Eleven
(4,
5,
9–
11,
14,
15,
17,
20,
22,
23) of these 22 studies were retrospective in design. Seven were cross-sectional
(3,
8,
12,
13,
16,
19,
21). The four prospective studies
(2,
6,
7,
18) had relatively small numbers of subjects (N=50, N=88, N=70, and N=106, respectively). The difference in study results was independent of study design and of subjects’ diagnosis. Of the 10 studies of suicide completion, only three found a positive association with delusions or psychosis
(4,
6,
11); two of the three were retrospective, and the third did not control for severity of depression.
We decided to study this question because of the importance many clinicians place on the presence of delusions when assessing suicidality, despite the inconclusive reports in the literature. The present study involved 223 patients with major depression, 150 with schizophrenia, and 56 with bipolar disorder. Our goal was to determine whether there is an association between delusions and a history of suicide attempt. The study used direct assessment of patients with standardized instruments.
Method
Subjects
After admission for inpatient or outpatient treatment to research units at New York State Psychiatric Institute or Western Psychiatric Institute and Clinic, 429 patients (376 inpatients and 53 outpatients) were recruited. All patients had physical examinations and routine blood tests, including a urine toxicology test. Exclusion criteria included current substance or alcohol abuse, neurological illness, or active medical conditions. The age range of the patients in the study group was 14–72 years (mean=35.1 years, SD=11.6); 47.6% of the subjects were male (N=204), and 69.9% were Caucasian (N=300). After complete description of the study, all subjects gave written informed consent for the protocol as approved by the institutional review boards of the two study sites.
In the total study group, 212 subjects (49.4%) had a history of a suicide attempt. A suicide attempt was defined as a self-destructive act carried out with at least some intent to end one’s life. Attempters and nonattempters were comparable in terms of axis I diagnoses: 223 subjects (52.0%) in the total study group had major depression (117 attempters and 106 nonattempters); 150 (35.0%) had schizophrenia (70 attempters and 80 nonattempters); and 56 (13.1%) had bipolar disorder (25 attempters and 31 nonattempters).
It should be noted that data for subjects from two different institutions were included in the analysis. To investigate whether site (New York versus Pittsburgh) exerted a significant effect on the relationship between delusions and suicide attempter status, we did a logistic regression analysis using data from the entire study group (N=429). The dependent variable was attempter status, and the independent variables were age, sex, presence of delusions, diagnosis, site (New York versus Pittsburgh), interaction of delusions with diagnosis, and interaction of delusions with site. The results showed that neither site (B=–0.07, p=0.81) nor the interaction of delusions with site (B=0.56, p=0.23) had a significant effect on the relationship between delusions and attempter status. Additional formal tests and graphical methods showed no evidence of a site effect on the relationship between delusions and attempter status, the presence of suicidal ideation before and on admission, and lifetime number of suicide attempts. Therefore, this study assumed that the data for subjects from the two sites could be analyzed together.
In this regression model, no covariate reached significance. However, the interaction of delusions with diagnosis approached significance (B=0.58, p=0.06). Therefore, further analyses were done for diagnostically specific groups.
Measures
Diagnoses were made with the Structured Clinical Interview for DSM-III-R
(24) or the Diagnostic Interview for Genetic Studies
(25). Psychiatric symptoms were assessed with the Brief Psychiatric Rating Scale (BPRS)
(26) and the Global Assessment Scale (GAS)
(27), with scores calculated without consideraton of suicidal ideation. Depressive symptoms were assessed with the 17-item Hamilton Depression Rating Scale
(28), excluding items for depersonalization, derealization, and paranoid symptoms. Psychotic symptoms were assessed with the Scale for the Assessment of Positive Symptoms (SAPS)
(29) and the Modified Scale for the Assessment of Negative Symptoms (SANS)
(30). Suicidal ideation during the 2 weeks before and at the time of hospital admission was assessed with the 19-item Scale for Suicide Ideation (each item scored 0–2, with 0 representing less and 2 representing more severe suicidal ideation)
(31). Lethality of the most recent attempt and maximum lethality of all past attempts were rated with the Medical Lethality Scale (scored 0–8, with 0 representing no medical harm and 8 representing death)
(32). Raters were trained master’s- or doctoral-level nurses, social workers, or psychologists. Interrater agreement and intraclass coefficients were in the good-to-excellent range and have been reported elsewhere
(1).
Statistical Methods
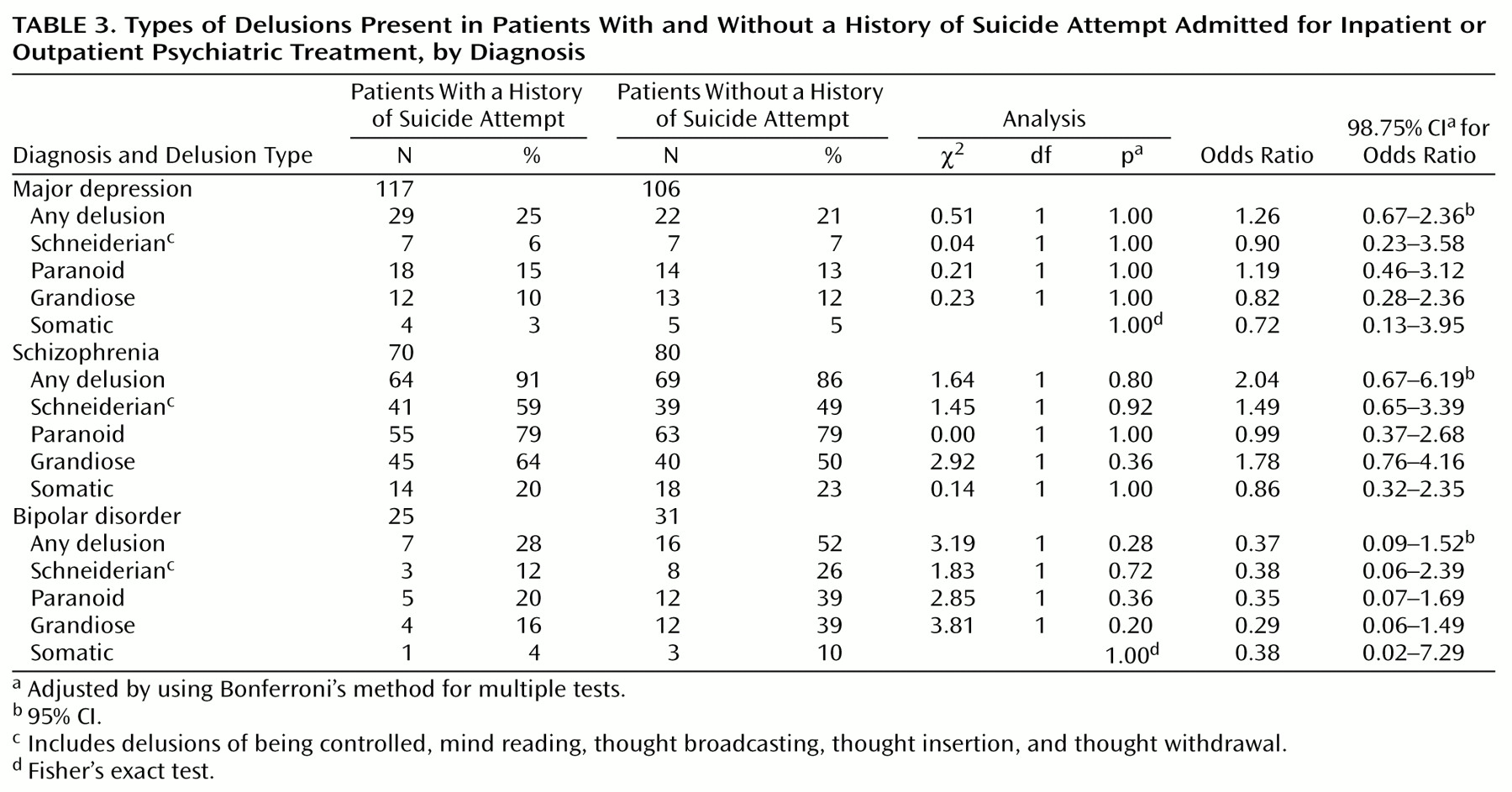
Differences between suicide attempters and nonattempters were tested with t tests for quantitative variables and chi-square tests for categorical variables. For the purpose of data reduction, the 12 delusion types in the SAPS were grouped into four clusters similar to those reported by Peralta and Cuesta
(33) in a factor analysis of the SAPS with a group of 660 psychotic inpatients. These clusters were as follows: 1) Schneiderian delusions, including delusions of being controlled, mind reading, thought broadcasting, thought insertion, and thought withdrawal; 2) paranoid delusions, including delusions of persecution, jealousy, and reference;
3) grandiose delusions, including religious delusions and delusions of guilt or sin; and 4) somatic delusions. We converted the 12 SAPS delusion types and the four delusion clusters into dichotomous variables for the purpose of data analysis, with a SAPS rating of 2 (mild) or greater required for the delusion to be rated as present. Logistic regression analysis was used to examine the relationship of the four delusion clusters with attempter status. Odds ratios and 98.75% confidence intervals (corrected for the four variables by using Bonferroni’s method) were calculated to show the strength of the relationship between attempter status and the dichotomous delusion variables. Logistic regression analysis with interaction variables was used to test for an interaction between delusions and diagnosis in relationship to attempter status.
Delusional and nondelusional patients were also compared in terms of the degree of suicidal ideation during the 2 weeks preceding and at the time of hospitalization as well as on the lethality and total number of past suicide attempts. Variables were tested in both bivariate tests and in multivariate regression models to study the relationships between potential predictors and suicidal ideation and behavior.
Results
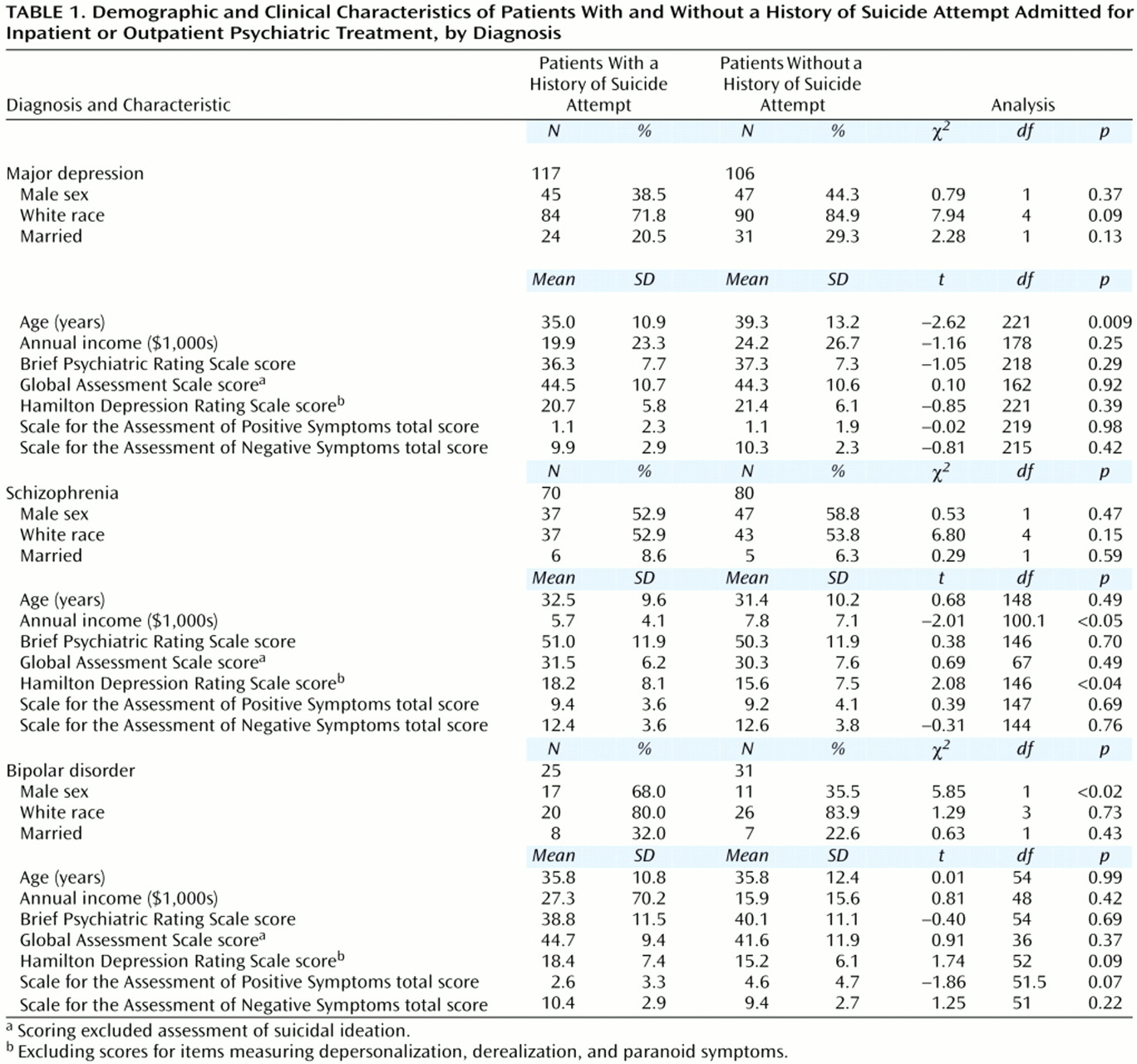
Bivariate analyses with the Bonferroni correction for multiple tests (significance set at p<0.005) showed no significant differences between suicide attempters and nonattempters in age, sex, race, marital status, income, or mean scores on the BPRS, GAS without suicidal ideation, Hamilton depression scale, SAPS, or SANS (
Table 1).
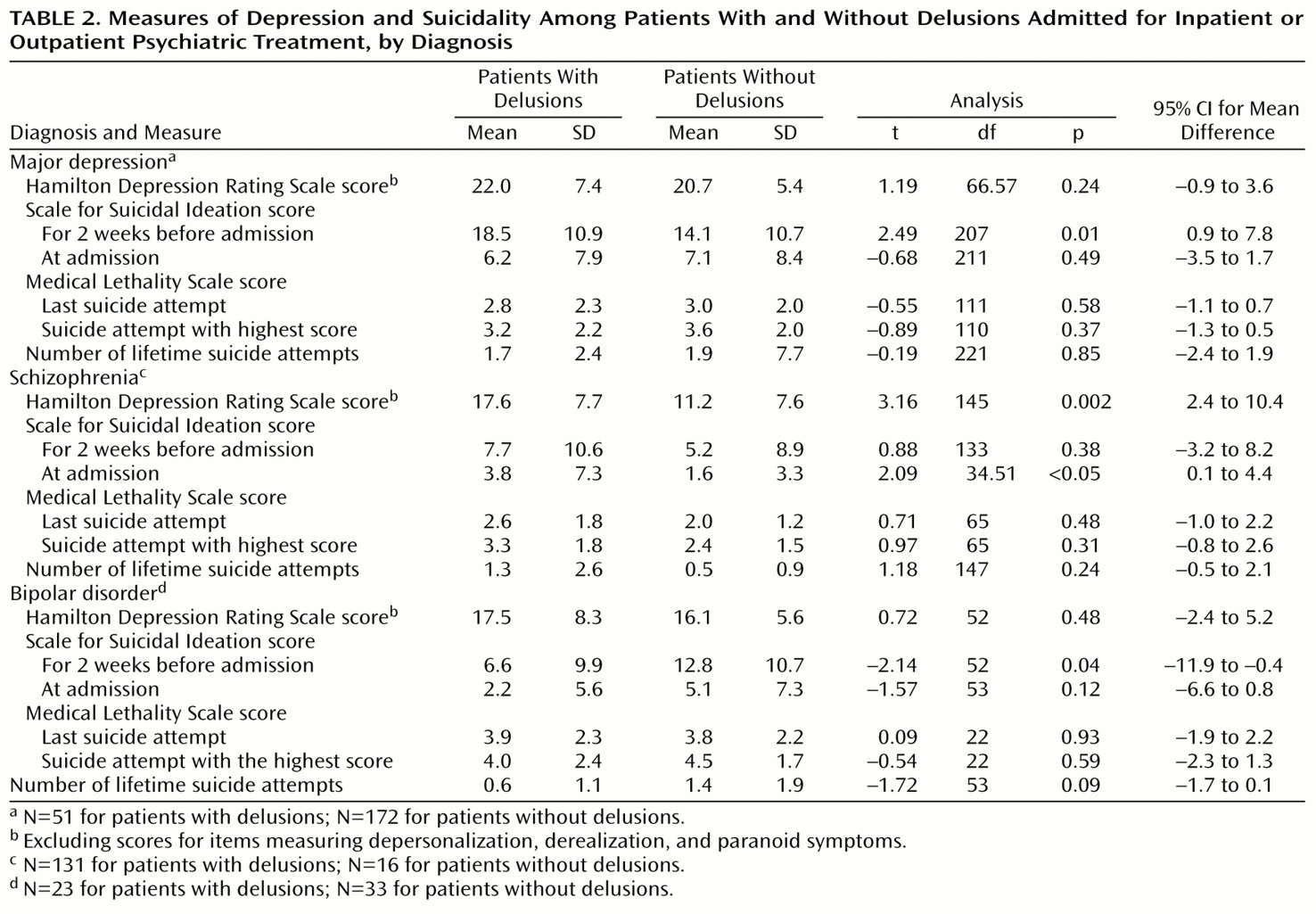
In the subgroup with major depression, bivariate analysis showed that patients with delusions had significantly more severe suicidal ideation than those without delusions during the 2 weeks preceding hospitalization (
Table 2). However, a linear regression analysis with age and presence of delusions as the independent variables showed that more severe suicidal ideation in the 2 weeks before hospitalization was associated only with younger age (t=–4.52, df=205, p<0.0005). Specific delusion types in the subgroup with major depression were not associated with attempter status (
Table 3), and the presence of delusions was not associated with the lethality or number of lifetime suicide attempts (
Table 2). A power analysis showed a 97% chance of detecting a 30% difference in suicide attempt rates by using a chi-square test with an alpha level of 0.05 to compare 51 patients with major depression who had delusions and 172 who did not.
In the subgroup with schizophrenia, bivariate analysis showed that patients with delusions had more severe suicidal ideation at the time of admission than those without delusions, but were also significantly more depressed, as measured by Hamilton depression scale (
Table 2). The GAS score, excluding suicidality, was negatively correlated with suicidal ideation on hospital admission in this group (r=–0.31, N=64, p<0.02). Bivariate analysis of the 12 delusion types in the SAPS showed that guilty delusions were associated with more severe suicidal ideation 2 weeks before hospitalization (t=2.74, df=134, p=0.007, uncorrected for multiple tests) and with a history of suicide attempt (χ
2=5.75, df=1, p<0.02, uncorrected for multiple tests). (Bonferroni correction would set the significance level at p<0.004.) A linear regression analysis with suicidal ideation on admission as the dependent variable and Hamilton depression scale score, GAS score, and presence of delusions as the independent variables showed only one significant association, between suicidal ideation and Hamilton depression scale score (t=2.32, df=58, p<0.03). Like the group with major depression, the group with schizophrenia showed no association between the presence or absence of delusions and the lethality or number of suicide attempts (
Table 2). A power analysis showed a 63% chance of detecting a 30% difference in suicide attempt rates by using a chi-square test with an alpha level of 0.05 to compare 133 patients with schizophrenia who had delusions and 16 who did not.
In the subgroup of patients with bipolar disorder, bivariate analysis showed that those with delusions had less severe suicidal ideation than nondelusional patients during the 2 weeks before hospitalization (
Table 2). Bivariate analysis of the 12 delusion types in the SAPS showed that grandiose delusions were associated with less severe suicidal ideation in the 2 weeks before hospitalization (t=–2.49, df=15.12, p<0.03, uncorrected for multiple comparisons) (no other delusion type was associated with suicidal ideation). In a linear regression analysis with suicidal ideation during the 2 weeks before hospitalization as the dependent variable and age, sex, race, and presence of delusions as the independent variables, there was a significant association of suicidal ideation with delusions, with delusional subjects tending to have less severe suicidal ideation (t=2.28, df=48, p<0.03). However, when this analysis was repeated with data from only those patients with mixed or depressed symptoms (N=37) and with data from only those with hypomanic or manic symptoms (N=16), the association was no longer statistically significant. In fact, patients with bipolar disorder who had a depressed or mixed episode with delusions were significantly more depressed, as measured by Hamilton depression scale, than those without delusions (t=3.6, df=33, p=0.001). A power analysis showed a 60% chance of detecting a 30% difference in suicide attempt rates by using a chi-square test with an alpha level of 0.05 to compare 23 patients with bipolar disorder who had delusions and 33 who did not.
Discussion
The main result of this study is that multivariate analyses did not find an association of delusions at the time of admission with current or recent suicidal ideation or past suicide attempts across the diagnostic groups. Our study adds to the literature (approximately half of studies published since 1982) that does not find such an association. We did not study the association with completed suicide and cannot rule out the possibility that some types of delusions predict future suicide. However, only three of 10 published studies found a relationship of completed suicide to delusions.
Five of the nine studies of delusional depression and suicide risk published since 1982 found a positive association of delusions with either suicidal ideation or behavior
(5,
8,
9,
11,
12). Of these, three were retrospective chart reviews
(5,
9,
11). One cross-sectional study had a sample of only 23 patients with delusions, and this group was more depressed, as measured by the Hamilton depression scale score, than the nondelusional group
(8). In the cross-sectional study by Thakur et al.
(12), which involved 189 patients with delusional depression and 485 with nondelusional depression, the association of delusions with suicidal ideation found in bivariate analyses did not hold up in a multiple logistic regression analysis.
Five
(2–
4,
7,
10) of the 10 studies of delusions and suicide risk in schizophrenia published since 1982 found a positive association of delusions or psychosis with either suicidal ideation or behavior. However, two of these were retrospective studies
(4,
10), two
(2,
7) had relatively small samples (N=50 and N=35, respectively), and one
(3) did not control for severity of depression.
In the subgroup of patients with schizophrenia in our study, there was a significant association between delusions and suicidal ideation on hospital admission. There was no association between delusions and a history of suicide attempts; however, this result may have been related to the high prevalence of delusions (89%) among the patients with schizophrenia. Moreover, the risk for suicidal ideation conferred by delusions could not be separated from the risk conferred by severity of depression as measured by the Hamilton depression scale. The results suggest that depression may be the most important factor associated with risk for suicidal ideation in schizophrenia. This finding highlights the need for aggressive treatment of depression in persons with both disorders.
The only other published study of delusions and suicidality that included patients with bipolar disorder (depressed phase), to our knowledge, found no association between delusions and suicidal ideation
(16). Our finding (controlling for age, sex, and race) that patients with bipolar disorder who had delusions on admission had less suicidal ideation during the prior 2 weeks than those without delusions may be due to a protective effect of grandiose delusions. It is consistent with our recently published study of a smaller group of subjects that found lower SAPS scores among patients with bipolar disorder who had attempted suicide than among those who had not, although the difference did not reach statistical significance
(34). However, studies with larger subject groups will be required before any firm conclusions can be drawn. That patients with bipolar disorder in a depressed or mixed episode who are delusional were more depressed than those without delusions suggests that this group may be at greater risk for self-harm, although we could not demonstrate this association.
Our findings should be interpreted in light of a number of limitations. Most of the subjects were patients referred to urban university-affiliated research hospitals, and the results may not be generalizable to other populations. The study also tested the association of current delusions with past suicide attempts and with recent or current suicidal ideation. Last, for the purposes of addressing a specific issue of clinical debate, the study restricted itself to a focus on delusions and their effect on suicidality. We did not find that overall degree of psychosis, or of negative symptoms in particular, distinguished persons with or without a history of suicide attempt (
Table 1). However, the study did not specifically examine hallucinations or other psychotic or negative symptoms. These topics will be explored in future reports.
It is important to note that substance abuse and significant medical illness were exclusion criteria. Thus, the study patients may not represent community populations in terms of the prevalence of these comorbid conditions. If substance abuse and medical illness mediate the interaction of delusions with suicidality, our study would not have been able to detect this effect.
Furthermore, it should be noted that the study had substantial power to detect a 30% difference in suicide attempt history rates between delusional and nondelusional subjects in the subgroup with major depression but only modest power for the subgroups with schizophrenia and bipolar disorder. Our results for patients with bipolar disorder and the finding (before Bonferroni correction) of an association between more severe suicidal ideation and delusions of guilt among patients with schizophrenia will require further investigation in larger groups of subjects.
Despite these limitations, however, the study findings add to existing evidence that, in general, delusions do not constitute an independent risk factor for current suicidal ideation or past suicide attempts. Additional research, including replication of the current results and a prospective study in a larger study group, is required to provide a definitive answer to the question of whether delusions predict future suicide attempts.