More than a decade ago, the importance of systematic diagnosis of psychiatric disorders and of distinguishing disorders from universal distress following severe traumas was recognized
(1). Postdisaster diagnosis is critical to guiding appropriate treatment
(2). Despite this, posttraumatic stress disorder (PTSD) among rescue workers has usually been addressed with self-report questionnaires that provide symptom counts, not diagnoses
(1,
3,
4).
One prior study
(5) obtained systematic psychiatric diagnoses, reporting PTSD in 13% of firefighters 42 months after a bushfire. Other studies have described a wider range of difficulties—from distress to dysphoria, peritraumatic dissociation, and subjective poor mental health—in 9%–32%
(6–
10). Although not found universally
(4), rescue worker resilience and well-being have been identified following disasters
(7,
8).
The present article describes a systematic diagnostic study of firefighters who served as rescue/recovery workers after the Oklahoma City bombing. Using the same research instruments applied in the assessment of primary victims who had been in the path of the blast
(2) allowed direct comparisons.
Method
Approval was obtained in advance from the Washington University School of Medicine Institutional Review Board. Subjects provided written informed consent. Because authorities disallowed contact with all involved firefighters, a volunteer participant group was recruited. The 824-member Oklahoma City Fire Department was the source for all but 16 of the 181 study participants. The remaining 16 were recruited from the smaller Tinker Air Force Base Fire Department. Fire department administrators delivered letters from the researchers to the firefighters that invited them to participate and included stamped postcards to allow confidential responses. The death of the study’s original principal investigator during the interview period complicated data collection, which spanned 27 months.
Psychopathology both before and after the bombing was assessed retrospectively with the National Institute of Mental Health Diagnostic Interview Schedule (DIS)
(11). The Disaster Supplement
(12) elicited disaster exposure information, including injuries, time spent under the “mother slab” (a precariously hanging 35,000-pound section of roof) and in “the pit” (a depressed area within three-story-high piles of debris in the structure’s most unstable section), and body handling.
It was hypothesized that the firefighters would have lower rates of psychopathology than the survivors of the direct bomb blast because of differences in their exposure to the disaster as well as preexisting characteristics of the populations. Variable time elapsed between the bombing and the assessment because of the long duration of data collection (mean=33.8 months [SD=6.8], median=35, range=15–41) was expected to yield significant effects on reported psychopathology.
Categorical variables were compared with chi-square tests, substituting two-tailed Fisher’s exact tests for expected cell sizes <5 and McNemar tests with continuity correction for repeated measures. Categorical and numeric variables were compared by using t tests. Linear regression analyses compared numeric variables.
Results
Nearly all of the firefighters were male (97%, N=176) and Caucasian (89%, N=161). The mean age of the group was 38.5 years (SD=7.9), and they had on average 13.8 years (SD=1.3) of education. The majority (76%, N=138) were married. Disaster-related injury or illness was reported by 11% (N=20). The number of days participants worked at the disaster site ranged from 1 to 17 (mean=8.2 [SD=4.2], median=7). Most (74%, N=134) had labored under the mother slab and in the pit (84% [N=152]). Time spent working under the mother slab ranged from 15 minutes to 74 hours (mean=14.1 hours [SD=16.6], median=7 hours), and time spent in the pit ranged from 15 minutes to 99 hours (mean=11.1 hours [SD=14.8], median=6 hours).
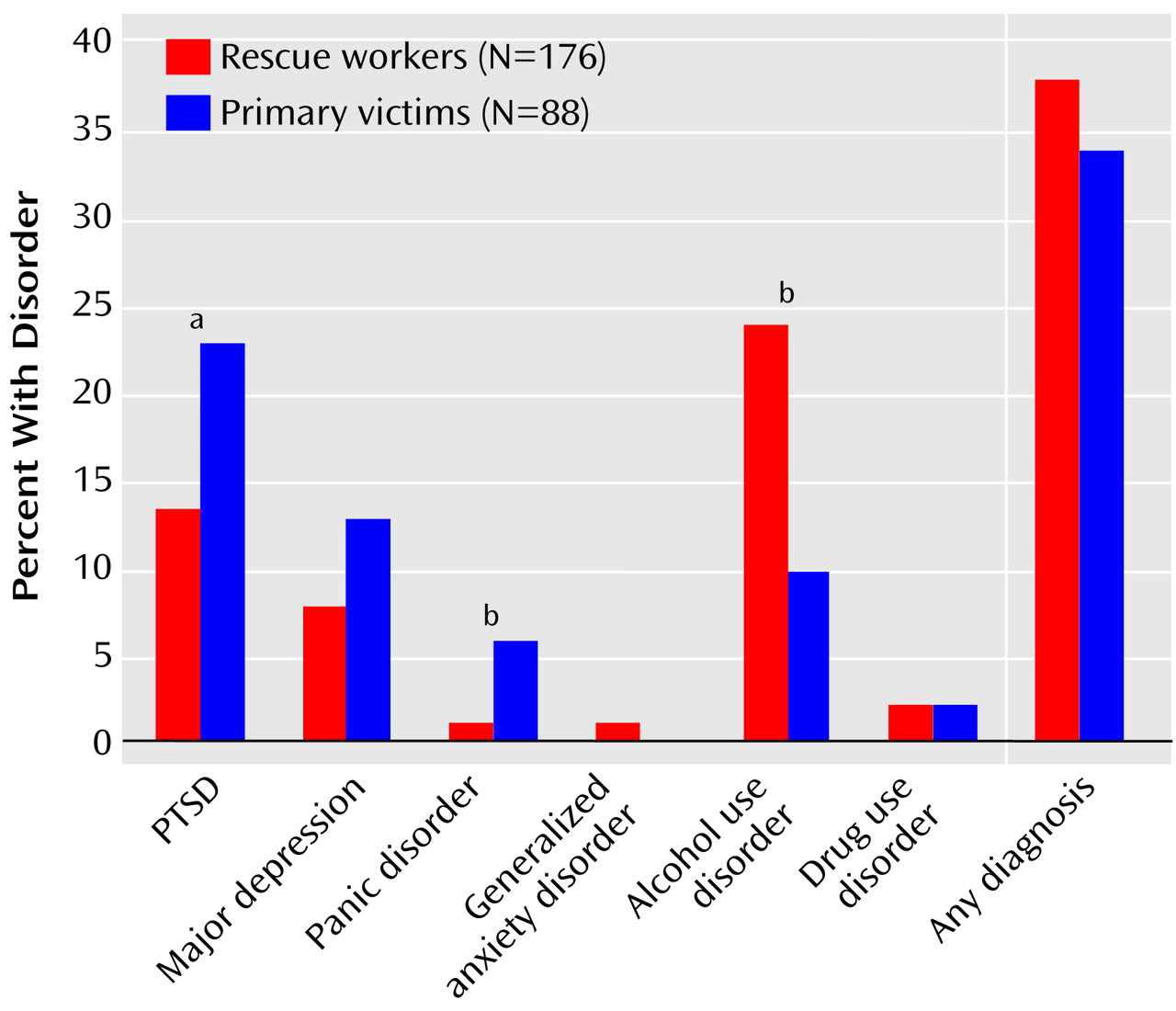
Figure 1 compares postdisaster psychopathology among the male rescue workers and among male primary victims. The rate of posttraumatic stress disorder related to the bombing was significantly lower in male rescue workers (13%, N=22) than in male primary victims (23%, N=20). In addition, the rate of postdisaster panic disorder among the male rescue workers was significantly lower (1% [N=1] compared with 6% [N=5] among the primary victims), and the rate of alcohol use disorder was significantly higher (25% [N=43] versus 10% [N=9], respectively). Among all firefighters, bombing-related PTSD was diagnosed in 13% (N=24), and any postdisaster psychiatric disorder in 38% (N=68). Most prevalent was alcohol abuse/dependence (current: 24% [N=43], lifetime: 47% [N=85]); only 2% (N=3) were new cases emerging after the bombing. More than one-half of the individuals diagnosed with PTSD (54%, N=13) suffered another postdisaster disorder, compared with 27% (N=42) of others (χ
2=7.40, df=1, p=0.007).
Time elapsed from bombing to interview was not associated with PTSD or any psychiatric diagnosis, pre- or postdisaster. PTSD was associated with more time spent at the bombing site (mean=10.0 days [SD=3.8] versus mean=7.9 days [SD=4.1] for those without PTSD) (t=2.41, df=180, p<0.02) and more time spent in the pit (mean=21.7 hours [SD=29.0] versus mean=9.6 hours [SD=11.1] for those without PTSD) (t=2.64, df=89, p=0.01). PTSD was not associated with injury, other exposure, or demographics.
More than one-half (53%, N=96) of the firefighters had a preexisting psychiatric disorder, with alcohol abuse/dependence complicating most (47% of all firefighters, N=85). The majority with any psychiatric disorder after the bombing (82%, N=56) had preexisting psychopathology (versus 35% [N=40] of others) (McNemar χ2=15.07, df=1, p≤0.001). Excluding alcohol diagnoses, the rate of nonalcohol disorders after the bombing was four times higher in those with predisaster psychopathology (43%, N=21 of 49) than in those without predisaster psychopathology (11%, N=14 of 132) (McNemar χ2=4.67, df=1, p<0.05). Last, the rate of bombing-associated PTSD was significantly higher in those with a predisaster diagnosis of PTSD (38%, N=5 of 13) than in those with no predisaster diagnosis of PTSD (12%, N=19 of 168) (p<0.02, Fisher’s exact test).
Discussion
An important strength of this study was the consistent use of a structured diagnostic instrument that allowed for direct comparison with primary victims. Firefighters experienced less PTSD than did direct bomb blast survivors. This may reflect firefighters’ lower injury rates
(2) and reduced vulnerability from selection and self-selection for work entailing trauma exposure, preparedness, experience with routine job-related trauma exposure, and attention to mental health needs through education and debriefing pre- and postbombing. Contrary to expectations, no temporal associations of findings to length of time until assessment could be identified. Preexisting psychopathology strongly predicted general postdisaster psychopathology.
These retrospective data await confirmation in larger, systematically recruited and prospectively assessed, study groups. This study’s volunteer group, representing less than one-fourth of the Oklahoma City firefighters involved, could have underestimated or overestimated their psychopathology, limiting generalizability of findings. Diagnostic stability over the recruitment period, consistent with findings of other research
(6), did not suggest either tendency, however. Nonetheless, this important flaw in the present study’s sampling procedure highlights the critical importance of obtaining direct access to the study population for systematic recruitment of a representative sample.
Nearly one-half of the firefighters qualified for a lifetime diagnosis of alcohol abuse/dependence, which generally predated the disaster. Most postdisaster psychiatric disorders were alcohol-related, leaving only 12% with other disorders alone. Current alcohol problems have been previously described in 29% of firefighters not selected for exposure to disaster
(13). High prevalence of alcohol problems independent of the disaster experience in firefighters suggests the need for ongoing programs related to alcohol abuse/dependence that may be endemic among firefighters.