Cognitive impairment is a common complication after stroke, with a prevalence varying from 13.6% to 35.2%
(1–
7). The impairment may range from a minimal deficit in memory
(8) to a transient disturbance of orientation
(9) to an irreversible dementia
(3,
5,
10). Figures about the incidence of cognitive impairment after stroke have varied on the basis of the population studied, criteria used to determine cognitive impairment or dementia, type of neuropsychological testing used, time after stroke at which cognitive status was assessed, and whether the patients were depressed.
In this investigation, we studied cognitive changes over 2 years in a group of depressed stroke patients with initial cognitive impairment who were treated for depression in a double-blind study. We hypothesized that for patients with early and sustained remission of depression, cognition would rapidly improve with depression and remain improved over the 2 years of follow-up.
Discussion
This study demonstrated a rapid improvement in cognitive function in patients with poststroke depression who showed an early and sustained remission of their depression. In addition, the improvement among patients with remitted depression was maintained over 2 years. To our knowledge, this is the first time that treatment or remission of poststroke depression has been shown to produce a cognitive improvement that lasts more than 2 years if no subsequent illness occurs.
Before the findings and their implications are discussed further, the limitations in this study need to be acknowledged. First, the MMSE is a relatively brief examination that is language dominated. A more detailed neuropsychological battery would have allowed a fuller examination of how the spectrum of cognitive functions and their longitudinal progression was affected by depression. Another limitation is the attrition of patients, mostly within the first 6 months. The patients in the study, who were regularly followed up through 2 years, may have been highly compliant and thus may not be representative of all stroke patients. A third limitation is that administering the MMSE every 3 months may have led to a practice effect. However, the leveling off of the MMSE score in the depressed patients and the lack of any improvement in the nondepressed patients suggest that this is not so. A final limitation, which is inherent not only in this study but also in most studies on poststroke cognitive impairment, is that the prestroke cognitive status of the subjects was not known and quantified. Most studies have identified and enrolled subjects after the onset of stroke and relied on retrospective approximation of the prestroke cognitive status from interviews with the subjects or close relatives. Without a prestroke neuropsychological assessment, it is difficult to ascertain how and to what extent cognitive functions were affected by stroke. Because of the similarities in age and education, however, overall group differences in premorbid cognitive function would not be expected.
As far as we are aware, one of the few, perhaps the only, study that was able to compare pre- and poststroke cognitive assessments is the Framingham study
(29). In this prospective observational study, participants were followed up biennially, and MMSEs were carried out. For participants who subsequently developed stroke, another MMSE was carried out 6 months after their illness. Participants in this study were generally older; the mean age for men was 76.0 years (SD=0.7), and for women it was 81.0 years (SD=0.8). The stroke patients had a prestroke mean MMSE score of 27.28 (SD=0.34) and a poststroke score of 23.57 (SD=0.92), while nonstroke control subjects had mean scores of 28.08 (SD=0.21) and 28.31 (SD=0.25), respectively. The change in MMSE score differed significantly between the stroke patients and control subjects. After the stroke, 31.1% of the patients had an abnormal MMSE score (defined as lower than 24). The importance of the Framingham study is that it demonstrates that about 70% of the stroke patients, although not demented or having an abnormal MMSE score after the stroke, nonetheless suffered some degree of cognitive decline after the stroke, which was quantified as 3.71 points of mean decline on the MMSE.
On the basis of the Framingham data, the initial mean MMSE score of 26.3 (SD=3.1) for the nondepressed patients in our study almost certainly represents a decline from their prestroke cognitive ability. This is further corroborated by comparison of their MMSE scores with population-based norms for age and educational level
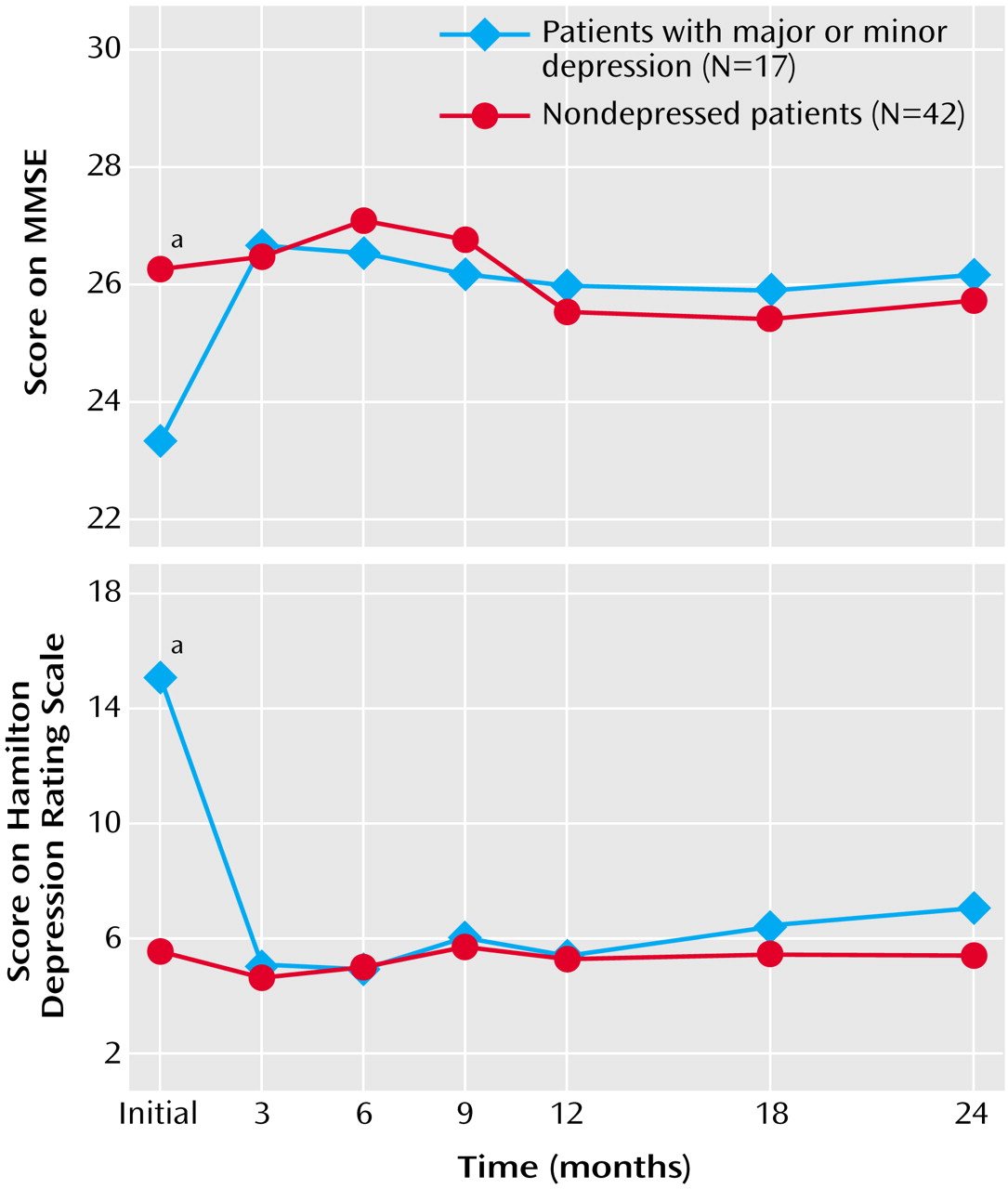
(30); the mean score for people ages 65–69 years with 9–12 years of education is 28 (SD=1.4). The depressed patients had an initial mean MMSE score of 23.3 (SD=4.2), which was 3.0 points lower than that for the nondepressed patients. After remission of the depression, the MMSE scores for the depressed and nondepressed patients at 6 months were almost identical (mean=26.5, SD=3.1, versus mean=27.1, SD=3.1), but they were still lower than the population-based mean norm of 28 (SD=1.4) for people ages 65–69 years who have 9–12 years of education
(30). Thus, the effects of brain infarction and depression on cognitive function appear to be additive.
For the patients in this study, the degree of cognitive impairment due to depression was 3.3 points on the MMSE (difference between the initial score of 23.3 and the mean score of 26.6 after remission of depression). During the longitudinal follow-up, the nondepressed patients showed no significant change in MMSE scores over 2 years. This finding suggests that the cognitive deterioration due to ischemic brain injury does not improve between 1 month and 24 months poststroke.
The determinants of cognitive impairment due to ischemic brain damage have been described in several studies. The Framingham study showed a correlation between poststroke cognitive decline and large left-sided strokes
(29). Tatemichi et al.
(7), by examining a broad range of neuropsychological deficits independently of a diagnosis of dementia, found cognitive impairment (described as failure on any four items in a battery of tests) in 35.2% of stroke patients and an association of cognitive impairment with major cortical syndromes and infarctions in the territories of the left anterior and posterior cerebral arteries. Moderately severe cognitive impairment, diminished alertness in the acute stroke stage, temporal lobe infarcts, multiple infarcts, and pronounced ventricular enlargement were found by Schmidt et al.
(31) to result in high risk for long-term intellectual dysfunction. Our group
(32) has found that long-term cognitive impairment may be associated with subcortical caudate strokes. The determinants of poststroke dementia have been found by Censori et al.
(2) to be diabetes mellitus, atrial fibrillation, aphasia, large middle cerebral artery infarcts, and frontal lobe lesions. Desmond et al.
(3) found the determinants to include 1) stroke characteristics, such as the severity and location of the stroke, especially with more severe left hemispheric infarcts in the territories of the anterior and posterior cerebral arteries, 2) vascular risk factors of diabetes mellitus and previous stroke, and 3) host characteristics, such as greater age, fewer years of education, and nonwhite race/ethnicity.
Poststroke cognitive impairment related to major depression has been studied by our group for several years
(17,
18,
26,
28,
33,
34). In an earlier study
(35), we compared patients with major depression and nondepressed patients matched for lesion size and location and found a difference of 5.8 points in MMSE score between depressed patients (mean=16.6, SD=7.8) and nondepressed patients (mean=22.4, SD=6.6) (p=0.02). In addition, we found that depression was associated with cognitive impairment only for the first year after the stroke and that the effect of depression on cognitive function was strongest during the acute poststroke period
(34).
We have also demonstrated
(17) improved cognition among patients whose depression remitted after treatment with nortriptyline or placebo. This suggested that the improvement in cognitive function was due to the mechanism of remission of major depression and was not due to a direct effect of nortriptyline on cognition. This conclusion is consistent with our finding in the present study that 10 nondepressed patients given nortriptyline showed no significant improvement in MMSE score.
Assessment of the use of antidepressant medication after the first 12 weeks of the treatment trial, when patients were returned to the care of their primary care physicians, revealed no difference between depressed and nondepressed patients in the frequency or duration of antidepressant use. This suggested that the sustained improvement in the cognitive function of the depressed patients was not due to prolonged use of antidepressants but was associated with sustained remission of depression.
Some studies on elderly populations with depression or stroke have shown long-term cognitive deterioration. Alexopoulos et al.
(36,
37), who followed up on elderly patients (average age, 73 years) with reversible depressive dementia without stroke, found that 43% developed an irreversible dementia about 33 months later. On the basis of this finding, the authors proposed that patients who have late-onset depression with reversible dementia may include some who have a preexisting early-stage dementia
(36,
37). Moroney et al.
(38) followed up on nondemented stroke patients (average age, 70 years) for 53 months and found that hypoxic-ischemic events after the stroke, such as seizures, cardiac arrhythmias, and pneumonia, resulted in a higher risk for subsequent dementia.
The absence of deterioration of cognitive function in our patients over 2 years in this study may be due to the fact that they were younger than patients in other studies and that the follow-up was shorter. Further cognitive deterioration after an initial stroke may be related to age, duration since stroke, or subsequent reinjury to the central nervous system, such as another stroke, hypoxic-ischemic events, or the onset of neurodegenerative disorders.
In summary, poststroke cognitive dysfunction associated with depression, once improved, is likely to remain stable over the next 2 years, unless there is subsequent reinjury to the central nervous system. Hence, there is a need for early detection and treatment of poststroke depression in order to maximize cognitive function.