Karl Ludwig Kahlbaum’s hallmark monograph,
Die Katatonie oder das Spannungsirresein (1), translated into English in 1973
(2), characterized catatonia as a specific disturbance in motor functioning that represents a phase in a progressive illness that includes stages of mania, depression, and psychosis and that typically ends in dementia. Although many authors confirmed Kahlbaum’s views, Emil Kraepelin, who incorporated the features of catatonia into his concept of dementia praecox
(3), exerted a persistent influence on the classification of catatonia. Bleuler followed Kraepelin’s conceptual model for catatonia
(4), and, although numerous authors argued against this view, clinicians throughout most of the 20th century considered catatonia as an exclusive subtype of schizophrenia
(5,
6). The idea that catatonia is tied to schizophrenia was codified in all DSM and ICD editions.
A change in emphasis was heralded in U.S. writings in the mid-1970s. Morrison
(7–
10) reawakened the profession to the association between catatonia and mood disorders. Abrams and Taylor
(11–
15) reestablished that most catatonic patients have a mood disorder, particularly mania, and that 20% of patients with mania exhibit catatonic features. Concurrently, Gelenberg
(16) documented the association of catatonia with neurologic and general medical conditions and emphasized that catatonia should be considered a syndrome, not a disease. Briefly summarizing that literature, Fink and Taylor
(17) argued that catatonia should not be linked exclusively to schizophrenia and that classification systems could better reflect the evidence that catatonia occurs in many illnesses. This effort helped further changes in the concept of catatonia that are reflected in DSM-IV, which maintained the link between catatonia and schizophrenia but also added catatonia as a specifier in mood disorders and as a syndrome resulting from a general medical disorder.
Efforts to further define the syndrome have been described in the European and U.S. literature. Following the writings of Wernicke, Kleist, and Leonhard, some German psychopathologists have characterized catatonia into distinct subgroups based on symptom clusters, the presence of a periodic course, and specific family illness patterns
(18–
23). A similar unique classification was offered by Gjessing
(24) in his studies of recurrent forms of the illness that he labeled “periodic catatonia”. American psychopathologists, viewing catatonia as a syndrome present in a variety of psychiatric disorders, took an opposite approach. They considered the merits of merging similar conditions such as the neuroleptic malignant syndrome and the toxic serotonin syndrome as medication-related variants of malignant catatonia. Thus, rather than three separate syndromes requiring distinct treatment paradigms, they recognized one
(25–
30). These and other efforts to define catatonia
(13) continue to challenge psychopathologists.
In this context, we examined the validity of catatonia as a distinct syndrome by reviewing the literature on catatonia. We sought this literature in major indices (Index Medicus, MEDLINE, PsycINFO), library collections (National Library of Medicine, New York Academy of Medicine, British Library), and the libraries of several medical schools. An extensive bibliography is cited in a review of the syndrome
(5). In our effort to determine the merits of a separate diagnostic class for catatonia, we followed the initial steps suggested by Robins and Guze
(31) for establishing the validity of a psychiatric illness: determining the reliability of identification, distinguishing the condition from other syndromes, and identifying a characteristic course or pattern of treatment responsiveness. We also applied the guidelines of Blashfield et al.
(32) for inclusion and exclusion of diagnoses in a classification system.
Catatonia Is Common
The phenomena that define catatonia are the motor abnormalities that occur in association with changes in thought, mood, and vigilance. The most common signs are mutism, posturing, negativism, staring, rigidity, and echophenomena. These signs occur in two principal forms, a retarded-stuporous variety and an excited-delirious variety. Kahlbaum described 17 signs, but other authors have extended this list, some identifying 40 or more phenomena
(5,
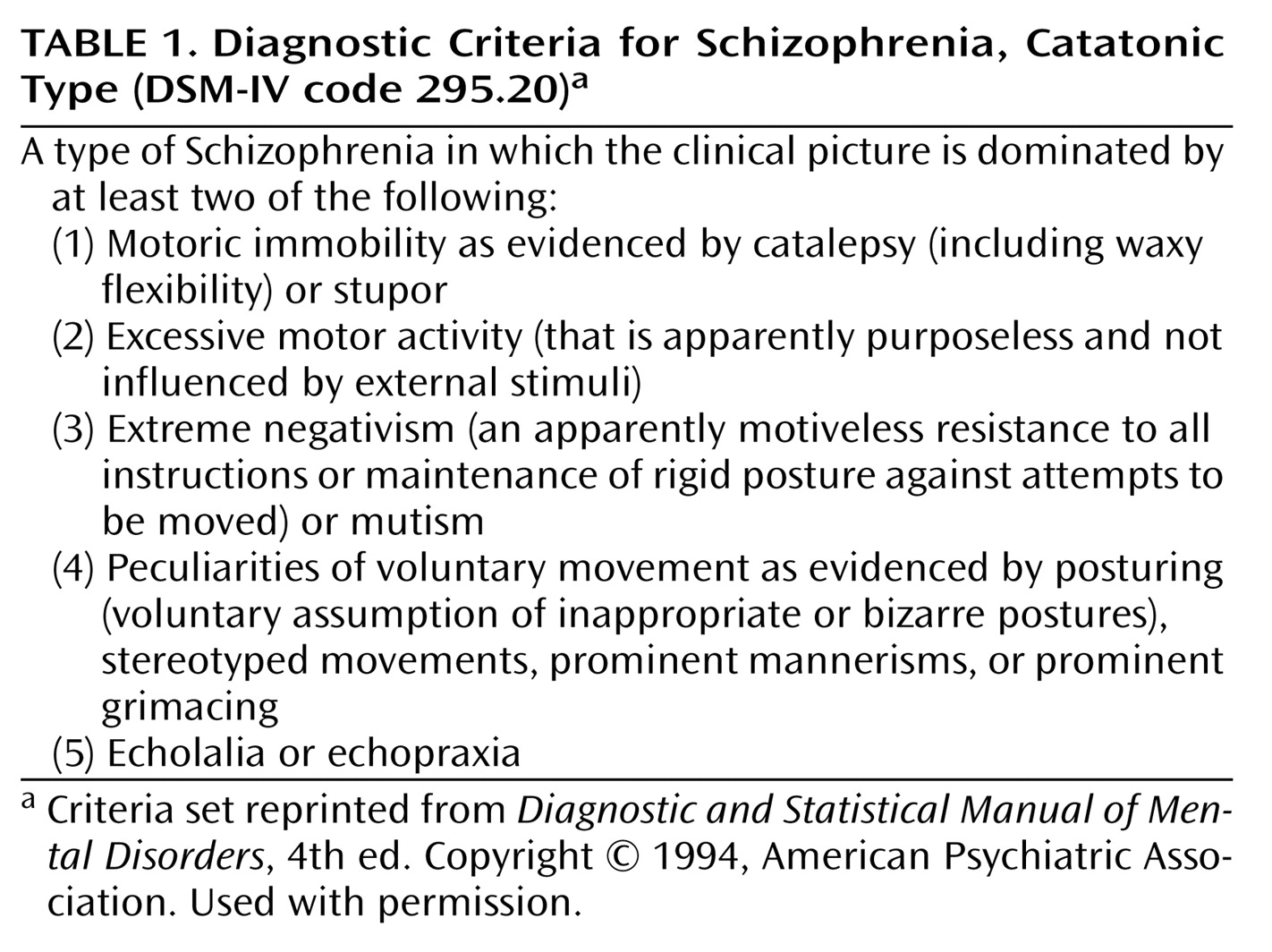
6). The presence of two prominent signs is sufficient for the patient to meet the current DSM criteria (
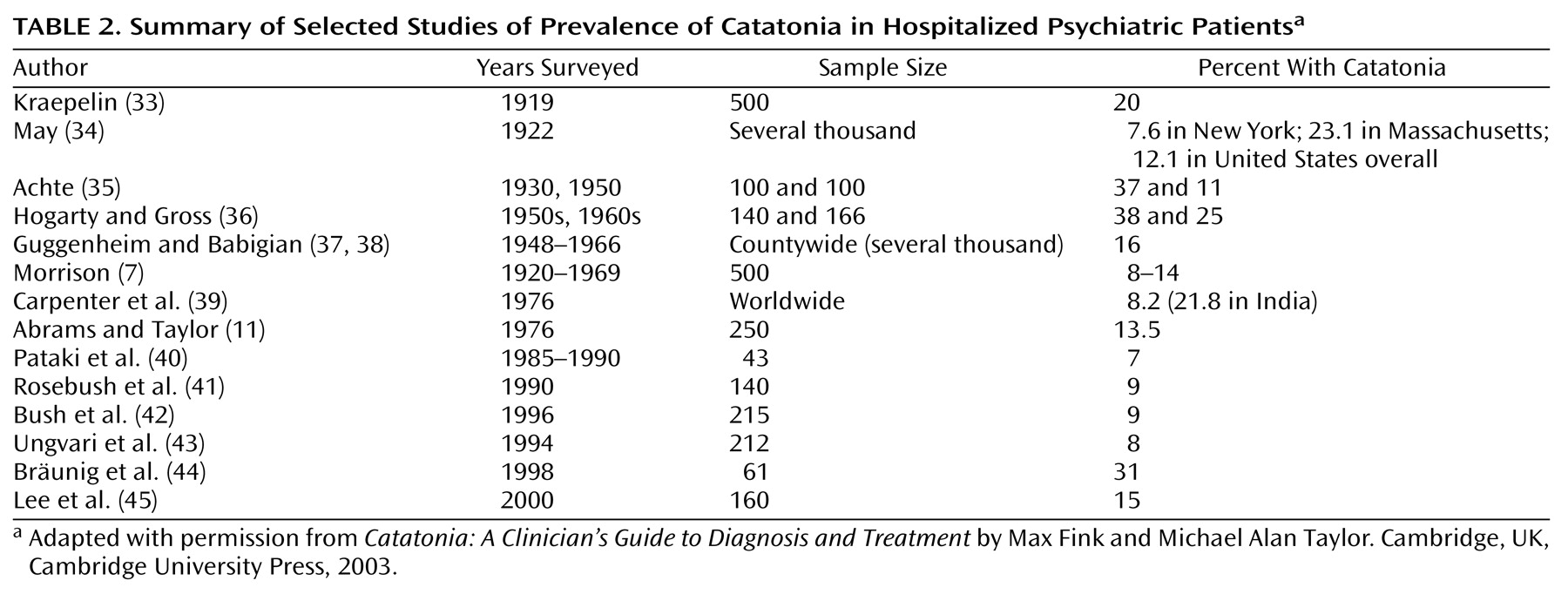
Table 1). Although no duration criterion is specified, most investigators who have used catatonia rating scales accept several to 24 hours’ duration as necessary. Using these or similar criteria, numerous surveys have found the prevalence of catatonia among psychiatric patients to range from 7.6% to 38% (
Table 2)
(7,
11,
33–45).
Using data from HCIA, Inc., we looked at discharge psychiatric diagnoses from a randomly selected one-third of nonfederal U.S. hospitals from October 1996 to September 1997
(46). Diagnoses were coded by using ICD-9-CM criteria. Among the 6,022 hospitals, 160,135 patients had a mood disorder diagnosis. Of those patients, 42,581 were classified as having a bipolar mood disorder. In addition, 68,298 patients were classified as having schizophrenia (catatonic subtyping not noted) and 17,816 as having schizoaffective disorder, a designation usually given to psychotic patients in a manic or mixed manic state who have become more chronically ill. Of other diagnoses associated with catatonia, 5,982 patients were listed as having a drug withdrawal state and 2,748 as having an extrapyramidal disorder. Neuroleptic malignant syndrome was not listed among the discharge diagnoses. Using a 10% overall prevalence of catatonia, as suggested by the studies of prevalence, and a 20% prevalence of catatonia for patients with bipolar mood disorder, we estimated that 29,875 acute psychiatric inpatients probably exhibited catatonia during that period. These data from a sample of one-third of U.S. hospitals suggest that a total of approximately 90,000 patients exhibit signs of catatonia annually. This figure is three times the estimate of 30,000 for the number of suicides annually in the United States
(47).
The commonly recognized diagnostic features of catatonia include immobility and mutism, but patients with catatonia notably display many other signs and may not be mute or immobile
(2,
4,
5,
7,
11,
15,
33,
48,
49). Recognition of the diverse signs of catatonia is central to recognizing the disorder. Some classic features (e.g., automatic obedience, gegenhalten, ambitendency) are not usually assessed even when catatonia is suspected. Also, the spectrum features of catatonia (e.g., whispered or robotic speech, unexplained foreign accents, tiptoe walking or hopping, rituals, and mannerisms) are not usually identified as signs of catatonia, and their diagnostic implications may remain unrecognized
(5,
49).
Catatonia has also been described in children and adolescents. Dhossche and Bouman
(50,
51) found 30 reports of catatonia in adolescents and children published between 1966 and 1996 and added another description. One-third of the subjects had a diagnosis of a neurologic or a general medical disease, six had a mood disorder, three had schizophrenia, and 11 had atypical psychoses. Cohen et al.
(52) described 42 children with catatonia, including 20 with a mood disorder and seven with schizophrenia. Wing and Shah
(53) used a catatonia rating scale to assess 506 consecutive referrals to a child communications and social disorders program. They reported that 30 (6%) of the adolescent patients met the criteria for catatonia. In another study, a diagnosis of catatonia was made for half of a group of adolescents receiving ECT
(54).
Identification as a Syndrome
Catatonia rating scales are a recent development, although lists of motor signs for identifying the syndrome were published as early as 1924
(6,
55,
56). Almost all the instruments begin with Kahlbaum’s original 17 features
(1,
2). Other scale developers have included 21 to 40 signs
(5,
57–61).
Three recently published rating scales reported good interrater reliability individually and across instruments. For example, four raters using a catatonia rating scale developed by Bräunig et al.
(58) to examine 71 catatonic patients reported pairwise correlations of 0.96 to 0.97. For the scale developed by Northoff et al.
(59), the interrater reliability for individual items was 0.9. For the Stony Brook scale developed by Bush et al.
(57), pairwise interrater reliability was also 0.9. Catatonic features can be reliably assessed whether they are the continuous signs of catalepsy and posturing or the intermittent features of ambitendency and echophenomena.
Several factor analytic and one cluster analytic study have delineated patterns among the many catatonic features, indicating that a syndrome exists
(13,
60–65). Despite differences in patient samples and a lack of uniformity in methods of assessment, two patterns—one consisting of catalepsy, posturing, mutism, and negativism and a second consisting of echophenomena, automatic obedience, verbigeration, and other stereotypies—have been abstracted. Weak relationships of the first pattern with mania and schizophrenia and of the second pattern with mania alone were suggested in these studies.
Delineation From Other Syndromes (Differential Diagnosis)
Elective mutism, metabolic-induced stupor, Parkinson’s disease, malignant hyperthermia, locked-in syndrome, and stiff-person syndrome are similar to but distinguishable from catatonia
(5,
6). Elective mutism is usually associated with preexisting personality disorder, identifiable stressors, and no other catatonic features. Lorazepam (or amobarbital) challenge, to which 50%–70% of patients with catatonia respond, may not resolve elective mutism
(66). Mutism also occurs in stroke, but other focal neurologic signs and stroke risk factors are frequently present, while other catatonic features are not. The mutism of the locked-in syndrome is associated with total immobility except for vertical eye movements and blinking. These patients typically try to communicate by these movements, whereas patients with catatonia make little or no effort to communicate. Unlike the primary akinetic mutism of catatonia, the mutism of locked-in syndrome is accompanied by no other catatonic features, does not respond to lorazepam challenge, and is usually associated with lesions in the ventral pons and both cerebellar peduncles
(67). The stiff-person syndrome is associated with painful spasms that are precipitated by touch, noise, or emotional stimuli. Baclofen, which can relieve stiff-person syndrome, may induce catatonia
(68).
Malignant hyperthermia looks like malignant catatonia and has been associated with neuroleptic malignant syndrome
(26). Malignant hyperthermia is an autosomal dominant transmitted muscle sensitivity to inhalation anesthetics and depolarizing muscle relaxants that is confirmed by muscle biopsy. Malignant hyperthermia occurs after a surgical procedure.
Akinetic parkinsonism also resembles catatonia. Patients with akinetic parkinsonism may be mute and immobile and may posture
(69). This condition usually occurs after years of illness with parkinsonian symptoms and dementia. Benzodiazepines do not relieve akinetic parkinsonism, but anticholinergic drugs may provide some benefit.
Stupor is a DSM criterion for catatonia (see later discussion). Stupor that is caused by a metabolic disorder or that is associated with delirium may present with catatonic features
(5,
49). Neuroleptic malignant syndrome and nonconvulsive status epilepticus are causes of stuporous states associated with signs of catatonia. Benzodiazepine withdrawal has been associated with a delirious nonconvulsive status epilepticus with catatonia
(70). EEG results constitute diagnostic criteria for nonconvulsive status epilepticus, but they are not helpful in distinguishing delirium or neurologic stupor from malignant catatonia, as each condition is associated with diffuse EEG slowing
(71).
Distinguishing catatonic excitement from manic excitement is problematic. Both states seem purposeless, are sudden in onset, and are of short duration. Both are associated with psychosis. That so many patients with catatonia meet the criteria for manic-depressive illness further blurs distinctions. Kahlbaum
(1,
2) and Bleuler
(4) introduced the concept of excitement periods in a catatonic episode, but in delineating these periods, they seemed to be describing manic episodes. Kahlbaum characterized catatonic excitement by “hystrionic exaltation, expansive mood permeating all speech [with] constant declamations and recitations accomplished by lively gesticulations [and] sudden short-lived joy”
(2, pp. 33–34). Bleuler
(4) described catatonic excitement as a “hyperkinetic [state] with flight of ideas [during which the patient will] cry, sing, verbigerate, laugh, curse, scream, and spit. They grimace, showing sadness, happiness or horror.” Other than by the presence of catatonia, the mania associated with catatonia cannot be distinguished from mania without catatonia
(14,
15,
33,
48). A parsimonious conclusion is that the validity of catatonic excitement is unproven, and the presence of excitement during a catatonic episode indicates an underlying manic-depressive illness.
Catatonia by Other Names
Malignant catatonia has been described under various sobriquets since 1849, long before the antipsychotic drug era
(72). The hallmarks of malignant catatonia are acute onset of excitement, delirium, fever, autonomic instability, and catalepsy. Until the advent of ECT, most patients died
(72–
74). The term “neuroleptic malignant syndrome” was applied when the condition was associated with exposure to antipsychotic drugs. Neuroleptic malignant syndrome was assumed to result from the dopaminergic blockade characteristic of these agents
(26). Despite their selective dopamine blockade, all atypical antipsychotic drugs can induce neuroleptic malignant syndrome, although they are less likely than conventional antipsychotics to do so
(75,
76). The characteristics of neuroleptic malignant syndrome and malignant catatonia cannot be distinguished either clinically or by laboratory testing, leading to the present consensus that neuroleptic malignant syndrome is a specific example of malignant catatonia
(26–
29,
77–79). Further weakening the distinction of neuroleptic malignant syndrome from catatonia are reports that certain nonneuroleptic drugs can induce the condition
(28,
80–84). Further, in treatment trials based on the similarities between neuroleptic malignant syndrome and malignant catatonia, benzodiazepines and ECT—the standard treatments for malignant catatonia—have proved successful in the treatment of patients with neuroleptic malignant syndrome
(85–
89). The toxic serotonin syndrome is also similar to malignant catatonia; except for the gastrointestinal features of the former syndrome, the two are indistinguishable
(28,
30,
90,
91). Neuroleptic malignant syndrome and the serotonin syndrome are most likely severe forms of catatonia that are induced by agents with different chemical characteristics. Their treatment is also the same as that for malignant catatonia.
Other conditions that are commonly associated with catatonic features include delirious mania
(92–
96) and benign stupor
(97–
100). Patients with these syndromes exhibit many signs of catatonia and respond to treatments for catatonia. A specific designation for catatonia in psychiatric classification systems would encourage the incorporation of many syndromes into a single disorder that responds well to the treatment algorithm of benzodiazepines and ECT
(101).
Of the catatonia variants, stupor presents difficulties for differential diagnosis because it is elicited by so many neurologic and metabolic disorders. Also, unlike delirious mania or the serotonin syndrome, stupor is a specific DSM criterion for catatonia and a classic feature described by Kahlbaum and virtually all other writers on the subject. Definitions of stupor in catatonia that are based on the simultaneous presence of other catatonic features skirt the issue of directly defining stupor
(102). Attempts to discriminate between stupor related to a psychiatric condition and stupor caused by a recognized neurological disease have not been helpful, given recent findings of brain changes in catatonic patients who respond well to lorazepam or ECT
(5). Plum and Posner
(103) define stupor as a state of unresponsiveness from which the patient can be aroused only by vigorous and repeated stimuli and back into which the patient lapses as soon as the stimuli cease. This description is consistent with the literature on catatonia.
Good Response to Specific Treatment
No study of treatment efficacy for catatonia has fully met current standards for evaluating therapies. The systematic trials with meaningful sample sizes are either naturalistic
(5,
6) or refer to the more malignant forms of catatonia. A meta-analysis or other statistical analysis for pooling multiple-source databases has also not been done. Despite these shortcomings, the literature is remarkably consistent—from the first reported patient treated with amobarbital in 1930
(104) to the first dementia praecox patient (with catatonia) treated with convulsive therapy in 1934
(105) to the many positive reports in the past decade. It has compelling face validity. Modern investigators of catatonia conclude that drugs with anticonvulsant properties, particularly benzodiazepines and barbiturates, and ECT effectively relieve or resolve catatonic episodes regardless of their severity or etiology
(84,
106–110).
The number or pattern of catatonic features does not affect outcome, and the syndrome has an excellent acute treatment prognosis. The patient’s long-term prognosis depends on the underlying condition that elicited catatonia
(9,
12,
13). Exposure to either typical or atypical antipsychotic drugs, however, usually worsens catatonia or induces the malignant form
(111–
114).
Common Causes of Catatonia
Mood Disorder
Despite the historic linkage of catatonia with schizophrenia, catatonic episodes are most commonly associated with mood disorder, particularly mania. The more severe the mania, the more likely that catatonic features will also be present. Kahlbaum
(1,
2) observed that most catatonic episodes were preceded by episodes of depression and mania. Bleuler
(4) commented that “as a rule catatonic symptoms mix with the manic
and the melancholic conditions” (emphasis ours). Kraepelin
(3,
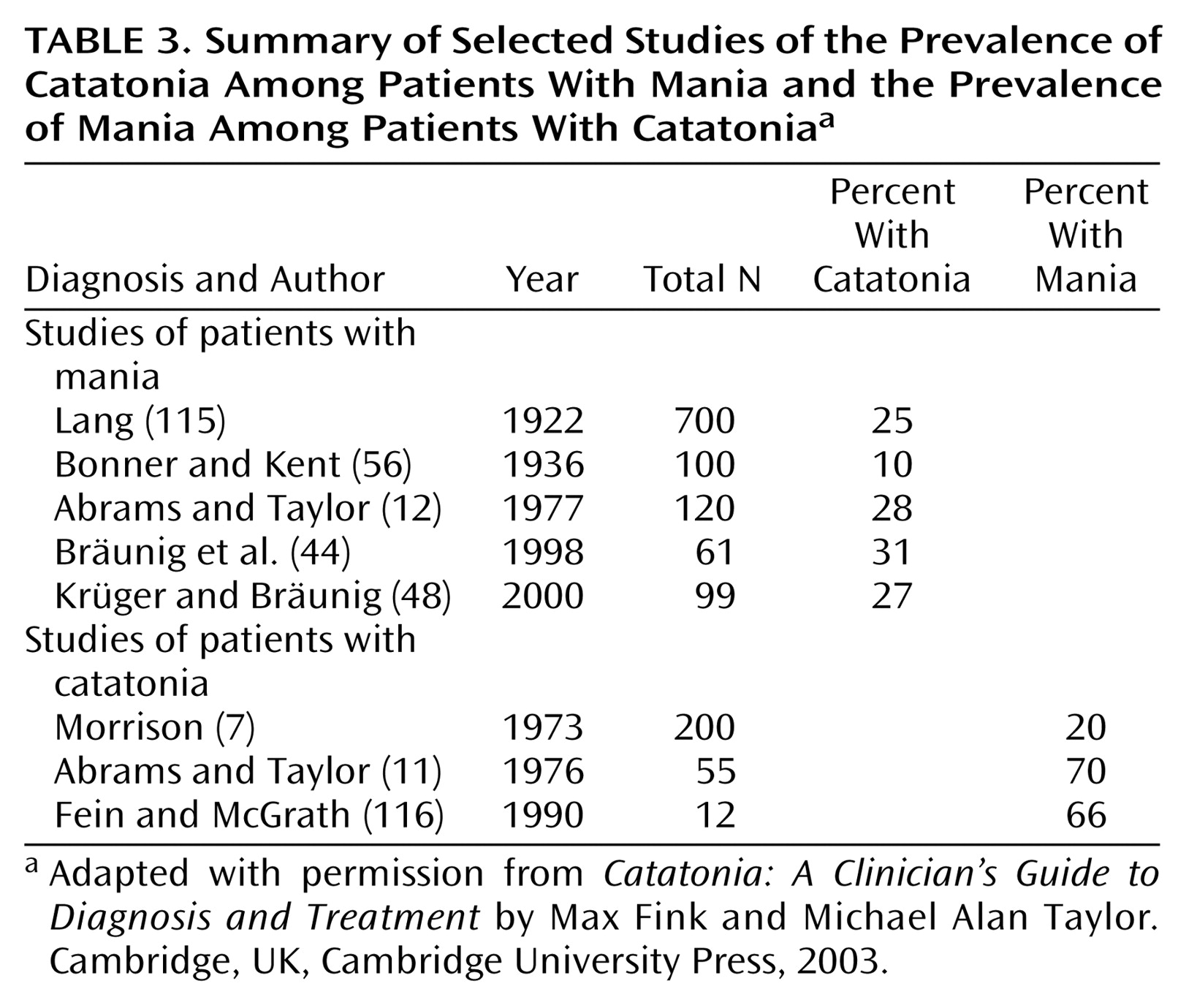
33) reported that nearly 50% of catatonic attacks begin with a depressive episode, that catatonia is often associated with mania, and that dementia praecox patients with catatonia were likely to recover. Many authors link catatonia to manic-depressive illness (
Table 3). Their findings suggest that 25% or more of manic patients have enough catatonic features to meet the DSM criteria and that more than half of catatonic patients have manic-depressive illness.
General Medical and Neurologic Conditions
Catatonia is a feature of many general medical conditions
(5,
11,
16,
49). Metabolic disturbances, endocrinopathies, viral infections (including HIV), typhoid fever, heat stroke, and autoimmune disease, all of which are commonly associated with delirium, are also associated with catatonia. Drug intoxications and withdrawals may induce catatonia. These drug-related conditions include exposure to antipsychotic drugs
(16,
25,
26,
57,
75,
76,
81) and illicit recreational drugs
(49,
117,
118), withdrawal from benzodiazepines
(119) and dopaminergic drugs
(120), and opiate intoxication
(121). Neurologic conditions associated with catatonia include postencephalitic states, parkinsonism, bilateral globus pallidus disease, thalamic and parietal lobe lesions, frontal lobe disease, and general paresis
(11,
16,
122–124). In children, catatonia may be caused by a developmental or seizure disorder
(125).
Nonaffective Psychoses
About 10%–15% of patients with catatonia meet the criteria for schizophrenia when the diagnosis requires no past or present episodes of mood disorder. Catalepsy, mannerisms, posturing, and mutism are the features traditionally associated with catatonic schizophrenia
(7,
10,
126–128).
Genetic Form of Catatonia
German psychopathologists, beginning with Wernicke, Kleist, and Leonhard, and more recently students at the University of Würzburg, defined putative subsyndromes of catatonia that are not delineated in the DSM or ICD. One form of catatonia has been described as familial and as having a suspected major gene effect
(18–
23). A follow-up study of these patients found their prognosis to be poor, and benzodiazepines and ECT were deemed unhelpful
(129). The fact that so many catatonic patients have manic-depressive illness, which is itself highly heritable, makes interpretation of the Würzburg findings difficult, and it is unclear how best to integrate their subdivision of catatonia into general classification systems.
A Unique Category for Catatonia in Psychiatric Classification
The present diagnostic criteria for catatonia are problematic because they are not formulated to account for the differential diagnostic concerns described in the previous sections. For example, the DSM criteria for catatonia are nonspecific and redundant (
Table 1). Stuporous patients, for example, are often mute. They would meet criteria 1 and 3 and could be labeled catatonic, although stuporous and mute patients are not all catatonic
(99). To suggest that they are would dramatically broaden the category and the prevalence of catatonia. Catalepsy often appears as posturing; thus, patients with this single sign fulfill criteria 1 and 4. On the other hand, some catatonic patients seem purposeful in their mutism and negativism, and some manic patients seem purposeless in their excitement, limiting the utility of these descriptors. Last, there is no duration criterion. Rating scales typically require a duration criterion to enhance reliability. Some modification of these criteria would strengthen the boundaries of the syndrome, facilitating further study and the application of appropriate treatments.
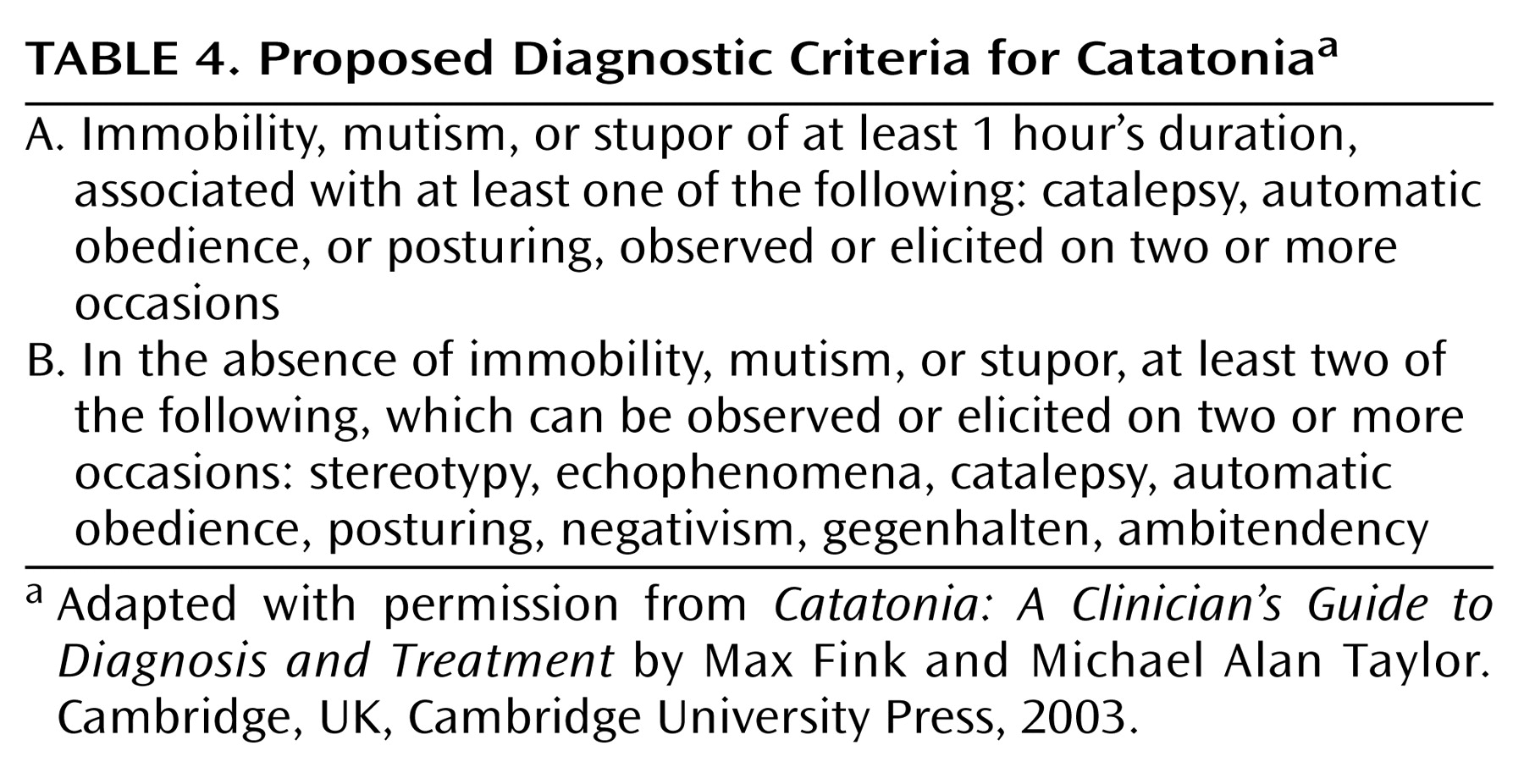
In DSM-IV, catatonia remains mainly as a subtype of schizophrenia (DSM-IV code number 295.20). The less prominent alternatives of catatonic disorder due to a general medical condition (293.89) and catatonia as a specifier for some mood disorders (296.4x–296.5x) are too restrictive and do not reflect the most common etiologic linkages to catatonia described in earlier sections of this paper. We suggest that catatonia be classified separately from other syndromes, similar to the identification and classification of delirium. We also propose modifications to the criteria for catatonia (
Table 4).
Psychiatric diagnostic classifications have a separate category for delirium, a phenomenon that cuts across specific “illnesses” and that is not anchored in any one diagnosis. Clinical practice typically requires a syndrome to be recognized before the etiology can be determined and the pathophysiology corrected. If the presence of delirium is not recognized, morbidity and mortality may be increased, either by the delirium itself or the processes that caused the delirium. Some types of delirium, e.g., anticholinergic delirium, Wernicke’s encephalopathy, delirium tremens, and nonconvulsive status epilepticus, respond to specific treatment
(130). Delirium is a separate class in diagnostic systems because it is a definable and treatable syndrome that has adverse consequences for the patient when it is not recognized. In DSM-IV, delirium is included as a syndrome within the category “Delirium, Dementia, and Amnestic and other Cognitive Disorders.”
Catatonia is a recognizable and definable syndrome that can be identified as readily as delirium. It has many causes, and it responds to specific treatments. When catatonia is not recognized and not properly treated, it has adverse consequences for the patient
(5,
6,
131,
132). Catatonia could appropriately be included as a syndrome within the DSM-IV category of “Movement Disorders.”
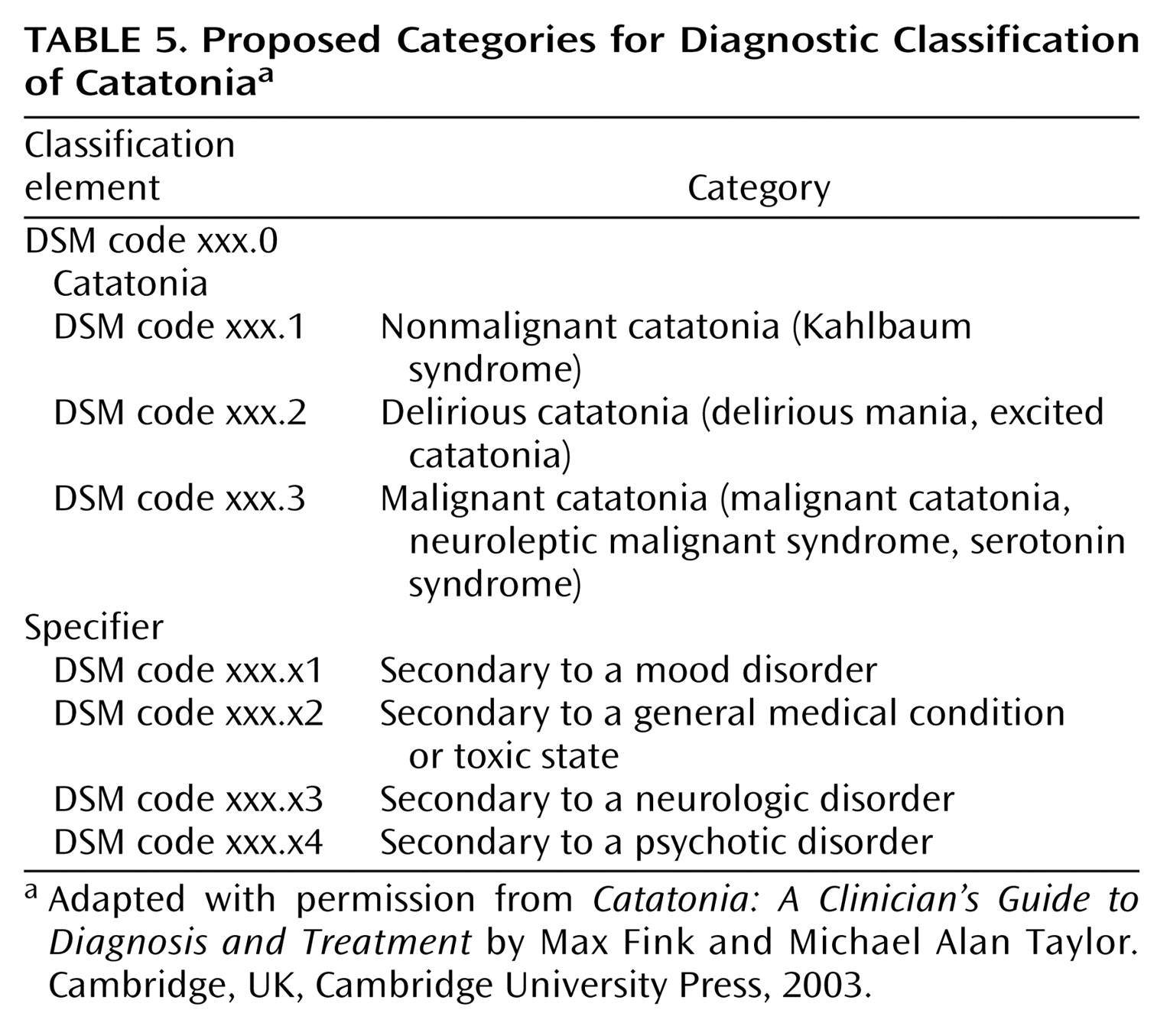
Proposed categories for a classification of catatonia are provided in
Table 5. The subtypes reflect differences in lethality. The nonmalignant form may be referred to as the Kahlbaum syndrome, as recommended by others
(133,
134). It responds to lorazepam (6–20 mg/day). The delirious forms require high doses of lorazepam for relief, respond best to ECT, and are typically made worse by antipsychotic drugs
(111,
112). The malignant forms require life-supportive measures, treatment of fever and dehydration, and high doses of a benzodiazepine; ECT may be required if medication does not quickly resolve the condition
(5,
78,
79,
87,
88). After 4 days, permanent disability may ensue, and the mortality rate associated with malignant catatonia/neuroleptic malignant syndrome rises dramatically, suggesting that a patient with an acute and febrile form of catatonia can be considered at risk of dying.
Our review of the many forms and severities of catatonia suggests that a specifier for etiology is useful. Specifiers facilitate treatment planning and research study. If catatonia resulted from a mood disorder, for example, ECT would be a treatment of choice for both catatonia and mood disorder. If medication were added as the catatonia resolved, mood stabilizers or antidepressants would be the first choices. Catatonia secondary to other disorders, such as a general medical, a neurologic, or a psychotic disorder, warrants other interventions.
Conclusions
We organized the data about catatonia from the extensive literature along the lines suggested by Robins and Guze
(31) for establishing the validity of a syndrome. More recently, Blashfield et al.
(32) offered five criteria to justify the inclusion of a syndrome in a diagnostic system. We find catatonia to meet these criteria—the existence of at least 50 peer-reviewed journal articles discussing the syndrome and the presence of recognized and well-defined syndrome criteria, with at least two independent empiric studies demonstrating interclinician agreement equal to or greater than 0.70. The guidelines of Blashfield et al. also suggest that a patient who meets one criterion for the disorder have at least a 0.50 probability of meeting another criterion for the disorder and that the proposed category can be differentiated from other categories with which it is likely to be confused. Catatonia meets these requirements. Thus, the scientific literature offers substantive support for the identification of catatonia as a distinct nosologic syndrome. We believe that there is a data-supported rationale for the classification of catatonia in a distinct syndrome category. Such a designation will encourage greater identification, more focused treatment, and further research directed at identifying the neurobiologic substrate of the disorder.