Childhood sexual abuse is a major public health problem that affects 16% of women in this country at some time before their 18th birthday
(1) and is a common cause of posttraumatic stress disorder (PTSD)
(2,
3). Despite the magnitude of the problem, little is known about possible changes in brain structure and function in abuse-related PTSD. In addition to symptoms such as nightmares, hyperarousal, impaired social functioning, and sleep disturbance, alterations in several facets of memory are a prominent part of the presentation of patients with PTSD. These memory alterations include amnesia, flashbacks, impaired learning and concentration, and intrusive memories. These observations have led to the hypothesis that brain regions involved in memory, including the hippocampus and prefrontal cortex, mediate symptoms of PTSD
(4).
The hippocampus plays a critical role in learning and memory
(5). Patients with hippocampal lesions perform poorly on tests of verbal declarative memory, including tasks involving recall of a paragraph or learning a list of words
(6), with the degree of dysfunction correlating with hippocampal volume and cell loss
(7–
10). Although studies have suggested that the left hippocampus plays a greater role in verbal memory, verbal memory impairment has been shown to be more severe with bilateral hippocampal lesions, compared to unilateral lesions
(10), indicating that both hippocampi play a role in verbal memory.
Studies in animals have shown that the hippocampus is sensitive to stress. Animals exposed to stress showed deficits in hippocampal-based memory function
(11,
12), alterations in hippocampal morphology
(13,
14), and inhibition of neurogenesis (or the growth of new neurons)
(15) that were reversible with treatment
(16). A variety of mechanisms have been proposed for these findings, including elevated levels of glucocorticoids released during stress
(17,
18), stress-related inhibition of brain-derived neurotrophic factor
(19,
20), and changes in serotonergic function
(21), although mechanisms continue to be debated
(22).
These studies led to efforts to determine if stress-induced hippocampal damage is seen in PTSD patients
(23). Patients with PTSD from both combat and early childhood abuse had deficits in verbal declarative memory function, including tasks such as paragraph recall and word list learning
(24–
29). One study found that patients with combat-related PTSD had an 8% reduction in right hippocampal volume, as measured with magnetic resonance imaging (MRI), that was correlated with deficits in memory function
(30). Other studies found smaller left hippocampal volumes in abused women with PTSD
(31,
32) and smaller bilateral hippocampal volumes in patients with combat-related PTSD
(33). Two studies found reduced hippocampal
N-acetylaspartate, a marker of hippocampal integrity, in combat-related PTSD
(34,
35), although one of those studies did not find a corresponding volume reduction
(35). Studies in children
(36,
37) and patients with new-onset PTSD did not find smaller hippocampal volumes
(38). Some studies have also found smaller hippocampal volume in depression, another disorder that has been linked to stress
(39–
41). These studies suggest that deficits in the hippocampus may be associated with chronic PTSD.
Studies of the hippocampus in PTSD have left several unanswered questions. It is not known whether structural changes in the hippocampus are specific to abuse and PTSD or are a nonspecific effect of childhood abuse alone. Although deficits in hippocampal-based verbal declarative memory function measured with neuropsychological testing are suggestive of hippocampal dysfunction, it is not known whether deficits in hippocampal function (best measured with functional neuroimaging in conjunction with the performance of hippocampal-based memory tasks) are associated with PTSD. We therefore conducted a study to look at hippocampal structure (measured with MRI) in women with and without early childhood sexual abuse and with and without the diagnosis of PTSD. We also looked at hippocampal function (with positron emission tomography [PET]) during the performance of verbal declarative memory tasks in women with abuse with and without PTSD.
Method
Subject Recruitment and Assessment
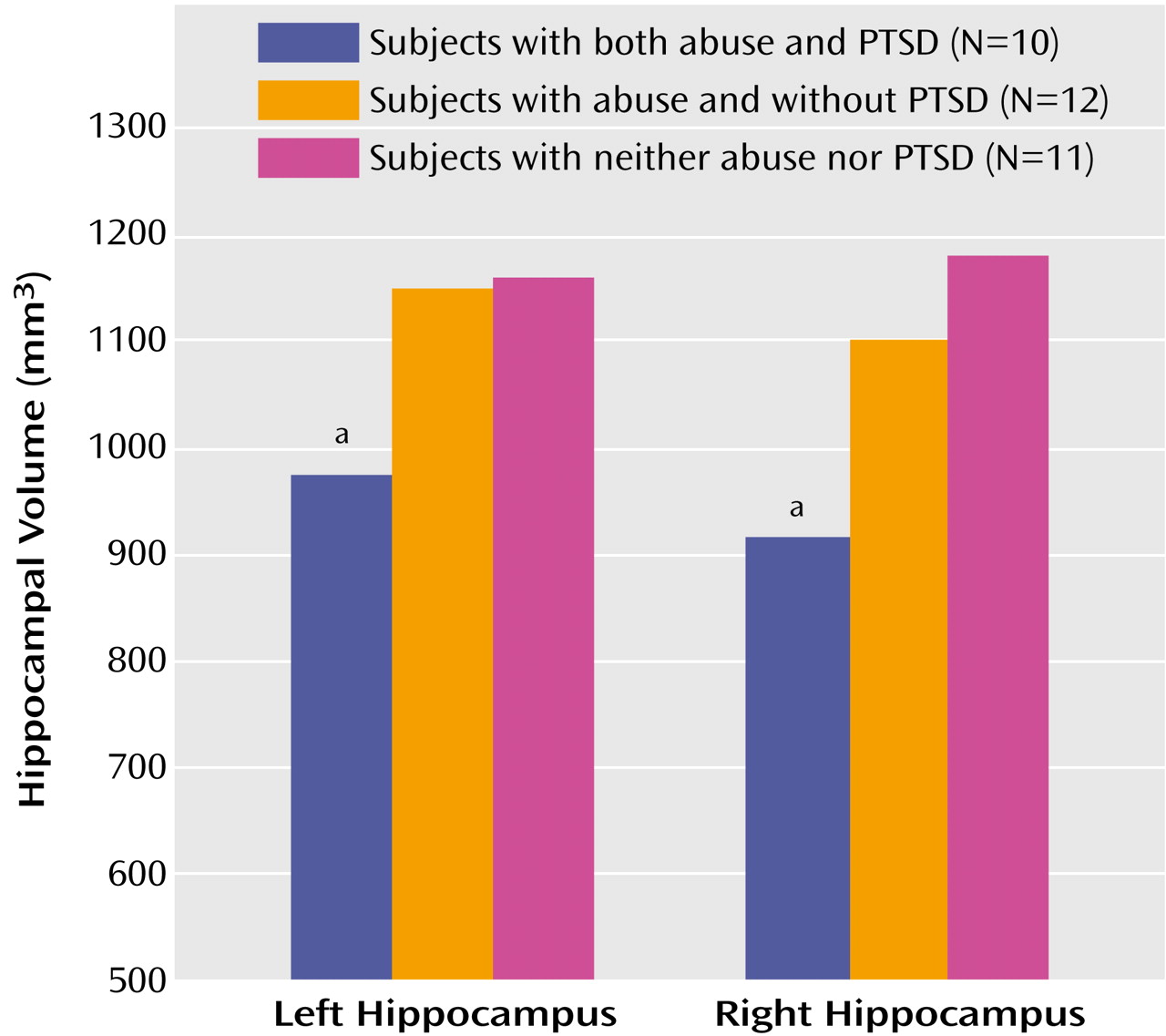
Thirty-three women with and without early childhood sexual abuse and PTSD participated in the study. Abused women had a history of severe childhood (before the age of 18 years) sexual abuse, including rape, genital fondling, or attempted rape. The subjects included women with childhood sexual abuse with PTSD (N=10), women with abuse without PTSD (N=12), and women without abuse or PTSD (N=11). The women in this study represented a different group from the subjects we have previously reported on in studies of hippocampal volume in PTSD
(30,
31). All women participated in the MRI component of the study. Only women with abuse, with or without PTSD, participated in the PET part of the study. All subjects were recruited through newspaper advertisements placed in local newspapers. The advertisements stated that women volunteers with a history of early life stress were requested for brain imaging studies. A second advertisement stated that healthy women volunteers were requested for brain imaging studies. The diagnosis of PTSD was established with the Structured Clinical Interview for DSM-IV (SCID)
(42) conducted by a master’s-level psychologist. Interrater reliability for the SCID at our site was high (intraclass correlation coefficient [ICC]=0.95). All subjects gave written informed consent for participation. Subjects were assessed with a history and physical examination, laboratory testing, and ECG to determine if they were free of medical illnesses that could affect brain structure or function. Individuals with serious medical illnesses were excluded. The subjects were not actively abusing substances or alcohol (within the past 6 months) and were free of all medications for at least 4 weeks before the study. The subjects’ medications were not discontinued for the purposes of participating in the study. Subjects with a serious medical or neurological illness, organic mental disorders, comorbid psychotic disorders, retained metal, or a history of head trauma, loss of consciousness, cerebral infectious disease, or dyslexia were excluded. All subjects were right-handed. No difference in age was found between the women with abuse and PTSD (mean=35 years, SD=6), the women with abuse without PTSD (mean=32 years, SD=8), and the women without abuse or PTSD (mean=38 years, SD=7). Likewise, the three groups did not differ in years of education (women with abuse and PTSD: mean=15 years, SD=2; women with abuse without PTSD: mean=17 years, SD=3; and women without abuse or PTSD: mean=15 years, SD=2).
History of childhood abuse was assessed with the Early Trauma Inventory by a master’s-level psychologist. The Early Trauma Inventory is a 56-item clinician-administered interview that assesses physical, emotional, and sexual abuse, as well as general traumatic events. The Early Trauma Inventory has been demonstrated to be reliable and valid in the assessment of childhood trauma
(43); at our site the interrater reliability was high (ICC=0.99). As noted previously, all women in the abuse groups had a childhood history of severe sexual abuse, defined as rape, attempted rape, or molestation before the 18th birthday. However, women with PTSD had still greater sexual abuse severity, as measured by the Early Trauma Inventory Sexual Abuse Severity Index (abused women with PTSD: mean=948, SD=711; abused women without PTSD: mean=71, SD=136). Subjects with a history of abuse also underwent assessment of PTSD symptoms with the Civilian Mississippi Scale, a reliable and valid measure of PTSD symptom severity that is administered as a self-report measure
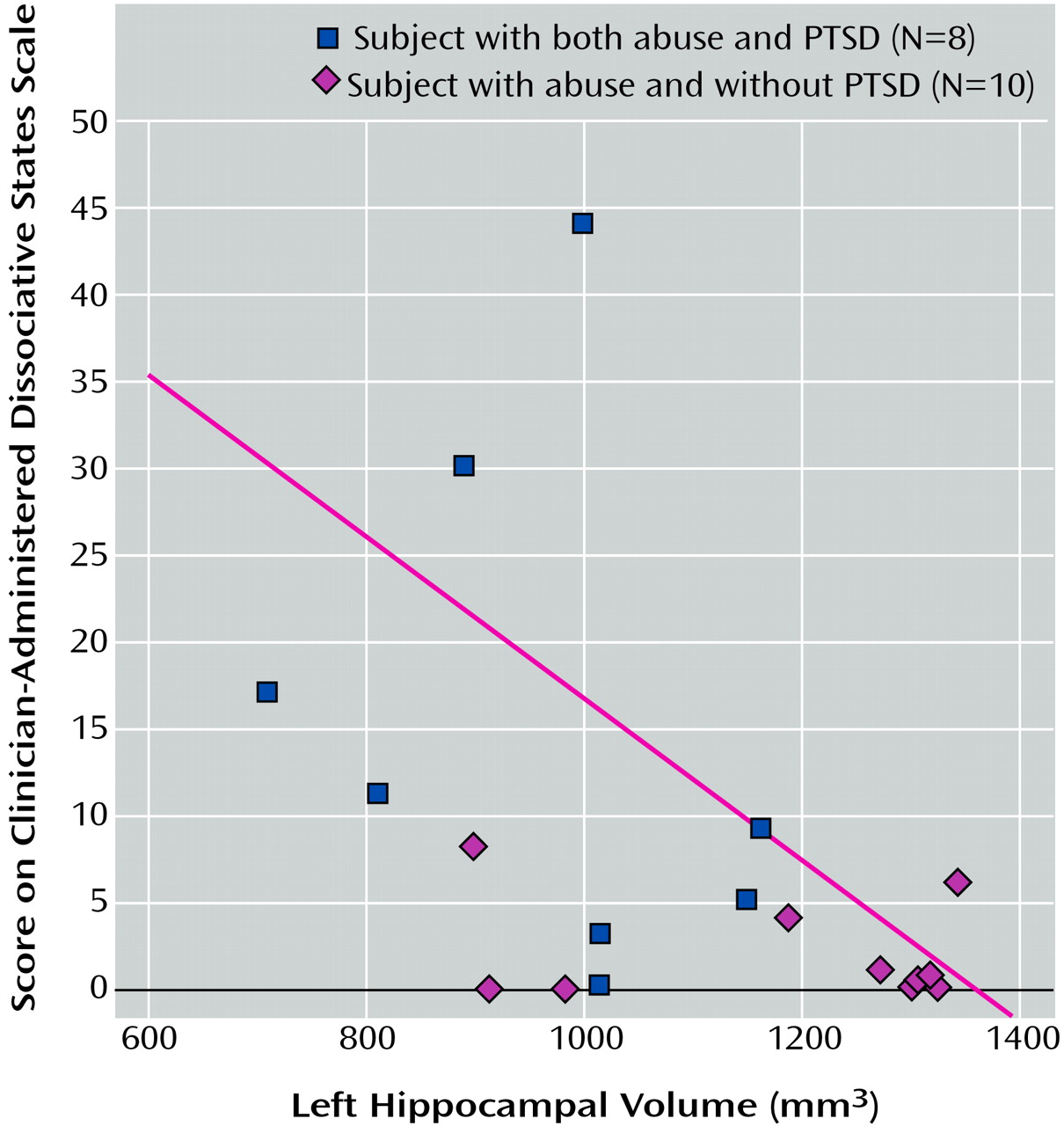
(44). The mean Civilian Mississippi Scale score was 126 (SD=26) for the abused women with PTSD and 75 (SD=6) for the abused women without PTSD. Current dissociative state in the abused women was assessed by a master’s-level psychologist with the Clinician-Administered Dissociative States Scale, a reliable and valid measure of the severity of dissociative states
(45); interrater reliability for the Clinician-Administered Dissociative States Scale at our site was high (ICC=0.92). The mean Clinician-Administered Dissociative States Scale scores were 11 (SD=10) for the abused women with PTSD and 2 (SD=3) for the abused women without PTSD.
On the basis of the SCID interview, eight (80%) of the 10 patients with PTSD fulfilled the criteria for a lifetime history of major depression and two (20%) fulfilled with criteria for current major depression. One patient (10%) met the criteria for a past history of dysthymia. Two (20%) fulfilled the criteria for a lifetime history of panic disorder with agoraphobia, two (20%) for current panic disorder with agoraphobia, and one (10%) for a lifetime history of panic disorder without agoraphobia. Four patients (40%) met the criteria for a past history of alcohol and/or substance abuse or dependence disorder; no patients had current disorders. The substance-related disorders included past alcohol dependence (30%), polysubstance dependence (10%), marijuana dependence (10%), and cocaine dependence (10%). Among the comparison group of sexually abused women without PTSD, three (25%) of 12 fulfilled the criteria for a lifetime history of major depression and none for current major depression on the basis of the SCID interview. One (8%) of 12 patients fulfilled the criteria for current panic disorder with agoraphobia. One (8%) of 12 fulfilled the criteria for lifetime obsessive-compulsive disorder, one (8%) for lifetime generalized anxiety disorder, and one (8%) for lifetime anorexia. One patient (8%) met the criteria for lifetime marijuana dependence, one (8%) for lifetime marijuana abuse, and one (8%) for lifetime cocaine dependence. None of the women without abuse or PTSD had a history of psychiatric disorder.
MRI Methods
All women underwent MRI imaging of the brain for measurement of hippocampal volume by using methods previously described
(30). Coronal images were obtained throughout the brain by using a General Electric Signa 1.5-T MR imaging device (Milwaukee) with spoiled gradient recall acquisition T
1-weighted images (TR=25, TE=5, NEX=2, 3-mm slice thickness without gaps). The images were transferred to a Sun Workstation (Sun Microsystems, Santa Clara, Calif.) for processing by using the ANALYZE program (Mayo Clinic, Rochester, N.Y.). Measurements of the mid-hippocampal body and whole brain volume were performed by using methods previously described
(30,
31). Briefly, the hippocampus was outlined in five slices (15 mm) between the superior colliculus and the bifurcation of the basilar artery. Measurements were performed by researchers who were blind to the subject’s name and diagnosis. Interrater reliability for this method, as measured with ICCs, was as follows: left hippocampus (ICC=0.93, p<0.05); right hippocampus (ICC=0.94, p<0.05).
PET Methods
In the PET study, the abused women with PTSD were compared with those without PTSD by using PET methods previously described
(46). Each subject underwent four PET scans on a single day. The subject was placed in the scanner with her head in a holder to minimize motion and was positioned with the canthomeatal line parallel to an external laser light. An intravenous line was inserted for administration of [
15O]H
2O. After the subject’s head was positioned within the camera gantry, a transmission scan of the head was obtained by using an external
67Ga/
68Ge rod source, to correct emission data for attenuation due to overlying bone and soft tissue.
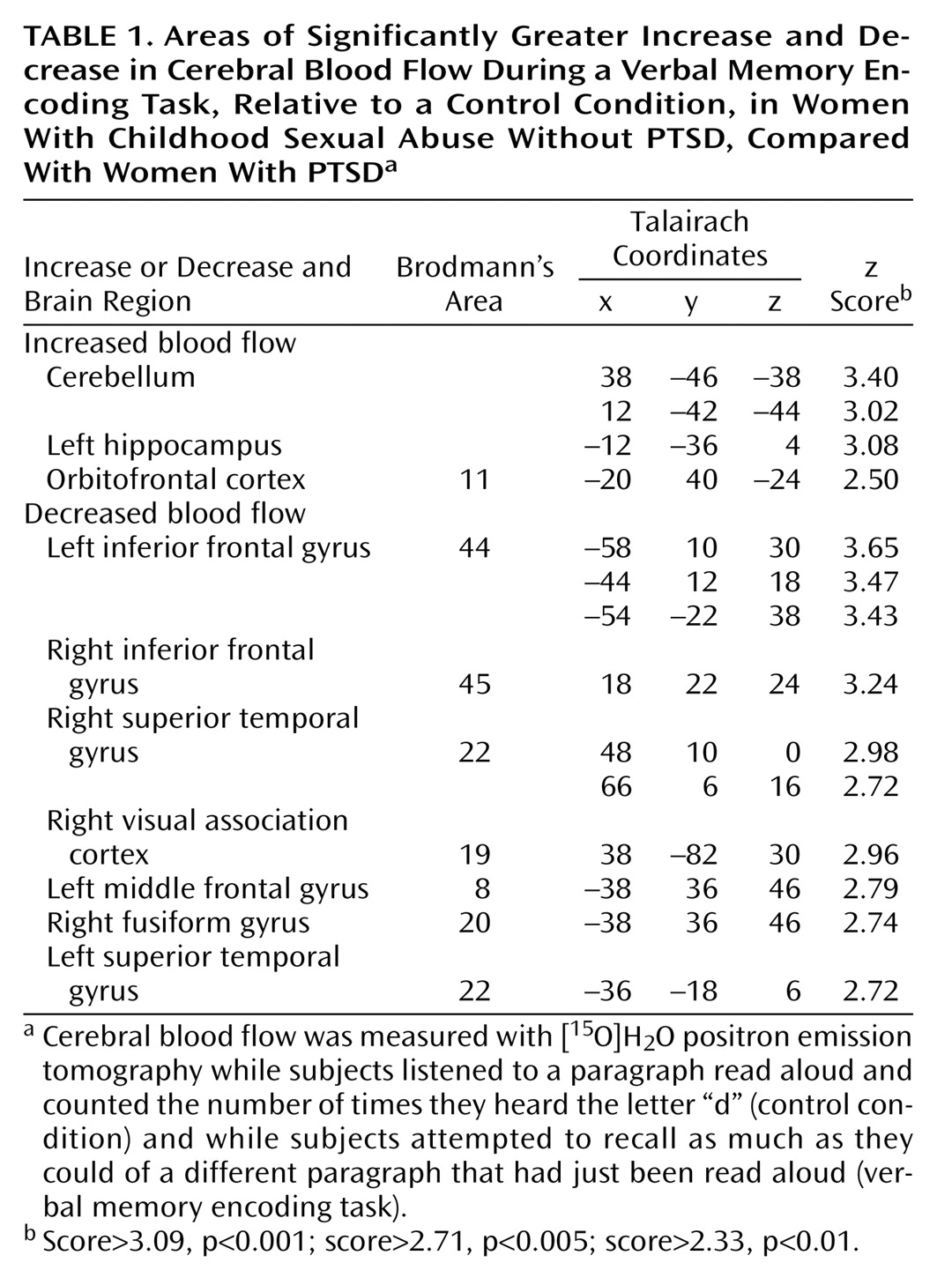
Subjects then underwent scanning during verbal declarative memory and control tasks. All tasks involved listening to a paragraph that was read aloud in a normal tone of voice over a 1-minute period. Encoding of paragraphs was selected as the task for assessment of neural correlates of verbal declarative memory function because prior studies have shown that PTSD patients have deficits on this task
(24,
25). Subjects first underwent two scans while listening to two different paragraphs during which time they were instructed to count the number of times they heard the letter “d.” Then subjects underwent two scans during which they listened to one of two different paragraphs preceded by instructions to form an image in their mind and try and remember as much of the paragraph as they could. Five minutes later, subjects were asked to engage in free recall of the paragraph. Scores consisted of the number of elements of the paragraph correctly recalled. A fixed order (the control condition followed by the memory-encoding condition) was followed to minimize memory encoding during the control condition. According to the logic of the study design, differences in brain blood flow between the memory-encoding and the control conditions would be secondary to the specific effects of verbal declarative memory encoding, while keeping other factors equal, including attention, auditory perception, and comprehension of a coherent verbal narrative.
Ten seconds before administration of [15O]H2O, subjects received instructions related to the paragraph to be read. The reader then began the reading of the paragraph, which lasted a total of 60 seconds. At the same time the reader began reading, the subject received a bolus injection of 30 mCi of [15O]H2O, followed 10 seconds later by a PET scan acquisition that was 80 seconds in length. The onset of the PET scan acquisition was timed to correspond to the point of maximum increase in uptake of tracer into the brain. With the bolus injection method of [15O]H2O (which has a half-life of 110 seconds), the tracer peaks at 10 seconds, with 90% of counts obtained in the first 60 seconds after the peak, which was the time during which the paragraph was read. PET imaging was performed on a Posicam PET camera (Positron Corp., Houston) (in-plane resolution after filtering=6 mm full width at half maximum).
Images were reconstructed and analyzed on a SunSparc Workstation (Sun Microsystems, Santa Clara, Calif.) by using statistical parametric mapping (SPM 96) (Wellcome Department of Cognitive Neuroscience, Institute of Neurology, University College London). Images for each patient set were realigned to the first scan of the study session. The mean concentration of radioactivity in each scan was obtained as an area-weighted sum of the concentration for each slice and adjusted to a nominal value of 50 ml/min per 100 g. The data underwent transformation into a common anatomical space and were smoothed with a three-dimensional Gaussian filter to 16 mm full width at half maximum. Regional blood flow with global blood flow as a covariate was compared between the control and active conditions in sexually abused women with and without PTSD. The interaction between group (PTSD versus non-PTSD) and condition (control versus memory encoding) was also examined. Statistical analyses yielded image data sets in which the values assigned to individual voxels correspond to the t statistic
(47). Statistical images were displayed with values of z score units. A threshold z score of 3.09 (p<0.001) was used to examine areas of activation within the hypothesized region (hippocampus). The threshold of the z score corresponds to a p value of <0.001 for a one-tailed t test. Since the current study was a replication of a prior study in combat veterans with PTSD, the direction of change in blood flow was hypothesized a priori, which justified the use of a one-tailed test. SPM 96 employs a fixed-effects analysis that may limit the ability to generalize from the findings for the study group. Location of areas of activation were identified as the distance from the anterior commissure in millimeters, with x, y, and z coordinates, using a standard stereotaxic atlas
(48).
Data Analysis
Repeated-measures analysis of variance with side (left and right hippocampus) as the repeated measure was used to compare hippocampal volume between groups. Linear regression was used to compare the relationship of left and right hippocampal volume with left hippocampal blood flow during the memory task and variables hypothesized to be related to these parameters, including PTSD symptom level as measured with the Civilian Mississippi Scale and dissociative symptom level as measured with the Clinician-Administered Dissociative States Scale. Analysis of covariance was used to compare hippocampal volumes between groups, with adjustment for whole brain size.
Discussion
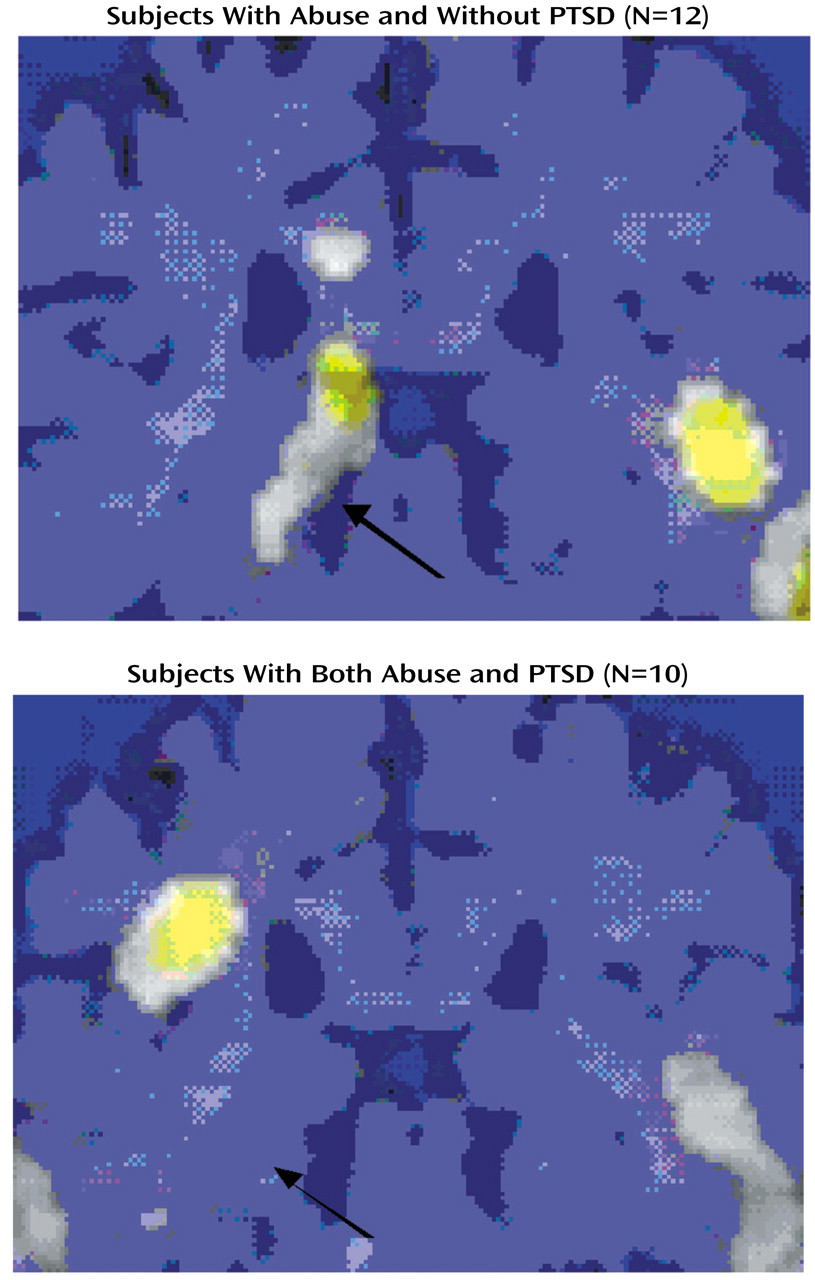
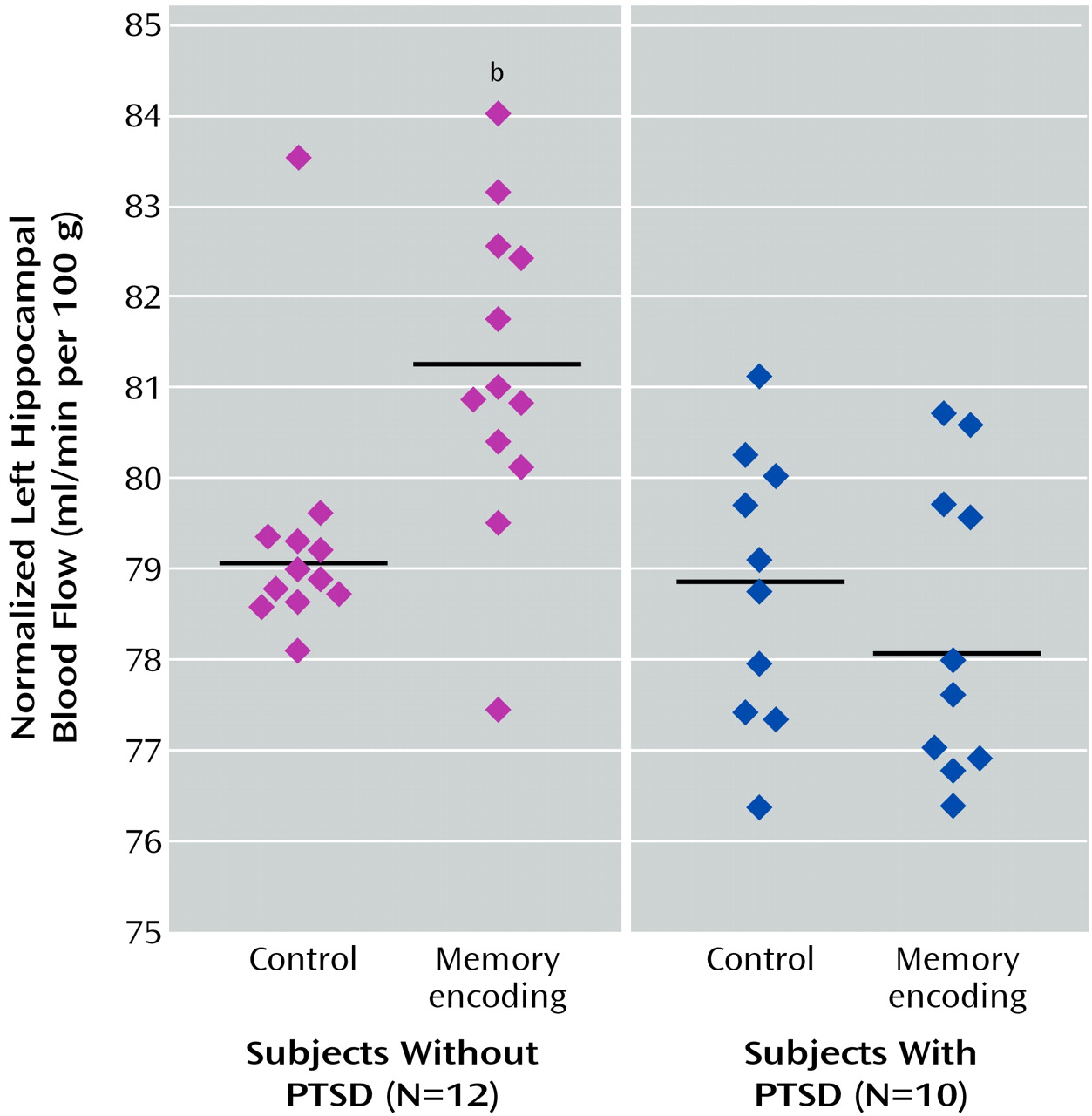
The findings of the current study are consistent with deficits in both hippocampal structure and function in PTSD related to early childhood sexual abuse in women. In this study, abused women with PTSD had a 16% lower mean hippocampal volume than abused women without PTSD and a 19% lower mean hippocampal volume than women without abuse or PTSD. These differences were significant after adjustment for differences in whole brain volume. The women with PTSD also showed a failure of left hippocampal activation during a verbal memory task (paragraph encoding) that was significant after adjustment for hippocampal atrophy. Measures of symptoms of dissociation were correlated with smaller left hippocampal volume, and measures of PTSD symptoms were correlated with smaller right hippocampal volume.
These findings are similar to those of prior studies of patients with PTSD. The current study represents the third independent replication of smaller hippocampal volume in PTSD from our own group. These findings also provide evidence that smaller hippocampal volume in patients is not seen in all individuals with a history of childhood abuse but is seen only in individuals who have both a history of abuse and the diagnosis of PTSD. This finding corroborates a previous study in combat veterans
(33) and suggests a correlation between changes in the brain and PTSD symptoms. To our knowledge, this is the first report showing failure of hippocampal activation during a memory task (during the encoding of a paragraph) in PTSD, which adds corroborative evidence for deficits in the hippocampus in PTSD. The findings provide a structural and functional neuroanatomical correlate for the deficits in neuropsychological testing of declarative memory found in patients with PTSD and provide support for the hypothesis that stress is associated with hippocampal damage or dysfunction.
The deficits in hippocampal structure and function appear to be specific to the diagnosis of PTSD and not a nonspecific outcome of exposure to childhood abuse. A number of studies have shown that PTSD is associated with long-term changes in brain structures and systems that mediate memory and the stress response
(23,
49). However, only 15% of individuals exposed to a traumatic stressor (defined as a threat to the life of self or significant other, accompanied by intense fear, horror, or distress) will develop chronic symptoms of PTSD. A critical question in the field is why, among individuals exposed to a given level of stressor, some develop chronic PTSD symptoms and others do not. It is possible that abused women who develop stress-induced neurological deficits, including hippocampal deficits, develop PTSD, while abused women who do not develop hippocampal deficits do not develop PTSD. Another possibility is that, in abused women who develop PTSD, the stress of the disorder, including repeated traumatic reminders with activation of stress responses, leads to hippocampal damage and/or inhibition of neurogenesis
(15,
16). A third possibility is that individuals with baseline hippocampal deficits have a genetic vulnerability to develop PTSD after being abused
(49). The findings of the current study are consistent with the idea that abuse per se in the absence of PTSD does not lead to deficits in hippocampal structure or function. Additional research is needed to improve our understanding of why some individuals develop PTSD in response to a stressor and others do not.
Several aspects of this study deserve comment. We did not find a significant difference in memory performance on the paragraph recall component of the study between women with and without PTSD, which contradicts prior studies of verbal declarative memory function in PTSD
(24–
29). However, prior studies that focused on neuropsychological testing alone had larger numbers of subjects. PTSD patients in the current study did show a pattern of poorer performance (8% difference) that might be statistically significant in a larger group of subjects.
We performed several correlations of dissociation (Clinician-Administered Dissociative States Scale), PTSD symptoms (Mississippi scale), and abuse severity (Early Trauma Inventory) with left and right hippocampal volume. These analyses showed a correlation between smaller left hippocampal volume and dissociation (Clinician-Administered Dissociative States Scale) and smaller right hippocampal volume and PTSD (Mississippi scale). Because of the multiple comparisons involved in these correlations, the findings should be considered preliminary. However, the finding of a correlation between smaller left hippocampal volume and dissociation replicates a finding of a prior study in abuse-related PTSD
(32).
The PET study involving measurement of hippocampal activation with memory tasks did not include a comparison group of women without abuse or psychiatric disorder. Therefore, we do not have information about the performance of this task in normal women. However, we subsequently studied brain activation using this same task in normal subjects (men and women) and demonstrated hippocampal activation (data not shown); this result suggests the validity of this task for measuring hippocampal activation in normal individuals (unpublished 2002 data of J.D. Bremner, et al.).
The women with abuse-related PTSD in the current study showed the typical dilemmas of multiple comorbidities of past history of alcohol or substance abuse/dependence and depression. Although we are confident that current or even recent alcohol or substance abuse/dependence did not confound our results, it is possible that past histories could be a confounding factor. Other studies based on national samples have shown that women with PTSD had a 28% rate of a past history of alcohol abuse/dependence, compared with 14% in women without PTSD
(3). Women with PTSD also had a 46% lifetime rate of comorbid depression, compared with 10% for women without PTSD. In addition, women with PTSD had higher rates of all anxiety disorders, including panic disorder. We did not exclude women with comorbid affective and anxiety disorders or past alcohol abuse/dependence, as we felt that these criteria would result in selection of subjects who were not representative of women with abuse-related PTSD at large. We did exclude women with a history of schizophrenia, eating disorders, or bipolar disorder and women with current alcohol/substance use disorders. Bremner
(23) has argued that these commonly comorbid disorders should be viewed as representing a group of “trauma-spectrum” disorders that have their basis in a stress-mediated effect on the brain. Friedman and Yehuda
(50) have argued against exclusion of patients with comorbid depression from PTSD studies, based on the absence of biological findings to support differences in PTSD patients with and without histories of comorbid depression and doubts about the truly distinct nature of depression as a separate entity in PTSD patients when this disorder follows the development of PTSD.
The current study used a declarative memory task (paragraph recall) to study hippocampal activation. However, despite the evidence from lesion studies that the hippocampus plays an important role in new learning and memory
(6), prior PET studies have not in fact consistently found activation in the hippocampus during memory tasks
(51–
57). Some researchers have argued that the hippocampus is activated only during successful retrieval, during learning of novel material, or during encoding (but not retrieval) of memories
(58). To our knowledge, the current study is the first study to use paragraph encoding as a probe of hippocampal function. Paragraph encoding involves a complex synthesis of speech comprehension, assessment of lingual structure and syntax, comparison with prior experiences, and visual imagery. The complex role of paragraph encoding is consistent with the integrative role in memory formation hypothesized for the hippocampus
(5). Memory encoding (as opposed to retrieval) was selected, as most prior PET studies have found more robust hippocampal activations with encoding tasks. For these reasons, and because we found robust deficits in paragraph recall in patients with PTSD, we used encoding of a paragraph as the probe of hippocampal function.
This study adds to a growing literature indicating hippocampal dysfunction in PTSD. In our own research we have used a multifaceted approach to study brain areas, including structural imaging, specific cognitive probes of function in individual brain regions (such as memory encoding as a probe of hippocampal function), and stimulus of specific PTSD symptoms (e.g., stimulation of traumatic recall with scripts of childhood abuse). These studies have provided convergent evidence that common brain areas, including the hippocampus, mediate both the cognitive and the symptomatic disturbances in PTSD. These studies and others have implicated in addition to the hippocampus an interconnected network of brain areas such as the medial prefrontal cortex, including the anterior cingulate proper (Brodmann’s area 32) and other areas of the anterior cingulate (subgenual area [Brodmann’s area 24] and the subcallosal area [Brodmann’s area 25])
(46,
59,
60); the inferior frontal gyrus; the inferior and middle temporal gyri; the posterior cingulate; and the visual association cortex
(61–
68). Given the known role of the hippocampus in mediating emotional processing of complex visual stimuli
(69,
70), it is not surprising that the same region is involved in both cognitive and symptomatic processes in PTSD.