Apathy is a term coined by the Greek Stoic philosophers to refer to the condition of being free from emotions and passions, such as fear, pain, desire, and pleasure. In the neuropsychiatric literature, apathy has been defined as the absence or lack of feeling, emotion, interest, concern, or motivation not attributable to a decreased level of consciousness, cognitive impairment, or emotional distress
(1,
2). Among neurological disorders, apathy was reported to be highly frequent in patients with stroke, Parkinson’s disease, Alzheimer’s disease, or traumatic brain injury
(3–
10). An important methodological limitation is the lack of valid and reliable diagnostic criteria, as well as structured interviews for apathy. Some authors have reported correlations between apathy and other behavioral scores, but they did not categorize patients by whether they were apathetic
(6), whereas other studies have diagnosed apathy on the basis of arbitrary cutoff scores on apathy scales
(3–
5).
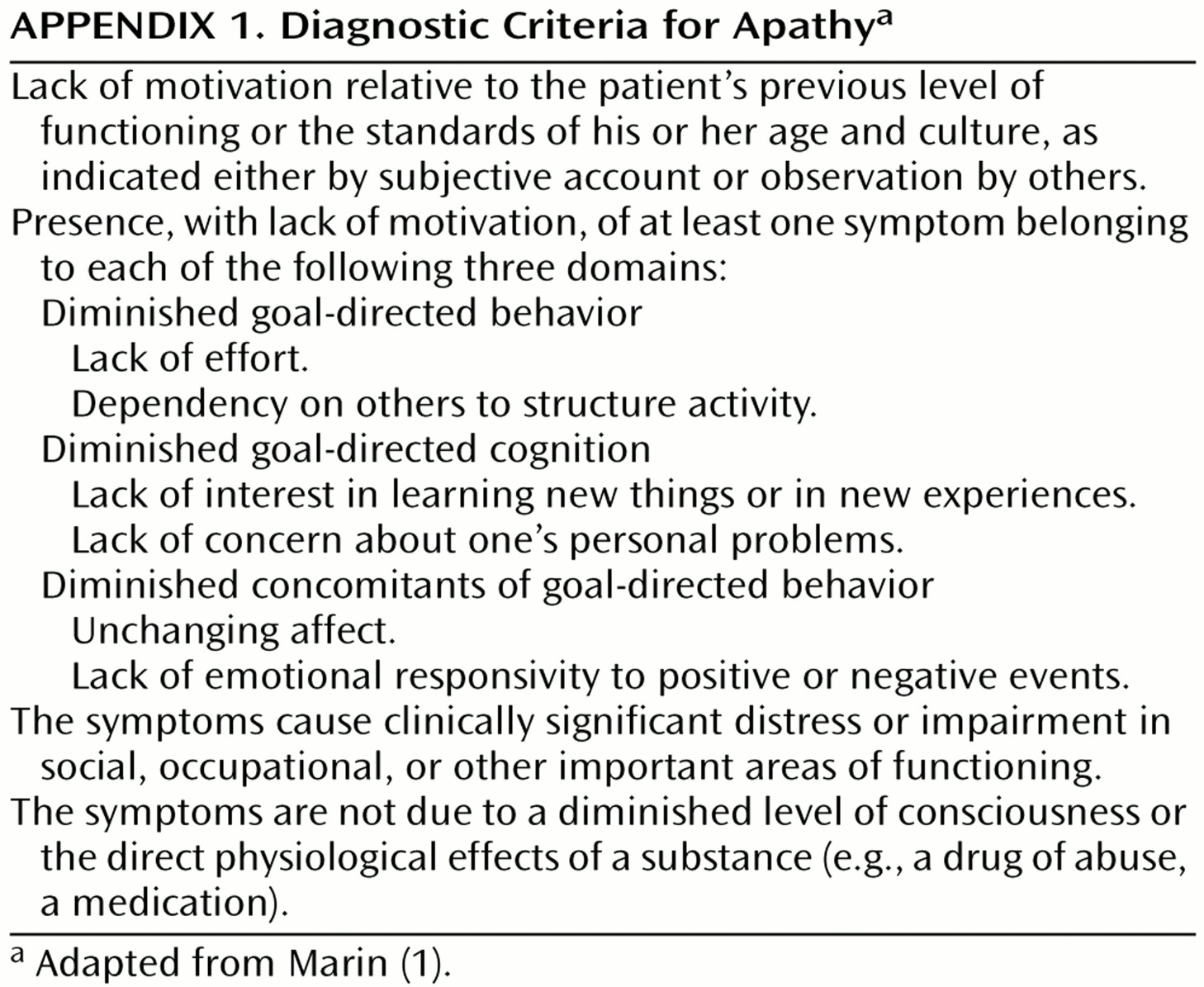
The present study had several aims. The first aim was to examine the usefulness of and provide partial validation for Marin’s criteria for apathy
(1). Since apathy has been identified as a frequent behavioral change in Alzheimer’s disease, we expected Marin’s criteria to demonstrate a significantly higher frequency of apathy in Alzheimer’s disease patients, compared to healthy comparison subjects. Finding a group of Alzheimer’s disease patients who met Marin’s criteria for apathy but not the DSM-IV criteria for depression would provide further validity. A second aim was to examine the related diagnostic problem of whether Alzheimer’s disease patients are able to provide a reliable account of apathy symptoms. To examine this issue, we assessed with the same apathy scale both the patients and their respective caregivers. Since the overlap of apathy and depression in Alzheimer’s disease may result from either the association of apathy and a specific type of depression or from an interaction between depression and the dementing process, we separated depressed Alzheimer’s disease patients into those with major or minor depression, and also assessed apathy in a consecutive series of nondemented patients with primary depression (i.e., no known brain injury). The final aim was to further validate the syndrome of apathy by examining whether Alzheimer’s disease patients who met the criteria for apathy had specific demographic or clinical correlates.
Results
Frequency of Apathy
Forty-two (13.2%) of the 319 Alzheimer’s disease patients had apathy only (i.e., without depression), compared to none of the 36 healthy comparison subjects (χ2=10.7, df=1, p<0.001). Depression and apathy were both present in 75 Alzheimer’s disease patients (23.5%), whereas 69 Alzheimer’s disease patients (21.6%) had depression but no apathy, and the remaining 133 Alzheimer’s disease patients (41.7%) had neither apathy nor depression. Minor depression was diagnosed in 58 of the 144 depressed Alzheimer’s disease patients (40.3%), whereas the remaining 86 (59.7%) had major depression. The Alzheimer’s disease patients with either major or minor depression showed a significantly higher frequency of apathy, compared to those without depression (51.2%, N=44; 53.4%, N=31; and 24.0%, N=42; respectively) (χ2=26.9, df=2, p<0.0001).
Apathy was present in 35 of the 95 nondemented patients with major depression (36.8%), compared with two of the 22 nondemented patients with minor depression (9.1%) (χ2=6.36, df=1, p=0.01). The frequency of apathy in the Alzheimer’s disease patients with major depression was significantly higher than in the nondemented patients with major depression (51.2%, N=44, and 36.8%, N=35, respectively) (χ2=3.76, df=1, p=0.05). Similarly, the Alzheimer’s disease patients with minor depression had a significantly higher frequency of apathy, compared to the nondemented patients with minor depression (53.4%, N=31, and 9.1%, N=2, respectively) (χ2=12.9, df=1, p<0.001).
Clinical Correlates of Apathy in Alzheimer’s Disease
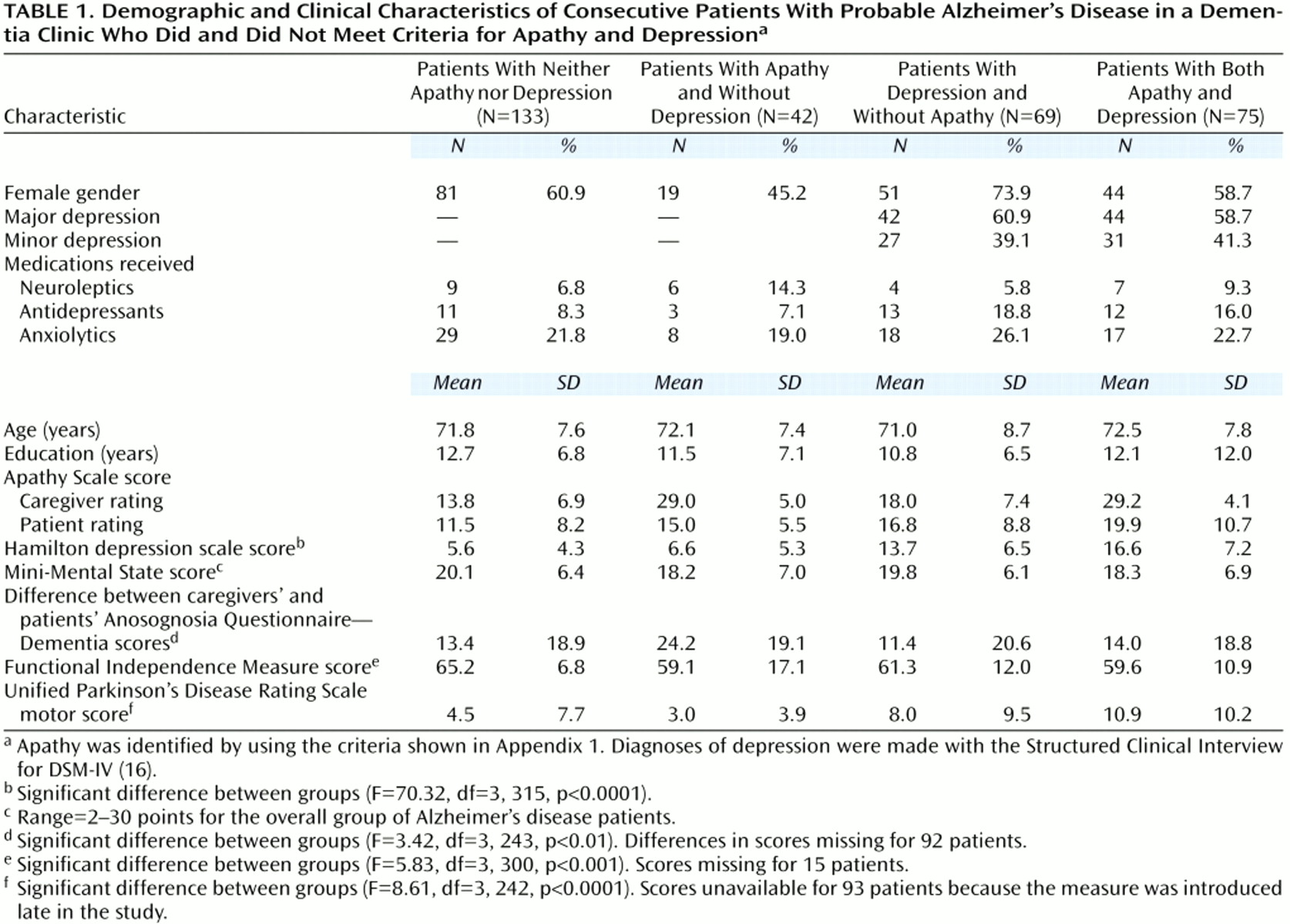
We examined significant differences in demographic and clinical variables between the four Alzheimer’s disease groups. There were no significant between-group differences in age, gender, or education, or in the proportion of patients who received neuroleptics, antidepressants, or anxiolytics (
Table 1). Hamilton depression scale scores were significantly different between groups (
Table 1). Post hoc tests showed that both depressed Alzheimer’s disease groups (with or without apathy) had significantly higher depression scores than the two nondepressed Alzheimer’s disease groups (p<0.0001, Tukey). There were no significant differences in Hamilton depression scale scores between the two depressed Alzheimer’s disease groups and between the two nondepressed Alzheimer’s disease groups (with or without apathy). There was an expected significant between-group difference in apathy scale scores (F=127.2, df=3, 315, p<0.0001). Post hoc tests showed that the Alzheimer’s disease patients with apathy (with or without depression) had significantly higher scores than those without apathy (p<0.0001, Tukey), and that the depressed Alzheimer’s disease patients without apathy had significantly higher apathy scores than the Alzheimer’s disease patients with neither apathy nor depression (p<0.05, Tukey). There was a significant effect for Functional Independence Measure scores (
Table 1). The Alzheimer’s disease patients with apathy (with or without depression) had significantly more severe impairments in activities of daily living than those with neither apathy nor depression (p<0.01 and p<0.05, Tukey, respectively). Finally, there was a significant effect for Unified Parkinson’s Disease Rating Scale motor scores (
Table 1). The Alzheimer’s disease patients with both apathy and depression (N=50) had significantly higher scores for extrapyramidal symptoms than nondepressed Alzheimer’s disease patients with apathy (N=29) (p<0.01, Tukey) or without apathy (N=104) (p<0.001, Tukey) (effect sizes 1.1 and 0.7, respectively) (
Table 1).
A stepwise regression analysis that included apathy scale scores (rated by the caregiver) as the dependent variable, and age, Mini-Mental State score, and Hamilton depression scale score as the independent variables showed a significant correlation for all three comparisons (Hamilton depression scale score: R2=0.12, N=319, p<0.0001; Mini-Mental State score: R2=0.04, N=319, p<0.001, and age: R2=0.02, N=319, p<0.05).
Clinical Correlates of Apathy in Primary Depression
There were no significant differences in demographic variables between depressed patients with or without apathy, but patients with major depression and apathy had significantly higher Hamilton depression scale scores than those without apathy (mean Hamilton depression scale scores 24.4, SD=5.0, and mean=19.7, SD=5.9, respectively) (t=3.87, df=93, p<0.001, effect size=0.8). Patients with major depression had significantly lower Mini-Mental State scores than patients with minor depression, but patients with major depression, regardless of whether they had apathy, had similar Mini-Mental State scores (major depression and apathy: mean=24.0, SD=5.9; major depression without apathy: mean=25.7, SD=3.6; minor depression and apathy: mean=29.5, SD=0.7; minor depression without apathy: mean=28.0, SD=1.3). Nineteen patients with major depression and apathy (20.0%) received antidepressant medications.
Awareness of Apathy in Alzheimer’s Disease
Since Alzheimer’s disease patients have been reported to underrate their own cognitive deficits and behavioral problems
(19), we examined discrepancies in apathy scale scores obtained in separate interviews from the Alzheimer’s disease patients and their respective caregivers. The last 97 Alzheimer’s disease patients from our present series were assessed with the apathy scale by a psychiatrist who was blind to their respective caregivers’ ratings. A one-way ANOVA analyzing the difference between the patients’ and the caregivers’ scores showed a significant effect (F=3.73, df=3, 93, p<0.01). Post hoc tests showed a significantly greater discrepancy in apathy scale scores (caregivers > patients) for the Alzheimer’s disease patients with apathy without depression (N=12) than for the nonapathetic Alzheimer’s disease patients with depression (N=25) (p<0.01, Tukey) or without depression (N=44) (p<0.01, Tukey). The Alzheimer’s disease patients with both depression and apathy (N=16) had a significantly greater discrepancy in apathy scale scores than those with depression only (p<0.05, Tukey). We also examined lack of awareness of cognitive impairments using the Anosognosia Questionnaire—Dementia scores from patients and caregivers. A one-way ANOVA analyzing the difference between caregivers’ and patients’ ratings showed a significant effect (
Table 1). Post hoc tests showed that the Alzheimer’s disease patients with apathy only had a significantly greater discrepancy in Anosognosia Questionnaire—Dementia scores than Alzheimer’s disease patients with depression only (p<0.01, Tukey).
Discussion
We assessed a specific set of clinical criteria for apathy in a large cohort of patients with probable Alzheimer’s disease, in patients with depression but no dementia, and in a group of age-comparable healthy individuals. There were several important findings. First, apathy in the absence of depression was diagnosed in 13% of a consecutive series of 319 patients with Alzheimer’s disease. This prevalence was significantly higher than in a group of 36 healthy individuals. An additional 30% of the Alzheimer’s disease patients had symptoms in two of the three domains of the apathy criteria. Second, apathy in Alzheimer’s disease was significantly associated with more severe impairments in activities of daily living and with patients’ poor insight into their apathy syndrome and cognitive deficits. There was a significant correlation between apathy scores and both age and Mini-Mental State scores (i.e., more severe apathy was significantly correlated with older age and more severe cognitive deficits). Third, the Alzheimer’s disease patients with apathy but not depression and those with neither apathy nor depression had similar depression scores, suggesting that apathy may not artificially increase depression scores. Fourth, the prevalence of apathy in the Alzheimer’s disease patients with minor depression was significantly higher than in the patients without dementia who had minor depression, but the differences were less marked between the Alzheimer’s disease patients with major depression and those with major depression who did not have dementia.
Before further comments, several limitations of our study should be pointed out. First, the assessment of apathy symptoms was based on a rating scale and not on a structured interview. Second, the severity ratings and diagnoses of apathy were both based on the same scale, which may partly account for the higher apathy scale scores in the Alzheimer’s disease groups with apathy. Third, our healthy comparison group consisted of individuals who volunteered to participate in the study, which may account for the lack of apathy in this group. Finally, the group with major depression and no dementia was about 20 years younger than the group with Alzheimer’s disease and depression. Future studies should examine whether age has a specific interaction with apathy and depression in these different populations.
The nosological position of apathy is a debated issue. Marin
(1) discussed different definitions of apathy and proposed specific diagnostic criteria. Using a slightly modified and more structured version of these criteria, we diagnosed apathy in 36% of a consecutive series of patients with Alzheimer’s disease, compared to none of the healthy individuals. Although this finding was expected, it provides partial validation for Marin’s criteria. In our previous study of a smaller sample of Alzheimer’s disease patients, we found a frequency of apathy of 46%
(5), and other studies reported frequencies ranging from 48% to 80%
(2,
7,
21–
23). The present study also demonstrated that most Alzheimer’s disease patients with apathy were also depressed, which replicates our previous finding in a smaller cohort
(5).
To our knowledge, this is the first study to examine the frequency of apathy among patients with primary depression and no dementia, and there were two main findings. First, about one-third of the patients in the study had apathy, and second, this frequency was significantly higher in patients with major depression than in patients with minor depression. Since patients with major depression had significantly lower Mini-Mental State scores than patients with minor depression, cognitive deficits may partly account for the high prevalence of apathy in major depression. On the other hand, patients with major depression with or without apathy had similar Mini-Mental State scores, suggesting that cognitive impairment may be necessary but not sufficient to produce apathy among depressed nondemented individuals. Hyperintensities in T
2-weighted MRI images have been reported to be significantly related to depression
(24), and future studies should examine whether these abnormalities are also associated with apathy or with an apathetic subtype of depression.
Whereas apathy was significantly more prevalent in nondemented patients with major depression than in those with minor depression, Alzheimer’s disease patients with either minor or major depression showed a similar prevalence of apathy. These findings suggest 1) that once depression occurs in Alzheimer’s disease patients, these patients may have a “lower threshold” for apathy, compared to nondemented depressed individuals; and 2) that the high prevalence of apathy in Alzheimer’s disease may result from an interaction between depression and the dementing process.
Given the large overlap of apathy and depression, the question arises of whether apathy is always related to at least subsyndromal depression, which could argue against considering apathy as a specific behavioral syndrome. However, our finding that the Alzheimer’s disease patients with apathy but no depression and those with neither depression nor apathy had similar depression scores supports the validity of apathy as a behavioral syndrome independent from depression. Apathetic Alzheimer’s disease patients (with or without depression) also had significantly more severe impairments in activities of daily living and more severe extrapyramidal signs than nonapathetic Alzheimer’s disease patients, suggesting that apathy may account for some of the functional impairments in Alzheimer’s disease.
There also was an interesting association between apathy and less awareness of behavioral and cognitive changes. When Alzheimer’s disease patients and their respective caregivers were separately assessed with the apathy scale (with caregivers providing reports about patients), the discrepancy in scores (with patients providing lower scores than caregivers) was significantly larger for the nondepressed Alzheimer’s disease patients with apathy than for those without apathy. Similar results were found on the Anosognosia Questionnaire—Dementia, which primarily rates awareness about cognitive impairments. These findings demonstrate that Alzheimer’s disease patients with apathy have only partial awareness of their cognitive and behavioral changes and may provide unreliable answers.