnia with alcohol, even if reinforcing, may paradoxically worsen insomnia. Consequently, a vicious circle may develop in which alcohol initially makes it easier to fall asleep, but as tolerance to this sedative effect develops, the sleep-disruptive effects of alcohol become more apparent if not more severe
(31). Some patients may persist with self-medication despite worsening insomnia, because their drinking behavior is ingrained and reinforcing, and they feel desperate for sleep.
The levels of severity of both alcohol dependence and depression were significantly associated with insomnia. Because we excluded patients with current major depression, depressive symptoms in this study were most likely related to alcohol, dysthymia, or social stressors. We did not find higher rates of insomnia in women than in men or as a function of increasing age, a result contrary to findings in some studies of the general population
(33,
34) and primary care practices
(35). Age and gender differences for insomnia may disappear among patients seeking treatment for alcohol dependence. Although alcoholism severity and depression severity were significantly associated with insomnia, we did not measure anxiety symptoms despite evidence from recent studies
(36,
37) that supports a significant relationship between anxiety and sleep disturbance in alcoholic patients. Therefore, further studies are needed before we can make more than tentative conclusions about the correlates of insomnia among alcoholic patients.
As in other studies
(8,
14–
16), baseline insomnia predicted relapse to alcoholism. Baseline insomnia remained a predictor of relapse even after we controlled for severity of alcohol dependence and depressive symptoms. Contrary to our hypothesis, patients with a history of self-medicating insomnia with alcohol were not significantly more likely to relapse than nonmedicating patients.
Of the eight insomnia items, “I feel that I have insomnia” and “I have been unable to sleep at all for several days” were least sensitive, with only 6% and 4% of the subjects endorsing these respective items (
Table 1). Other insomnia items were endorsed by 18% to 32% of the subjects. This finding suggests that patients who report symptoms of insomnia do not necessarily think of themselves as having insomnia. Asking patients if they have insomnia may be analogous to asking them if they are alcoholic; patients may avoid these labels because of denial, stigma, definitions of these terms that exclude themselves, and/or fear of treatment implications. Not being able to sleep at all for several days is uncharacteristic of alcohol dependence except for extreme cases of alcohol withdrawal, such as those involving delirium tremens, which occurs in only about 5% of alcohol-dependent patients
(38). This may explain the insensitivity of that question. Future studies should address the optimal screening questions for insomnia among alcoholic patients.
Several methodological issues may limit the interpretation of results. First, we studied alcoholic patients who underwent polysomnography for research purposes. It is possible that alcoholics in treatment who have sleep complaints are likely to volunteer for sleep studies, thus skewing our frequency rates for insomnia and its self-medication with alcohol. However, our rate of insomnia was comparable to the rates in other studies
(4–
6) and provides further evidence of the frequency of these phenomena. Nevertheless, many patients may have entered the study because of their sleep problems, which could limit the generalizability of these results.
Second, our eight-item measure of insomnia was derived from a standardized and validated sleep questionnaire
(20), but full psychometric testing of the abbreviated questionnaire was beyond the scope of this study. For example, we did not calculate the sensitivity and specificity of the eight-item insomnia measure, because we did not conduct standardized clinical interviews for insomnia, and polysomnography by itself is not a gold standard for the evaluation of insomnia
(39,
40). Nevertheless, in addition to face validity, the insomnia measure was associated with drinking and depression severity, with polysomnographic measures of sleep fragmentation, and with relapse, providing evidence of concurrent, external, and predictive validity, respectively.
Third, only 43% of the patients were followed over time. The low follow-up rate reflects the fact that longitudinal outcomes were added as a secondary area of interest after the beginning of our primary investigations on the effects of alcoholism and aging on sleep abnormalities
(17). It is true that the followed and not-followed patients did not differ on any baseline variables except depression and wake time after sleep onset, and when these two variables were entered into the logistic regression analysis, insomnia remained a robust predictor of relapse. Nevertheless, the low follow-up rate remains a limitation, because patients lost to follow-up have potentially higher relapse rates than followed patients. Fourth, sleep measures were recorded on only one night, which did not allow subjects to adjust to the “first night effect” of sleeping under novel conditions. Fifth, relapse status was determined solely by self-report without biochemical or other corroboration, such as by a friend or family member. Still, whatever self-report bias occurred was expected to be similar across comparison groups.
In summary, symptoms of chronic insomnia and the use of alcohol to aid sleep were prevalent in alcoholic patients. Insomnia was significantly associated with severity of alcohol dependence, depressive symptoms, and polysomnographic measures of poor sleep continuity, and it was predictive of drinking during the follow-up period. These results suggest that alcoholic patients at risk for relapse are easily identifiable by routine questions about sleep. The potential for improving drinking outcomes by treating insomnia in alcoholic patients is now being investigated
(41–
43).