Systematic knowledge regarding the “state of mind” of those who attempt suicide remains elusive. Ratings of thoughts and attitudes around the time of a suicidal act have some power to predict future suicidal behavior
(1–
3), but little is known about the most basic aspects of cognitive processing in suicidal individuals, even though impaired cognitive functioning is common in psychiatric disorders for which suicide risk is elevated
(4,
5).
Suicide attempters have been characterized as “cognitively rigid” on the basis of self-ratings and performance on mental flexibility tasks
(6–
13). From case studies
(14), Rourke et al.
(15) suggested that a specific nonverbal learning disability may predispose individuals to suicidal behavior. Bartfai et al.
(16), using standard neuropsychological measures, found poorer performance on measures of fluency (verbal as well as nonverbal) and reasoning in a small sample of recent suicide attempters compared to chronic pain patients and nonpatients. Ellis et al.
(17), on the other hand, found no neuropsychological differences between diagnostically heterogenous groups of suicidal and nonsuicidal patients.
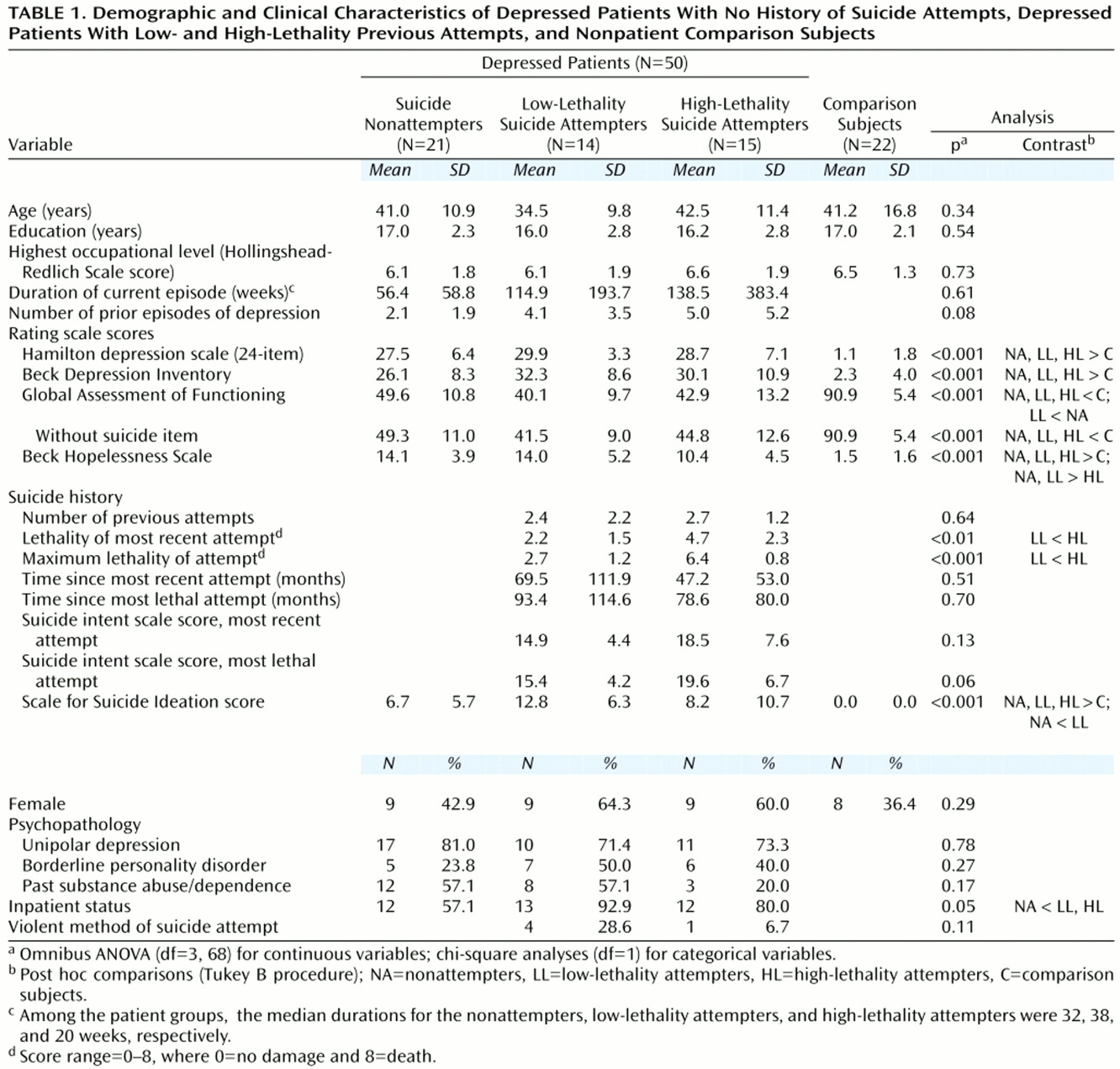
In this study, neuropsychological performance was assessed in a group of well-characterized, unmedicated subjects who met DSM-III-R criteria for a major depressive episode with or without a history of suicidal behavior. Past attempters were divided into two groups on the basis of the severity of their attempts. Prior research has suggested that those making more severe attempts are a distinct subgroup
(18–
20) who are demographically and biologically more similar to suicide completers
(21–
24). The depressed patient groups were also compared to a nonpatient group.
On the basis of prior studies of neuropsychological functioning in patients with depression
(25–
27), all depressed subjects were expected to perform poorly, relative to nonpatients, on measures of general intellectual functioning (because of deficits on performance IQ-type tasks), motor functioning, attention, and memory. On the basis of these studies and on potential links between suicidal behavior and prefrontal cortical dysfunction
(28,
29), past suicide attempters were expected to perform relatively more poorly on executive functioning measures.
Discussion
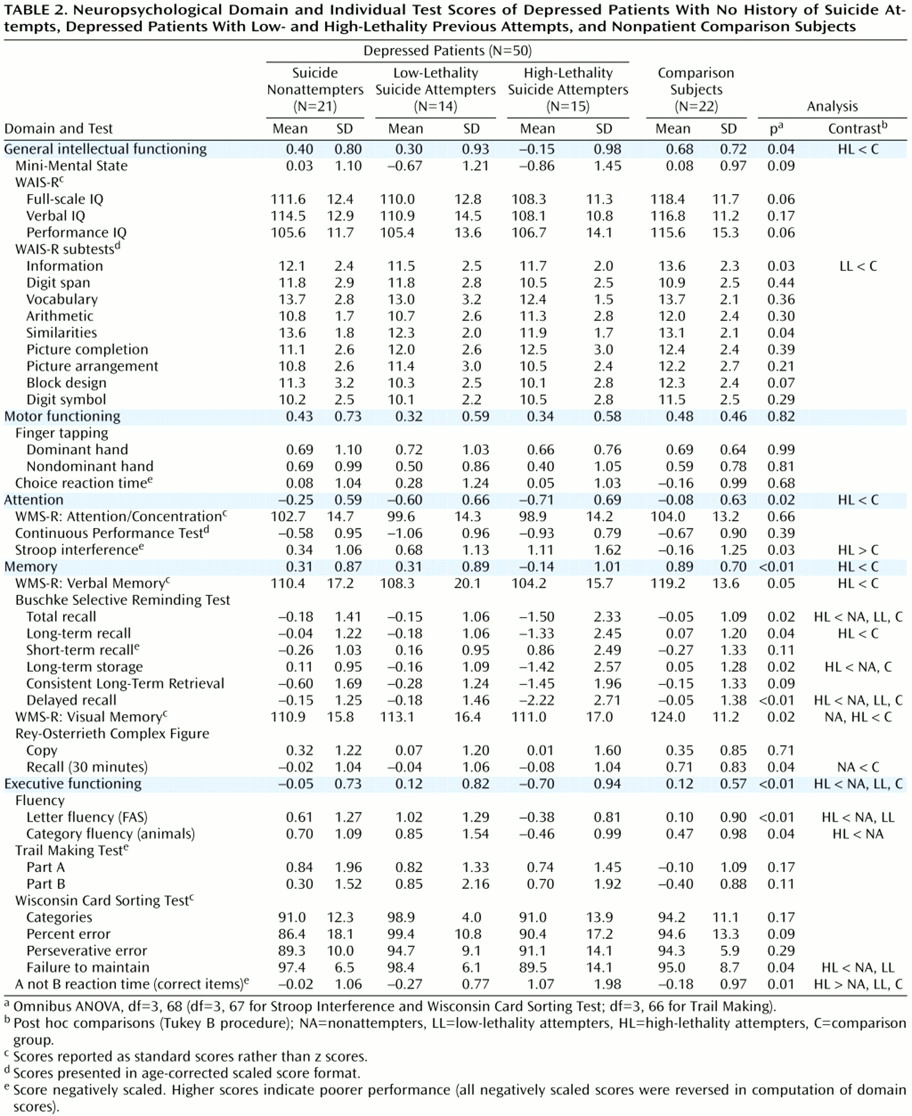
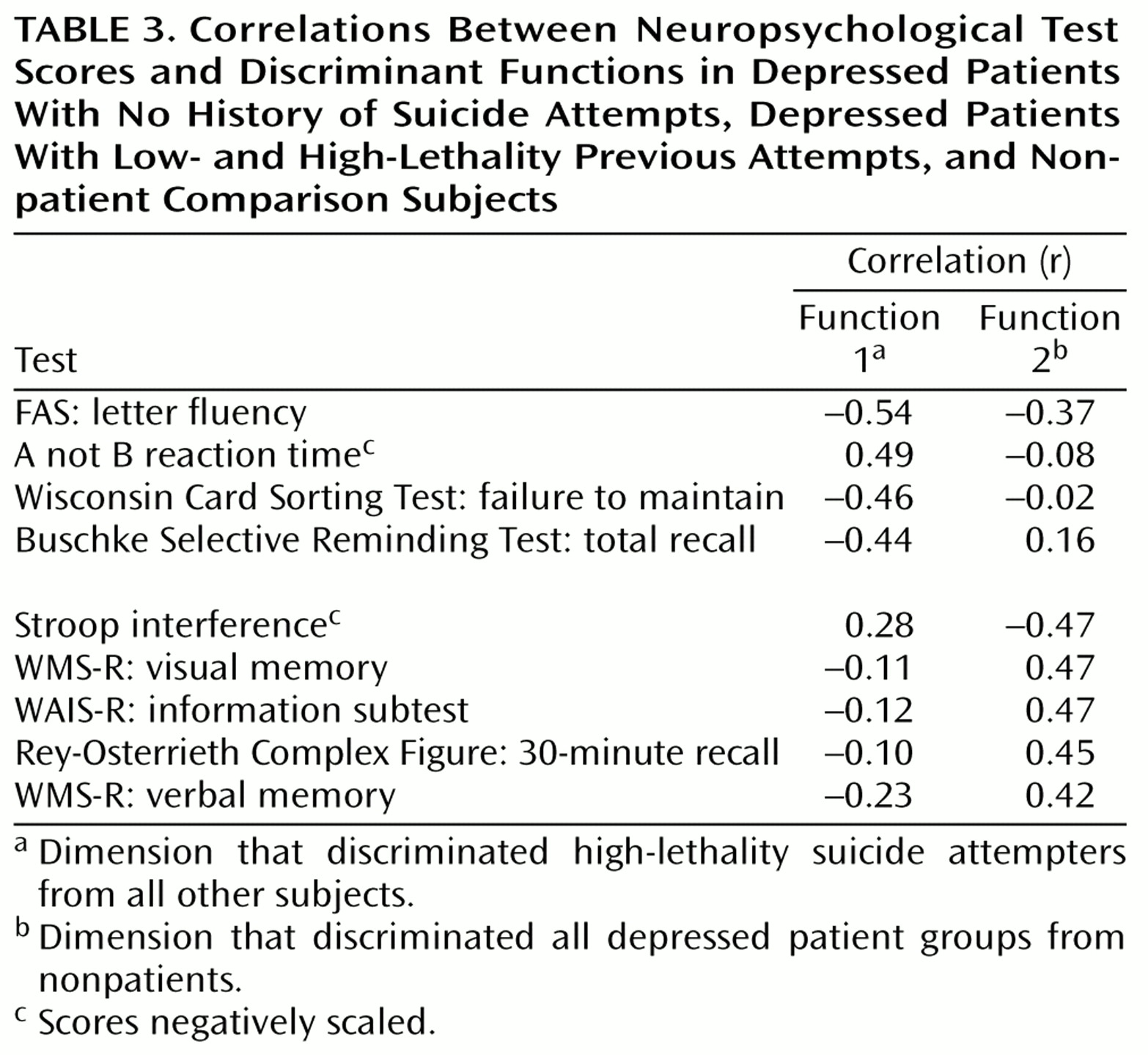
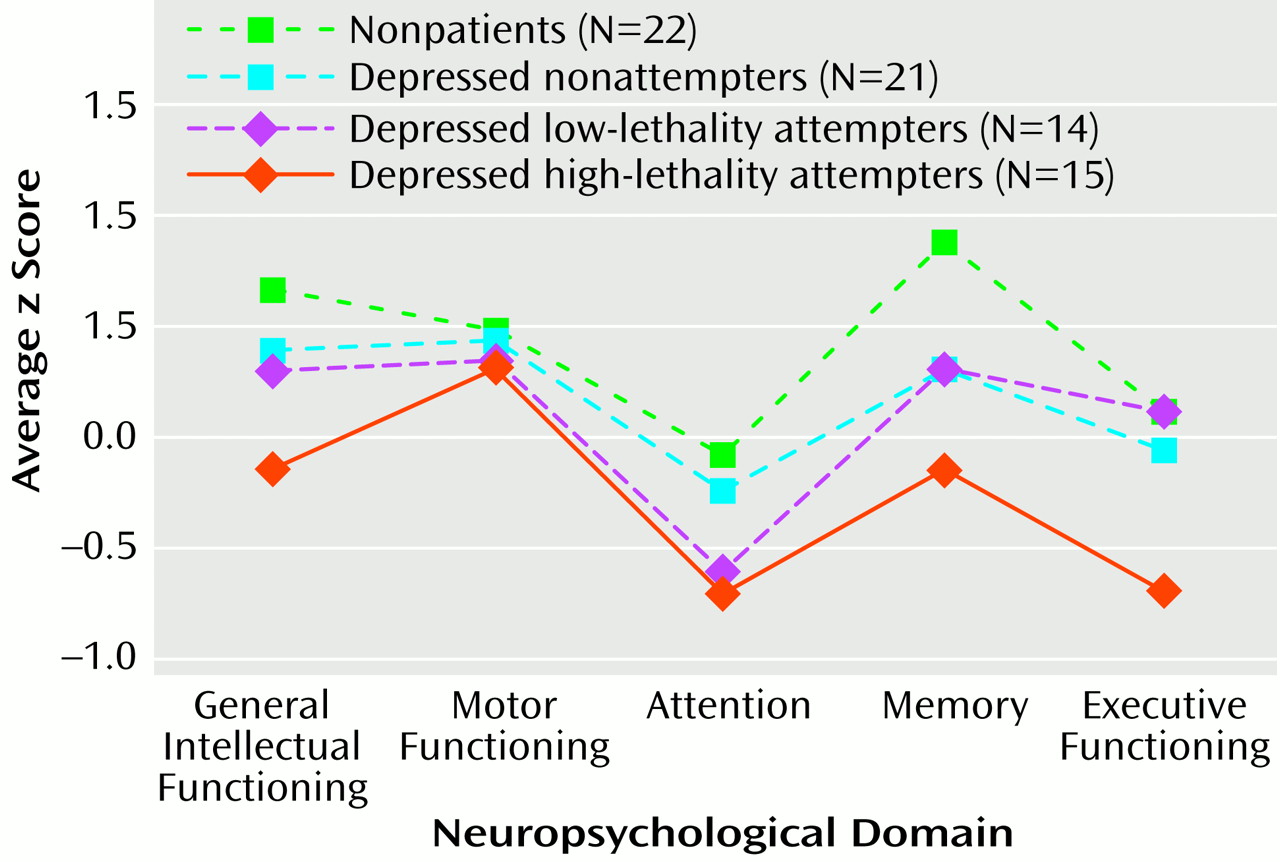
Subjects with a history of high-lethality suicide attempts exhibited deficits in executive functioning that were independent of deficits associated with depression alone. These deficits could not be explained by differences in prior education, occupational attainment, or apparent intellectual capacity (e.g., WAIS-R vocabulary scores), which were comparable across groups. Nor were these deficits accounted for by depression severity. In supplementary analyses, findings were maintained when analyses were restricted to nonpatients and inpatient depressed subjects and were not affected by gender distribution. If scores on the Hamilton depression scale or Beck Depression Inventory were covaried in analyses of domain scores, differences in general intellectual functioning, attention, and memory became nonsignificant, but differences in executive functioning remained (with Hamilton depression scale score as covariate: F=4.11, df=1, 67, p=0.01; with Beck Depression Inventory score as covariate: F=3.63, df=1, 67, p=0.02). The independence of these deficits from depression severity was evident in the results of the discriminant analysis as well. The first discriminant function, which was primarily associated with performance on executive functioning tasks, was uncorrelated with depression severity measures (Hamilton depression scale: r
s=0.06, p=0.61; Beck Depression Inventory: r
s=0.07, p=0.55). However, the second discriminant function, associated with performance on attention and memory tasks, was significantly correlated with both (r
s=–0.45, p<0.001, and r
s=–0.41, p<0.001, respectively). Discriminant function analysis maximizes group differences by using available data, but the dimensions extracted, and their association with high-lethality attempt status versus depression alone, are consistent with previous research. Impairments of fluency and logical reasoning have been found in
(16) or suggested by
(6–
13) prior studies of suicide attempters, while impairments of attention and memory are common in depression
(25–
27). The Buschke Selective Reminding Test is a memory task that discriminated high-lethality attempters, but it has stronger encoding/learning demands than other memory measures
(41,
42). Deficits in high-lethality attempters, then, might best be characterized in terms of these subjects’ difficulties on tasks requiring organization and focused effort, a specific realm of executive functioning
(47).
Neuropsychologically, deficits found in high-lethality attempters were consistent with prefrontal cortical dysfunction, even though these subjects were not more impaired on a number of measures commonly used to characterize prefrontal cortical dysfunction in psychiatric disease (e.g., number of categories or perseverative error scores on the Wisconsin Card Sorting Test, Trail Making Test performance). These commonly used measures tend to be more sensitive to dysfunction in superior prefrontal regions
(48), whereas the deficits found in high-lethality attempters—in language fluency, verbally mediated logical reasoning, and verbal learning—are consistent with dysfunction in inferior prefrontal subregions
(49–
51). Even on the Wisconsin Card Sorting Test, the failure to maintain score, which discriminated high-lethality attempters, loads on a separate factor from other Wisconsin Card Sorting Test scores
(52,
53) and assesses a function that is most commonly associated with inferior prefrontal damage
(54). The potential association between high-lethality attempters’ deficits and inferior prefrontal cortical dysfunction is consistent with autoradiographic postmortem studies of suicide completers that have found specific receptor abnormalities in the inferior but not superior prefrontal cortex
(55).
It is possible that brain damage resulting from high-lethality suicide attempts produced additional impairments. High-lethality past attempters in this study showed a modest deficit in general intellectual performance and impairment on a number of tests of mental efficiency and complex mental operations similar to that resulting from diffuse brain damage
(56). However, high-lethality attempters did not perform more poorly than other depressed groups on measures that are typically most sensitive to diffuse brain dysfunction
(42,
56), especially that produced by hypoxia
(57). These include measures of motor speed (finger tapping and choice reaction time) and psychomotor functioning (WAIS-R Digit Symbol subtest and Trail Making Test). Although brain damage effects cannot be ruled out completely, high-lethality attempters’ deficits are not typical of the type of damage resulting from nonspecific cerebral insult.
Given the study group sizes here, statistical power was limited for comparisons of four groups across five domains of functioning. The data enabled us to identify impairment dimensions related to high-lethality attempter status and depression, but larger samples are needed to validate and refine these neuropsychological profiles.
In spite of these limitations, these data suggest that neuropsychological dysfunction may play a role in determining risk for highly lethal suicidal acts. Although one recent study of geriatric patients found that mental status examination scores alone did not predict lethality of suicide attempts
(58), studies of adolescent samples have found a higher incidence of premorbid attention disorders
(59) in those making more lethal attempts as well as reduced communicativeness
(60). Neuropsychological dysfunction may contribute to risk by impairing decision making during acute psychiatric crises or may reflect neurobiological abnormalities associated with risk
(54). At least one study of cognitive performance in remitted past attempters suggests that deficits may resolve with treatment
(61), but to our knowledge there are no studies that used a comprehensive battery of tests to determine if relative patterns of strengths and weaknesses can still be detected following successful treatment of depression. Prospective longitudinal studies are needed to better assess the contribution of neuropsychological dysfunction to suicide risk as well as its interaction with other risk indicators.