Historically, suicide has been associated with axis I psychiatric disorders
(1). It has become increasingly apparent that axis II personality disorders are also very relevant, especially when comorbid with axis I disorders
(2). In two studies of subjects who committed suicide compared with subjects from the general population, comorbidity of psychiatric and personality disorders was the largest risk factor for suicide
(3–
5). Such comorbidity is also common in patients who attempt suicide
(6–
10) and adds to their general risk of eventual suicide
(11).
The reasons why extreme personality characteristics increase suicide risk, particularly when combined with psychiatric disorders, have received little research attention
(10). Personality traits thought to increase the risk of suicidal behavior include aggression
(10,
12), impulsivity
(10,
13), and poor problem-solving skills
(14). Mann and colleagues
(10) proposed a stress-diathesis model, including such characteristics as vulnerability factors, to explain the propensity for suicidal behavior across psychiatric diagnoses.
In a representative group of patients who had attempted suicide we compared those with and without comorbid axis I and axis II disorders in terms of the nature of their suicide attempts, their backgrounds, psychological characteristics, and outcome to identify factors that might explain the greater risk of suicide in patients with comorbid psychiatric and personality disorders. These factors might then be targeted in treatment and prevention.
Discussion
Comorbidity of psychiatric and personality disorders is increasingly recognized as a major factor in suicide
(4,
5,
34,
35). Far less attention has been paid to investigating this association in suicide attempters
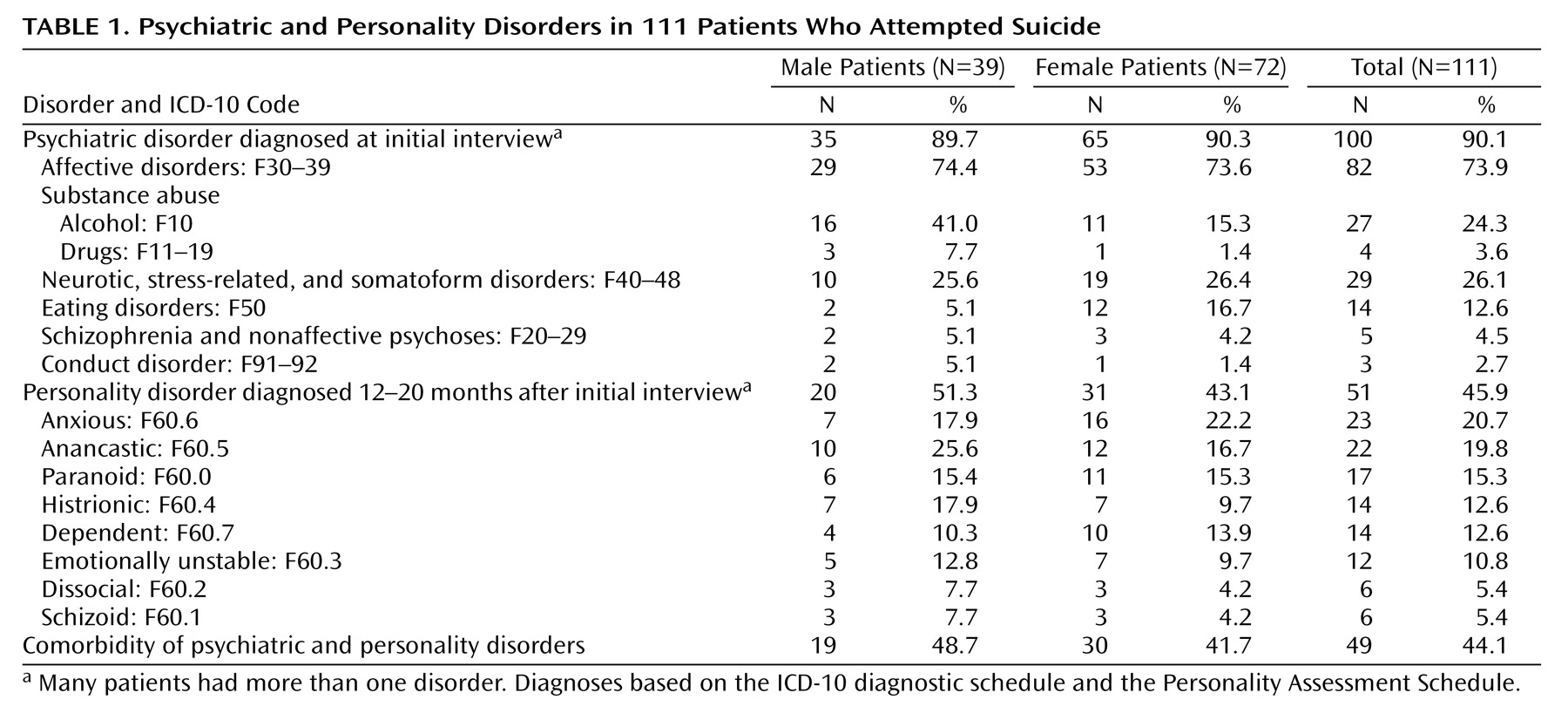
(10). Our finding that 44% of patients who attempted suicide had comorbid psychiatric and personality disorders is similar to the rate found in a study of Finnish suicide attempters
(6) that used DSM-III-R criteria. Emotionally unstable personality disorder (which includes borderline disorder) was not prominent in our patients, probably because of the exclusion of individuals with repetitive minor self-injury based on the recognition that as a group they differ from suicide attempters. Our finding of more cases of anxious personality disorder is similar to the finding in suicide attempters in South Africa
(36).
The study subjects were generally representative of patients who attempted suicide seen in the general hospital where the study was based
(9). Personality was assessed at the follow-up interview, a time when psychiatric disorder is usually less prominent
(29). Although assessment at follow-up also meant that some patients could not be assessed, the patients who were available were representative of the overall initial patient group. Assessment of personality was based on information provided by the subjects themselves because other informants were often not available.
It could be argued that grouping together separate categories of psychiatric and personality disorders is simplistic, but it seems to distinguish two substantially different groups of suicide attempters. Comorbidity of psychiatric and personality disorders, rather than personality disorder alone, appears to be the important factor in determining risk because, as in this study, personality disorder is rarely found by itself in patients who attempt
(9) or complete
(34) suicide.
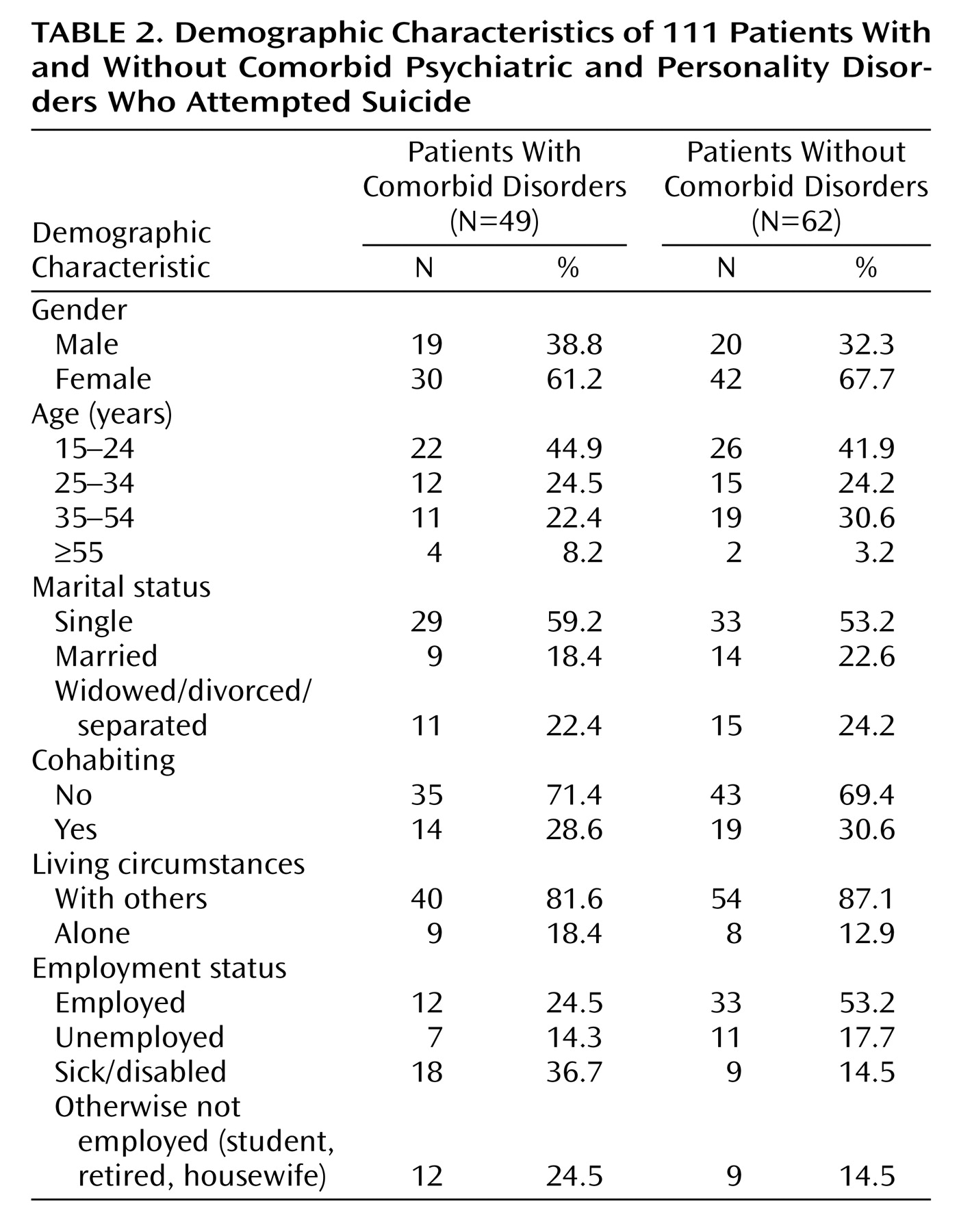
There was little difference in the sociodemographic characteristics of patients with and without comorbid psychiatric and personality disorders, except that fewer of the patients with both disorders were employed. However, more of the suicide attempts of the patients with comorbid disorders were precipitated by difficulty making friends and problems related to addiction, and more were associated with wanting to make others feel guilty, finding their situation unbearable, and wanting to get help.
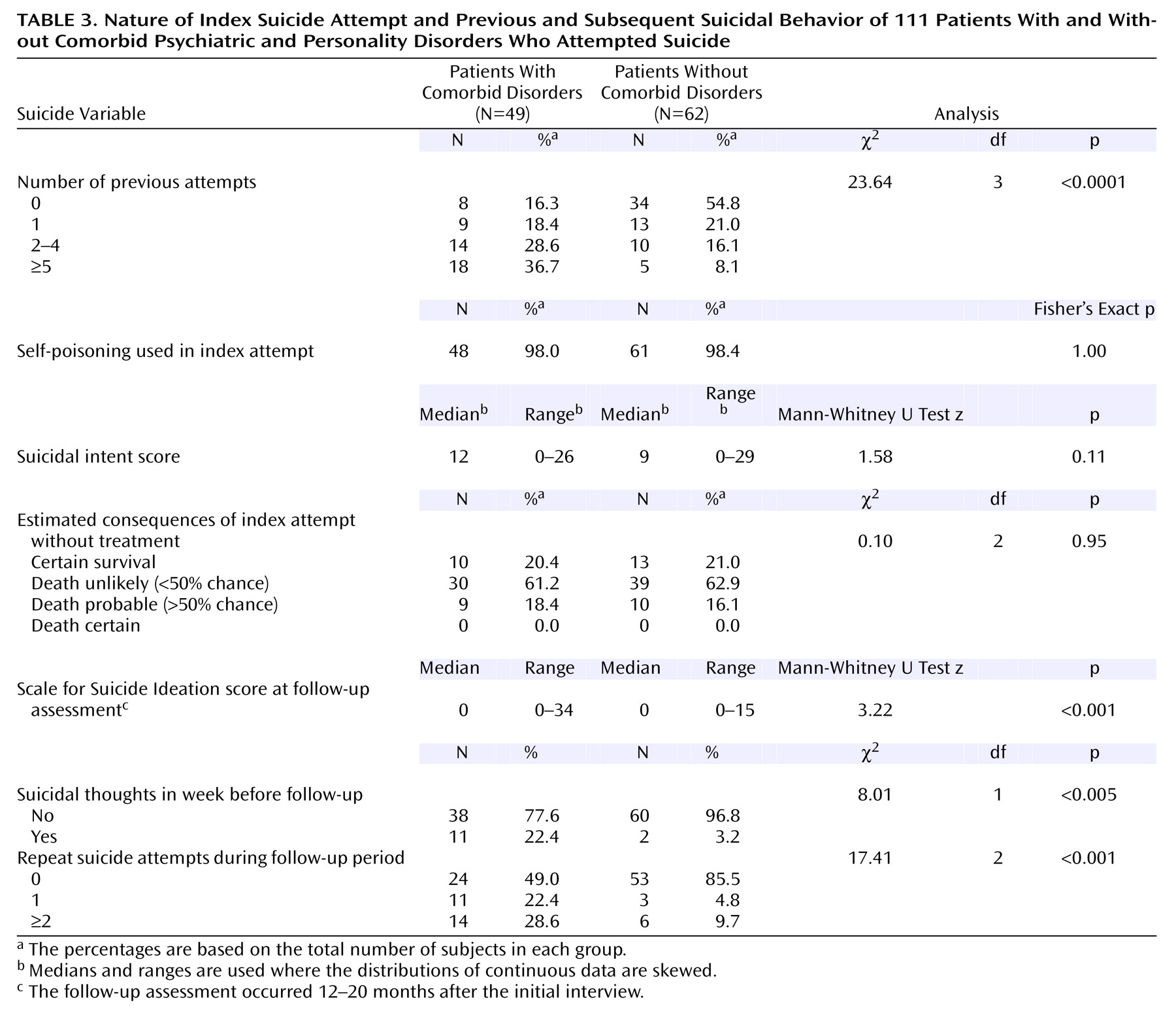
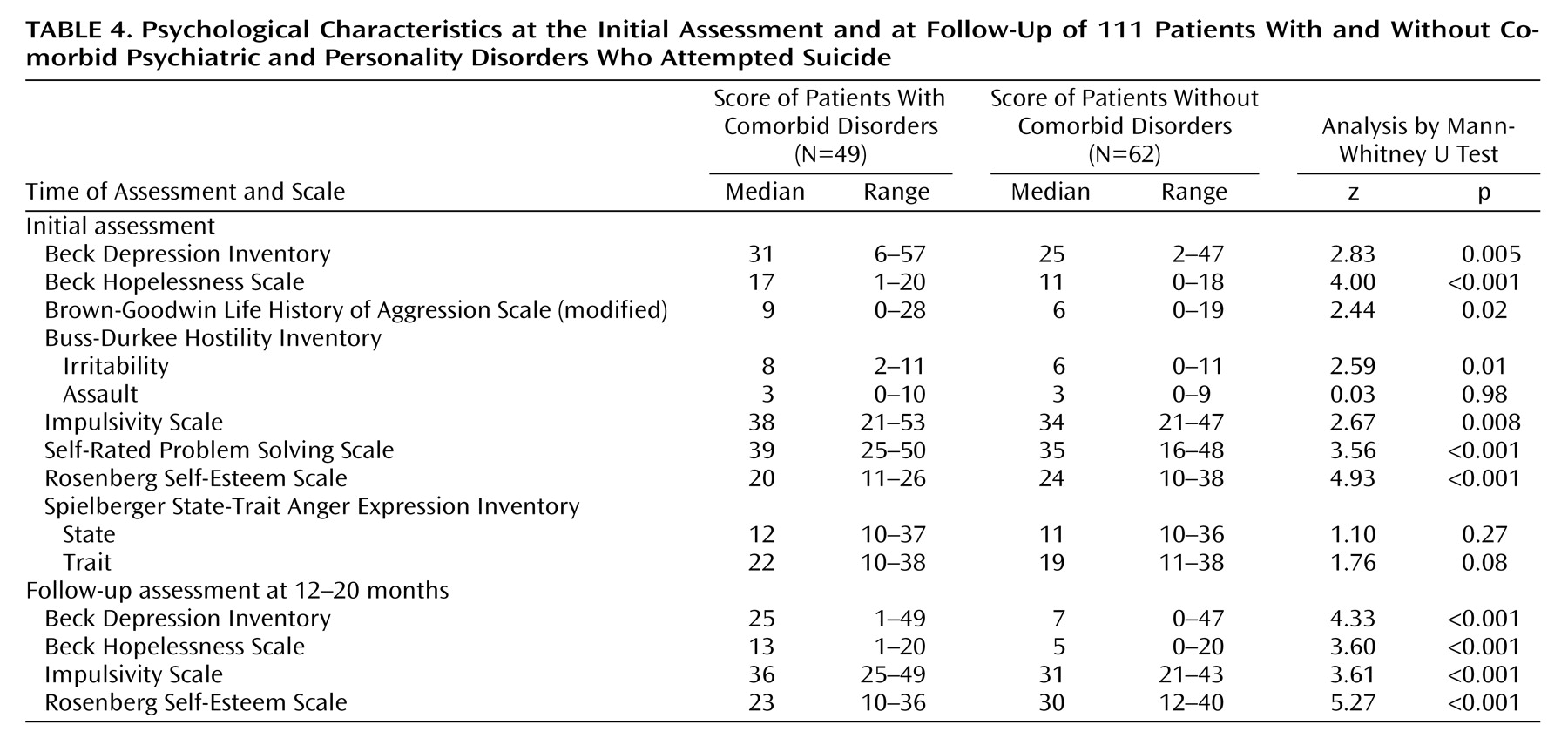
The patients with and without comorbid disorders differed markedly in their psychological characteristics, and most of these differences persisted at follow-up. These included characteristics associated with risk of both attempted and completed suicide, such as persistent depression and suicidal ideas, hopelessness, aggression, impulsivity, and low self-esteem. The greater risk of suicide in the patients with comorbid disorders was also underlined by the greater frequency of previous attempts, particularly multiple attempts, and the more frequent repetition of attempts during the follow-up period.
Multivariate analysis indicated that the key factors distinguishing the patients with and without comorbid disorders were lower self-esteem and poorer self-rated problem-solving skills. Such traits may be exacerbated by psychiatric disorders and increase the likelihood of a suicidal act when an individual is feeling hopeless because of depression or other disorders and is facing seemingly insurmountable problems. This paradigm is in keeping with the stress-diathesis model of Mann and colleagues
(10). Other important factors, such as aggression, a factor known to be important in suicidal behavior
(10), might be secondary to low self-esteem and frustration over difficulties in problem solving.
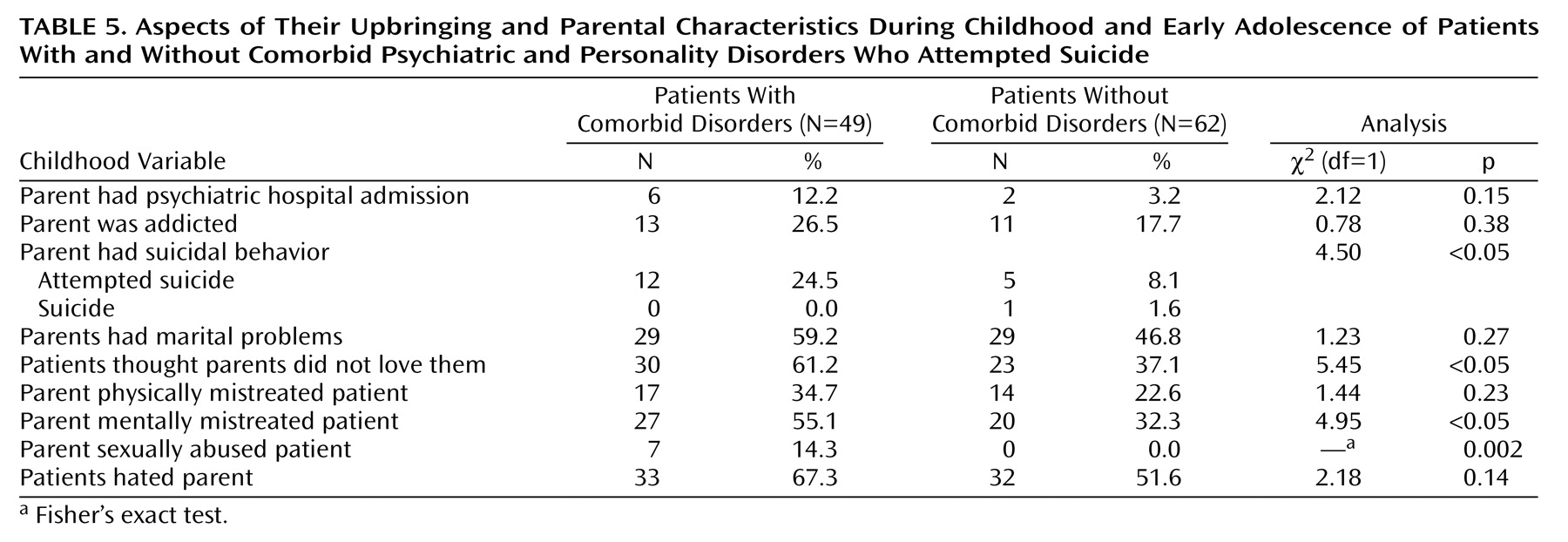
Upbringing, especially feeling unloved by parents, is also likely to have been important in shaping some of the specific characteristics of the patients with comorbid disorders. Genetic influences might also be relevant and may explain the trend for more parental suicidal behavior in the comorbid group.
Comorbidity of personality and psychiatric disorders characterizes an important subgroup of suicide attempters who have a particularly high risk of repeated suicidal behavior. The risk of completed suicide in this subgroup is indicated not only by the frequency of repetition but also by the presence of other risk factors, including persistent depression, suicide ideation, and hopelessness. This risk is underlined by the extent
(3,
34,
35) and relative risk
(4,
5) of this type of comorbidity among individuals who committed suicide compared with control subjects. The impact of comorbidity on risk of suicidal behavior (including repetition) may be attributable to specific characteristics, such as aggression and impulsivity, that increase the likelihood of suicidal behavior as well as the deleterious effects that personality disorders may have on the nature and prognosis of psychiatric disorders.
Prevention of suicidal behavior in individuals with comorbid psychiatric and personality disorders presents a considerable challenge. Clearly, treatment of psychiatric disorders most influencing the immediate suicide risk (e.g., reducing levels of depression and/or substance abuse) must be the first priority. It remains uncertain how best to influence the longer-term psychological characteristics of these individuals, which appear from the present study to include poor problem-solving skills and low self-esteem. Psychological treatments include dialectical behavior therapy, which has promising results for female patients with borderline personality disorders
(37). Mood stabilizers, selective serotonin reuptake inhibitor antidepressants, or low-dose neuroleptics may ameliorate of some of the characteristics that contribute to risk
(38). Multiple therapeutic agencies are often necessarily involved in management, especially where substance abuse is prominent. Intensive treatment may be required to overcome the reluctance of some patients to engage or persist in treatment.
Comorbidity of psychiatric and personality disorders represents one of the major challenges for suicide prevention.