Suicide and suicidal behavior are familial. Adoption, twin, and family studies have shown that first-degree relatives of suicide victims and attempters are at higher risk for suicidal behavior
(1). While the familial transmission of suicidal behavior is partly mediated by the transmission of psychiatric disorders
(2,
3), there is up to a 4–6-fold greater risk of suicidal behavior in first-degree relatives of suicide attempters or completers even after controlling for the familial transmission of psychiatric disorder
(2–
13). Impulsive aggressive traits appear to be part of a diathesis for suicidal behavior and may mediate the familial transmission of suicidal behavior
(8,
9,
12,
14,
15).
We recently demonstrated familial transmission of suicidal behavior in the offspring of mood disorder probands who attempted suicide
(16). The familial transmission of suicidal behavior was related, in part, to the familial transmission of sexual abuse and of impulsive aggression. In this report, we extend our findings of familial transmission of suicidal behavior by examining the relationship between family loading for suicidal behavior and familial transmission of suicidal behavior. We compared three proband groups, all adults with a history of a mood disorder separated on the basis of suicide attempt history and family loading for suicidal behavior: 1) suicide attempters with a sibling who also attempted suicide, 2) suicide attempters whose siblings never made a suicide attempt, and 3) nonsuicidal probands whose siblings also never engaged in suicidal behavior. We posited that the offspring of parents with the greatest loading for suicidal behavior would have the highest morbid risk for familial transmission of suicidal behavior and that the familial transmission of suicidal behavior would be mediated partly by higher impulsive aggression in probands and offspring.
Results
Comparison of Proband Groups
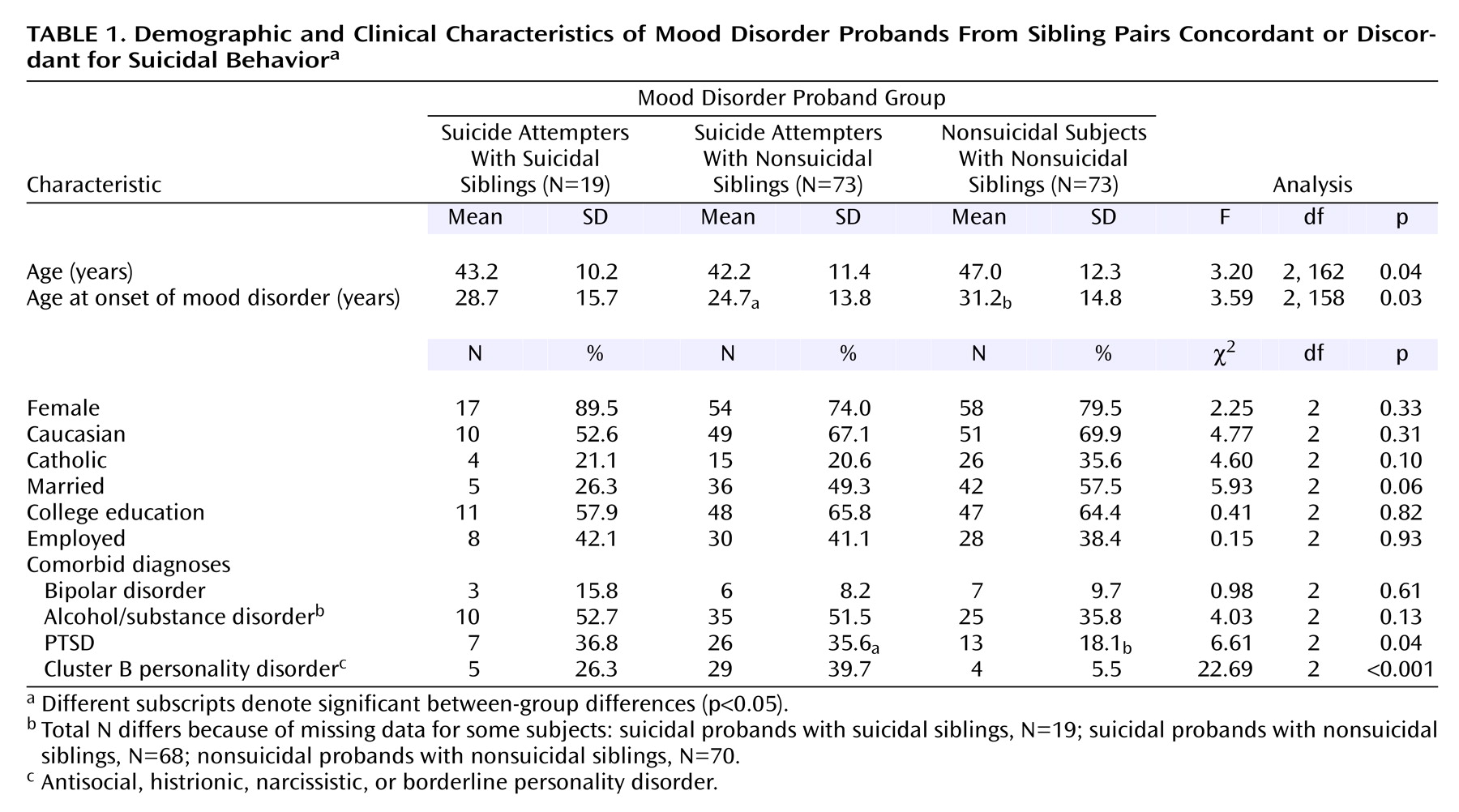
The probands were in their mid-40s and mostly female (
Table 1). All three groups had an age at onset of mood disorder around the age of 30. Pairwise comparison showed that age at onset was younger in the suicidal probands with nonsuicidal siblings than in the nonsuicidal probands. The rate of bipolar disorder or comorbid alcohol/substance abuse did not differ in the three groups. Both suicide attempter groups had higher rates of PTSD and cluster B personality disorders than did the nonsuicidal probands.
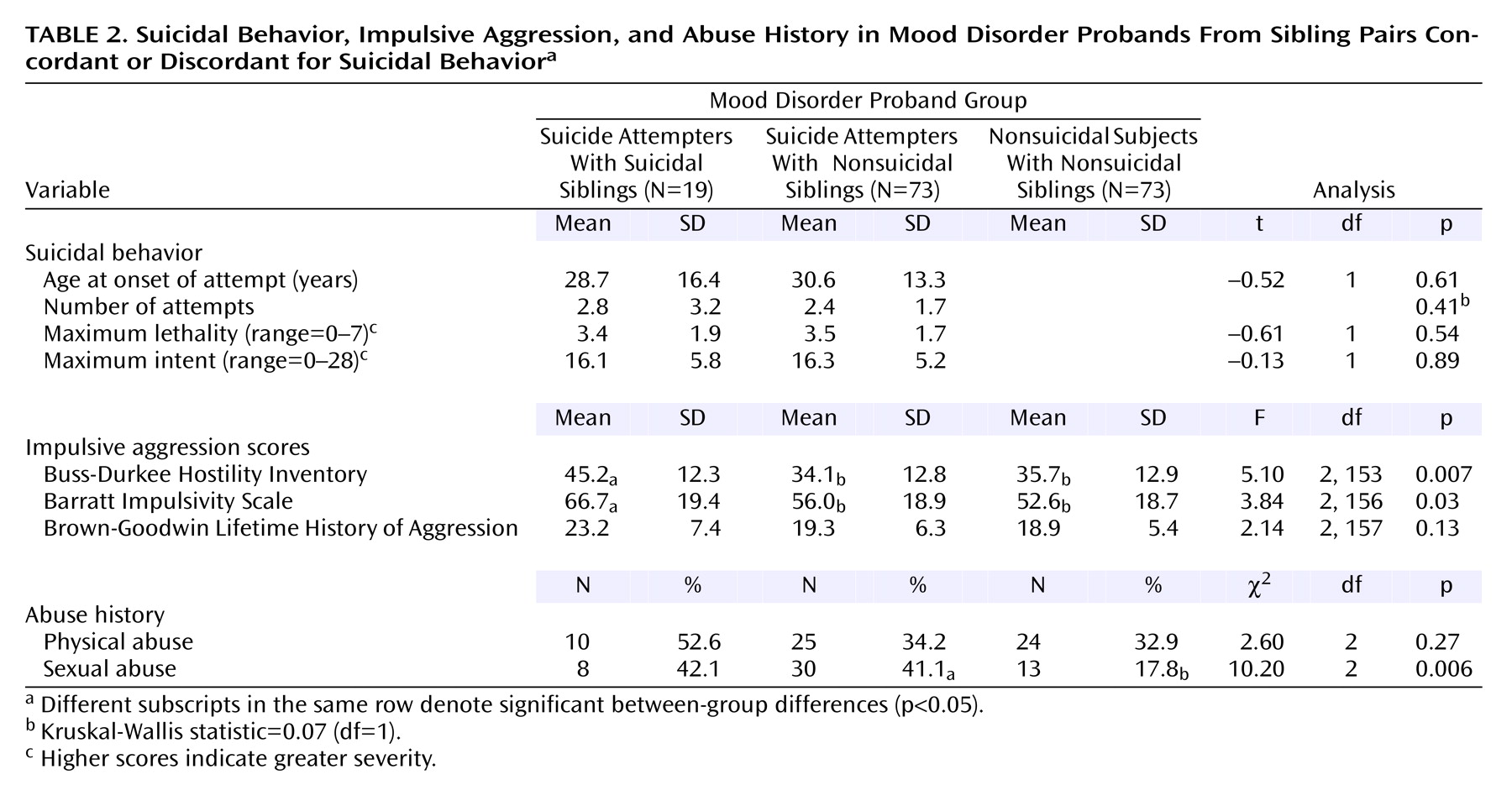
As hypothesized, suicidal probands with siblings concordant for suicidal behavior showed higher levels of impulsivity on the Barratt Impulsivity Scale and higher levels of impulsive aggression on the Buss-Durkee Hostility Inventory than each of the other proband groups (
Table 2). A reported history of sexual abuse was more common in both suicide attempter proband groups compared with the nonsuicidal probands. There were no group differences for physical abuse.
The prevalence of suicidal behavior among first-degree relatives of the three proband groups appeared to be highest in the suicide attempters with siblings concordant for suicidal behavior (10%, compared with 3% and 6% in the suicide attempters with siblings discordant for suicidal behavior and nonsuicidal probands, respectively). The difference, however, was not significant (p=0.14, Fisher’s exact test).
Comparison of Offspring
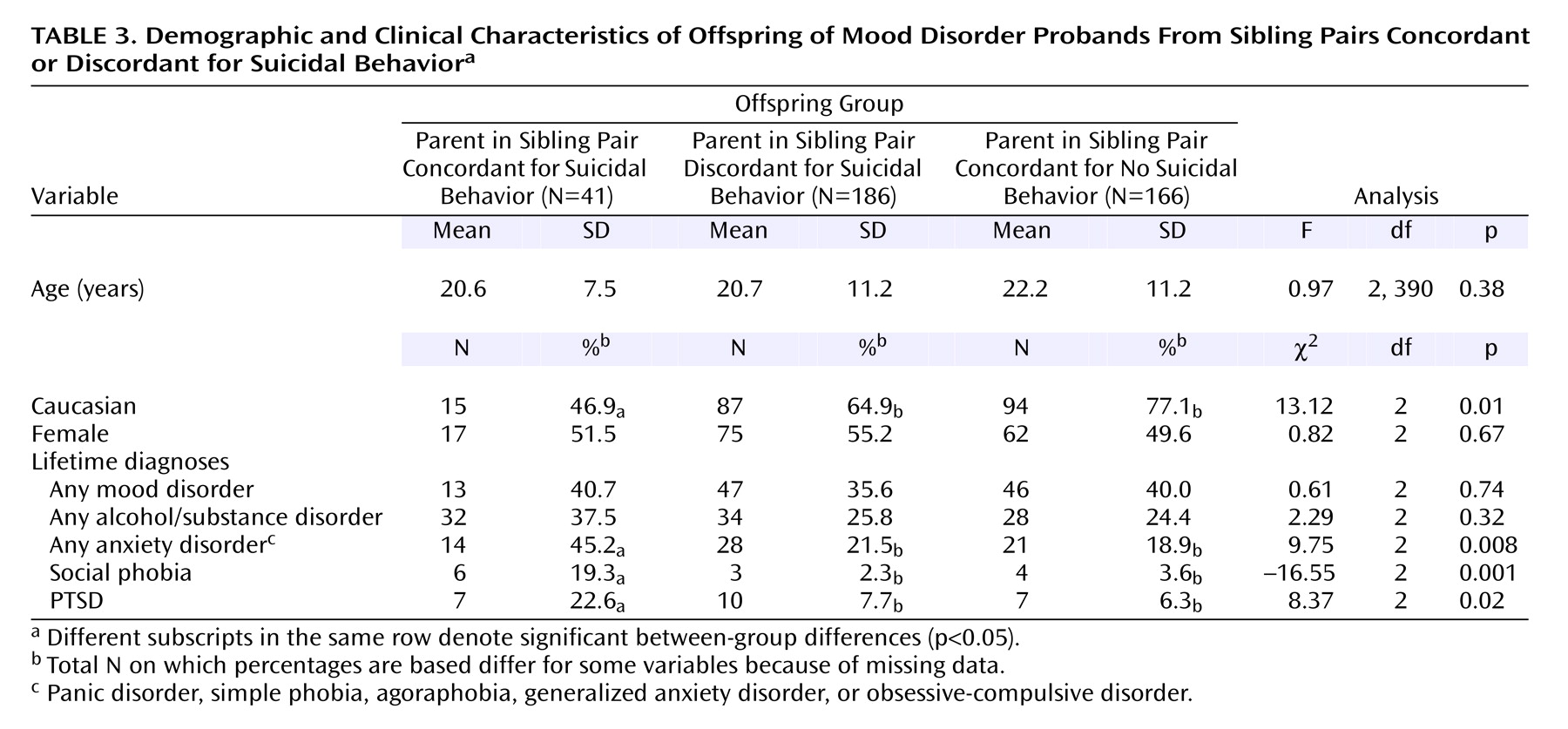
All subjects in the offspring groups were in late adolescence at the time of evaluation (
Table 3). The offspring of probands in the two suicide attempter groups were less likely to be Caucasian. The three groups had similar rates of mood disorders and alcohol/substance abuse but different rates of anxiety, social phobia, and PTSD. Post hoc comparisons showed higher rates of anxiety, social phobia, and PTSD in the offspring of suicide attempters with siblings concordant for suicidal behavior than offspring of the other two proband groups.
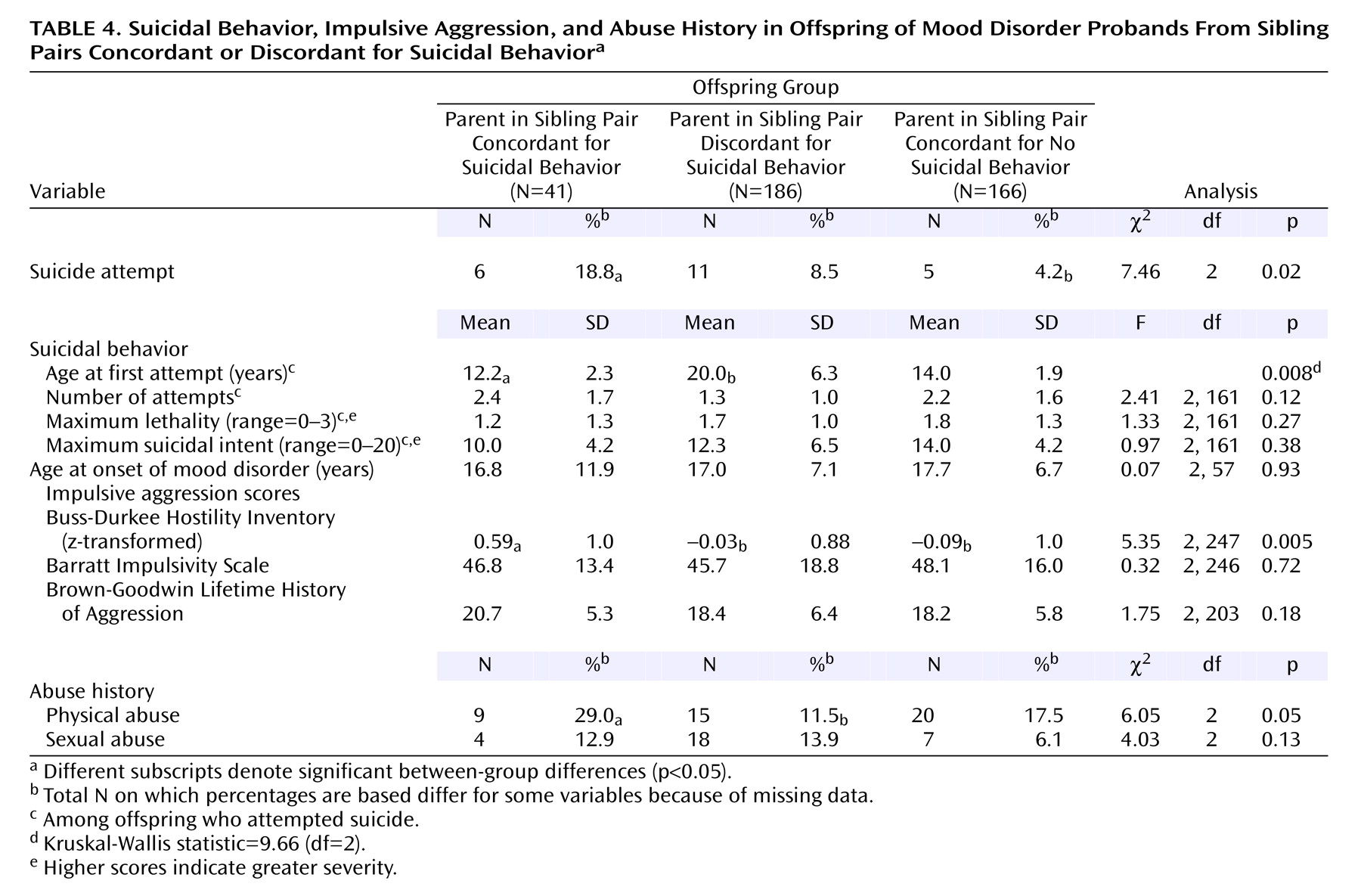
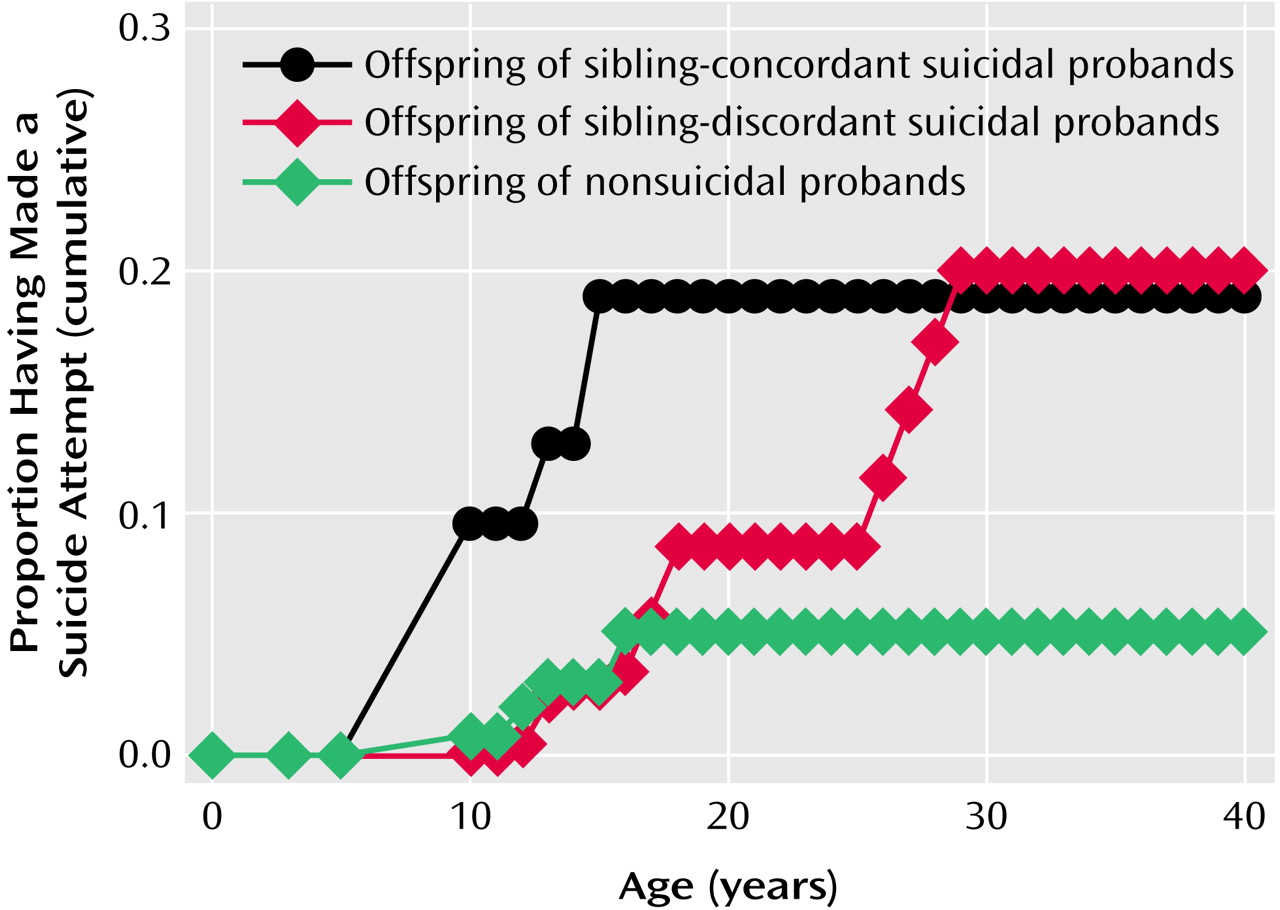
The rates of suicide attempts were different across the three offspring groups, with a significant pairwise difference between offspring of sibling-concordant suicidal probands versus offspring of sibling-discordant suicidal probands (18.8% versus 4.2%) (χ
2=7.90, df=1, p=0.005) (
Table 4). The morbid risk for suicide attempt was similar in the offspring of the two suicide attempter groups (mean=0.18 [SE=0.07] and 0.20 [SE=0.06]), but the age at first suicide attempt was about 8 years earlier in the offspring of sibling-concordant versus sibling-discordant suicidal probands (generalized Wilcoxon χ
2=6.27, df=1, p=0.01). The morbid risk of attempt was much greater in the offspring of sibling-concordant suicide attempters than in the offspring of nonsuicidal probands (mean=0.18 [SE=0.07] versus 0.05 [SE=0.02], respectively) (Wilcoxon χ
2=7.46, df=1, p=0.006) (
Figure 1). However, there was no significant difference in the age at onset of suicidal behavior for offspring of sibling-concordant suicide attempters versus offspring of nonsuicidal probands (Mann-Whitney U=6.5, p=0.51). Suicide attempt followed onset of the mood disorder by a median of 1 year (mean=0.33, SD=5.0) in offspring of sibling-concordant suicide attempters, 2 years (mean=5.0, SD=7.6) in the offspring of sibling-discordant suicide attempters, and 1.5 years (mean=0.5, SD=2.3) in the offspring of nonsuicidal probands.
The ages at first suicide attempt and onset of mood disorders were earlier in the offspring than in probands (Mann-Whitney U=31.50, p=0.003; Mann Whitney U=285.0, p=0.02). Neither lethality nor number of lifetime suicide attempts differentiated offspring of sibling-concordant suicide attempters from offspring of sibling-discordant suicide attempters. However, the maximum medical damage and suicide intent were lower in the offspring than in the proband parents (medical damage: t=4.57, df=107, p<0.0001; suicide intent: t=3.37, df=107, p=0.0005).
Suicidal probands with siblings concordant for suicidal behavior appeared to be more likely to have at least one sibling with a mood disorder (58%) than suicidal probands with nonsuicidal siblings (36%) and nonsuicidal probands (29%), although this was not statistically significant (χ2=5.6, df=2, p=0.06). In addition, the sibling pairs concordant for suicidal behavior were more likely to have at least one first-degree relative with a mood disorder (89% versus 45% versus 51%) (χ2=12.1, df=2, p=0.002).
Offspring of probands in sibling pairs concordant for suicidal behavior had higher levels of impulsive aggression than did the other two offspring groups. There were no group differences in impulsivity on either the Barratt Impulsivity Scale or the Conners impulsivity subscale. There were no differences in the rates of reported childhood sexual abuse among the three groups, but the rates of reported physical abuse were higher in the offspring of sibling-concordant suicidal probands than sibling-discordant suicidal probands.
Logistic and Cox Regressions
Proband and offspring variables that differentiated the sibling-concordant suicide attempter group from the other two groups were entered into a logistic regression. Only offspring impulsive aggression survived this logistic regression (odds ratio=2.0, 95% confidence interval [CI]=1.0–4.0; Wald χ2=4.12, df=1, p=0.04). Offspring impulsive aggression and proband concordance status were entered into a Cox regression predicting age at first offspring suicide attempt. Only offspring impulsive aggression was significant (odds ratio=2.2, 95% CI=1.3–3.8; Wald χ2=8.85, df=1, p=0.003), whereas proband concordance status, which was significantly associated with offspring attempt in the univariate analysis (odds ratio=2.9, 95% CI=1.1–7.3; Wald χ2=4.78, df=1, p<0.03), now escaped statistical significance (odds ratio=2.1, 95% CI=0.8–6.1; Wald χ2=1.77, df=1, p=0.18). This supports our hypothesis of impulsive aggression mediating the relationship between sibling-pair concordance for suicide attempt status and early-onset offspring suicide attempt.
Discussion
In this study, we found that greater familial loading for suicidal behavior in the proband generation was associated with 1) a greater risk of suicidal behavior and earlier age at first suicide attempt in offspring as well as 2) greater impulsive aggression in both parents and offspring. Offspring impulsive aggression was related to risk for suicide attempt and earlier age at first attempt. The seriousness of the suicidal behavior, as measured by lethality and number of attempts, was similar in the offspring of sibling-concordant and sibling-discordant suicidal probands. Offspring were younger at the time of their first suicide attempt and first episode of major mood disorder than their proband parents and had lower intent and lethality of suicidal behavior.
Greater familial loading for suicidal behavior was associated with a higher risk of suicide attempt among offspring. Offspring of suicide attempters with a sibling concordant for suicidal behavior were at highest risk for suicide attempt, offspring of suicide attempters with nonsuicidal siblings were intermediate, and offspring of nonsuicidal probands had the lowest risk for attempt. This dose-response relationship between familial loading for suicidal behavior and risk for offspring attempt further supports the conclusion that suicidal behavior is familially transmitted
(2–
18).
Familial loading for suicidal behavior was also associated with earlier age at onset of suicidal behavior. Specifically, the offspring of sibling-concordant suicide attempters showed the earliest age at onset of suicidal behavior—a full 8 years on average before the first suicide attempt by offspring of suicide attempters with nonsuicidal siblings. However, the few offspring of nonsuicidal probands who made suicide attempts also had their first attempt at a relatively early age. Thus, there are other explanations for early age at first suicide attempt besides familial loading for suicidal behavior.
The single most powerful predictor for familial transmission of suicidal behavior and of early first attempt in offspring was impulsive aggression in offspring. Impulsive aggression was highest in the suicide attempters with siblings concordant for suicidal behavior and in their offspring. Thus, it is likely that familial transmission of early-onset suicidal behavior is related to the transmission of impulsive aggression. Previous studies have shown a relationship between impulsive aggression in probands and families and familial loading for suicidal behavior
(1,
8,
9,
12,
14,
16,
31). Impulsive aggression has been consistently implicated in the phenomenology and neurobiology of suicidal behavior
(1,
32). However, there are multiple pathways to impulsive aggression and to early-onset suicidal behavior, such as by a history of sexual or physical abuse
(33). The offspring of the nonsuicidal probands who themselves attempted suicide had a particularly high rate of physical or sexual abuse (three of five subjects), which might have accounted for their early first suicide attempt, as has been reported in other studies
(33–
35).
Since mood disorder preceded suicide attempt in offspring, factors that lead to an earlier age at onset of mood disorder might thereby lower the age at first suicide attempt. Familial loading for mood disorders is related to earlier age at onset of mood disorder
(36). The sibling-concordant suicide attempter group did have the highest loading of mood disorder in proband first-degree relatives, but this did not account for an earlier age at first suicide attempt in offspring. This may be because the familial loading for mood disorder was already so high in all three proband groups.
We have identified factors related to predicting early onset of mood disorder (unpublished 2002 study of D. Brent et al.), namely impulsive aggression in offspring, physical abuse in offspring, and offspring comorbid anxiety. Impulsive aggression predicts early onset of both mood disorder and suicidal behavior. Thus, transmission of impulsive aggression may influence onset of suicidal acts by increasing the propensity to act on powerful feelings and by earlier onset of a major depressive episode.
Comorbid anxiety was more common in the offspring of the sibling-concordant suicide attempters. However, after impulsive aggression was controlled, anxiety did not predict earlier age at first suicide attempt. Anxiety disorders are often a precursor of mood disorders and in our study may herald the onset of major depression, which in turn leads to suicidal acts
(37–
39).
In our previous report, we found that the familial transmission of suicidal behavior was mediated by the familial transmission of sexual abuse
(16). However, there were no differences in the rates of sexual abuse between either the sibling-concordant and sibling-discordant suicide attempters or their respective offspring groups. There was a higher rate of physical abuse in the offspring of sibling-concordant suicide attempters, but in this study group, physical abuse was not related to the familial transmission of suicide attempt. Other studies have recognized the deleterious effects of physical abuse but also find that a suicide attempt history is more closely related to sexual rather than physical abuse
(40). Thus, the earlier age at onset of suicidal behavior in offspring of sibling-concordant suicidal probands was not related to a history of abuse in the probands or the offspring but was related to the severity of impulsive aggressive traits in the offspring. However, other studies have reported a relationship between sexual abuse and early onset of suicidal behavior and with impulsive aggression
(33–
35,
41).
The age at first suicide attempt was much earlier in the offspring than in probands, and the maximum lethality and intent were much lower in the offspring than in probands. This could be an artifact of recall bias, in which probands have failed to accurately recall their earlier, less serious suicide attempts. Alternatively, the offspring of attempters may have greater familial loading for suicidal behavior than their parents and consequently have an earlier age at first attempt. Offspring of both suicide attempter groups had first attempts of similarly low intent and lethality, despite the older age at onset in the offspring of the sibling-discordant suicidal probands. Suicidal behavior may begin early in life with relatively low intent and lethality and increase in crescendo-like fashion with age. This is consistent with studies that have compared older and younger suicidal subjects as well as studies that have followed suicide attempters longitudinally
(42–
46).
These results support the utility of collecting concordant sibling pairs for the genetic study of suicidal behavior as well as for the role of impulsive aggression as an “endophenotype” for suicidal behavior. Future studies that examine siblings concordant for suicide attempts may shed light on the genetics of suicidal behavior and of impulsive aggression.
This study should be viewed in the context of its limitations. Most of the probands and offspring who attempted suicide were female, so this study is most informative about female-to-female transmission of suicidal behavior. The proband group was restricted to those with mood disorders, particularly major depressive disorder, which has the benefit of increasing homogeneity but therefore does not address the familial transmission of suicidal behavior in the context of other psychiatric disorders, including bipolar disorder. The probands were recruited from inpatient facilities, where the disorders are more severe rather than representative. While a sibling-concordant suicide attempt group implies greater family-genetic loading for suicidal behavior, a greater risk of suicidal behavior in the proband generation could be due to a shared adverse family environment, such as abuse or neglect. Additionally, the familial transmission of suicidal behavior could be explained by imitation. Previous studies of twins and of parent-child pairs have looked at the wide variability between the twins of relative attempts and concluded that imitation is not a major explanation of the familial transmission of suicidal behavior
(18). Nevertheless, even within the context of these limitations, our results are consistent with findings from both referred and nonreferred patient groups and support further investigation of genetic traits related to suicidal behavior.
The strikingly early age at onset of suicidal behavior in the offspring of mood disordered suicide attempters with siblings concordant for suicidal behavior suggests risk factors that can be targets of early prevention. Replication of this study and early treatment and prevention studies are the next steps.