Cigarette smoking became common during the 20th century; many men smoked by the time of World War I, and many women were smoking by World War II
(1). The Surgeon General’s 1964 report on lung cancer and smoking was followed by steadily increasing information about the health hazards of smoking
(2,
3). General monitoring of time trends and correlates has indicated that more men than women smoke, more younger than older people, and, although overall rates have decreased, the decline is more marked among men than women
(4,
5).
Known as the Stirling County Study, the investigation provides a 40-year perspective that makes it possible to observe the associations between depression and smoking over a historical period when use of nicotine increased and then declined. Through repeated cross-sectional surveys, the study gives information about population trends in the prevalence of both smoking and depression as well as trends in their association. Through cohort follow-up investigations, the Stirling County Study provides data on trends exhibited by individuals in terms of initiation, cessation, and continuation of smoking and how these patterns relate to depression.
Method
Site
Data have been gathered in a county in Atlantic Canada with a population of about 20,000
(18,
19). The site was typically rural at the beginning of the study, but major changes have occurred. Service and information industries have burgeoned; women have become a large part of the labor force; educational levels have increased; the media has exerted strong influence; racial tension has increased; and use of drugs and criminal activity have increased. Decreases have occurred in religious activity, marital stability, and family size. Thus, the area exhibits most of the social trends that characterize North American society generally
(20–
22).
To assess the degree to which psychiatric findings about this population are similar or different from those of other areas, the depression portions of the National Institute of Mental Health Diagnostic Interview Schedule
(23) were included in the interviews carried out in the most recent wave of data gathering. The 1-month prevalence of major depressive episodes was 2.6%
(21), which is similar to the 2.2% found in the Epidemiologic Catchment Area (ECA) program
(24,
25) and the 2.3% found in the Edmonton Psychiatric Epidemiology Study
(26). The lifetime rates were also comparable: 7.9% in Stirling County
(21), 6.3% in the ECA program
(24,
25), and 8.6% in Edmonton
(26). Thus, where depression is concerned, the population of Stirling County is like many other populations in North America.
Study Design, Completeness, Interview Procedures
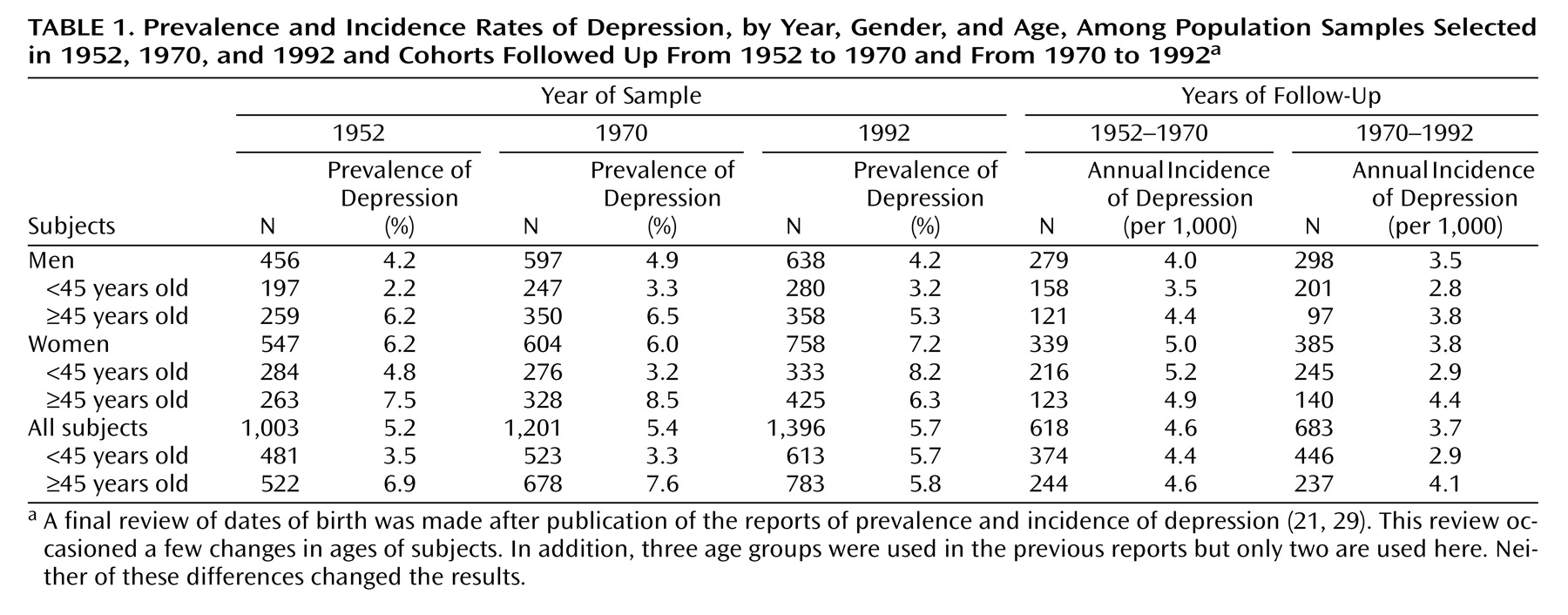
Data for this report derive from three adult population samples selected in 1952, 1970, and 1992 as well as from survivors of the 1952 sample who were reinterviewed in the 1970 survey period (cohort 1) and survivors of the 1970 sample reinterviewed in the 1992 survey period (cohort 2) (
Table 1). Completion rates from both types of investigations ranged from 82% to 92%. Sampling procedures, concerned with adequate representation of the demographic profile of the county, have been described in detail elsewhere
(20–
22).
Subjects were visited in their homes by trained interviewers. The purpose of the study and the nature of the interview were explained verbally, and a written description of the study along with the director’s name and her telephone number was provided when a subject expressed willingness to be interviewed. These procedures have been approved by the Human Research Committee of the Massachusetts General Hospital and by other committees concerned with the ethical protection of human subjects in both the United States and Canada.
Cigarette Smoking
Smoking habits were assessed by two questions. The first, “Do you smoke? Would you say ‘a lot,’ ‘some,’ or ‘not at all’?” was followed by a question about the amount and kind of smoking as “more than 20 cigarettes per day,” “20 or fewer cigarettes,” or “only cigars or pipes.” This study excludes cigars and pipes, and the two levels of daily cigarette smoking are labeled as “heavy” and “moderate.”
In the two earlier samples, among the people who smoked more than 20 cigarettes a day, most (92% in 1952 and 93% in 1970) indicated that they smoked a lot. In 1992, the proportion had dropped to 80%. Nevertheless, the division between heavy and moderate smoking seemed to be meaningful to most smokers.
The information about cigarette smoking is limited to customary daily use at the time of interview. It does not include past history, and subjects were not asked for dates of smoking onset and/or cessation.
Depression
The identification of depression involved the application of procedures called DPAX, where the DP stands for depression and the AX for anxiety
(27,
28). In this article, we deal only with depression and build on reports about its prevalence and incidence over the 40-year period
(21,
29). The DPAX procedures are implemented by computerized algorithms, and the definition of depression involves dysphoric mood as the essential feature; disturbances of sleep, appetite, and energy as associated symptoms; a duration of at least 1 month; and impairment in everyday functioning. Chronic and acute forms are not differentiated, and thus the definition can be regarded as similar to a combination of major depressive episode and dysthymia.
Over the years of the study, the vernacular for describing depressed mood has changed. The idiom of “being in poor spirits” was commonly used at the beginning of the study but declined in frequency. Idioms such as “feeling low and hopeless” and “wondering if anything is worthwhile” became more customary. The methods used for time trends have been adjusted for sensitivity to such changes
(21,
28).
The DPAX findings indicated that the current prevalence of depression in each year of study was about 5% (
Table 1). In 1992 a change in distribution was observed, occasioned by the fact that women younger than 45 years exhibited a twofold increase that was counterbalanced by small diminutions among older men and women
(21). The incidence of depression remained stable at approximately 4 per 1,000
(29).
Statistical Methods
Analysis of cross-sectional time trends used multivariate logistic regression in SAS PROC GENMOD
(30). For assessing trends in smoking, three analyses were conducted: the prevalence of heavy smoking, the prevalence of moderate smoking, and the prevalence of both levels combined. In each, the comparison group was subjects who did not smoke. Three predictor variables were used: age (<45 and ≥45), gender, and study year.
For analysis of trends in the relationships between smoking and depression, current depression was the outcome variable and four predictor variables were used: age, gender, study year (1952, 1970, and 1992), and current daily smoking (no cigarette smoking, moderate smoking, and heavy smoking).
Because we were especially interested in time trends, the main model tested included the interaction of smoking and study year. In addition, models were fitted that included all other pairwise interactions. To investigate possible higher-order interactions, the analysis was repeated, stratified by gender and then stratified by age.
Results of the logistic regression models are presented in terms of odds ratios with 95% confidence intervals. The odds ratios were adjusted so that, in each year of study, the reference category consisted of depressed nonsmokers.
Where the cohorts were concerned, standard life-table methods were used to calculate incidence rates for depression among subjects who were at risk for a first-ever depression
(29,
31). The effects of age, gender, smoking status at baseline, and cohort interval (1952–1970 compared with 1970–1992) were statistically assessed by using survival regressions implemented in log linear analysis
(32). In addition, the incidence of depression was related to the different patterns of tobacco use (continuing to be a nonsmoker as well as starting, continuing, or quitting smoking) over the time interval. Individuals who became depressed were compared with those who never had a depression by using relative risk with 95% confidence intervals.
Results
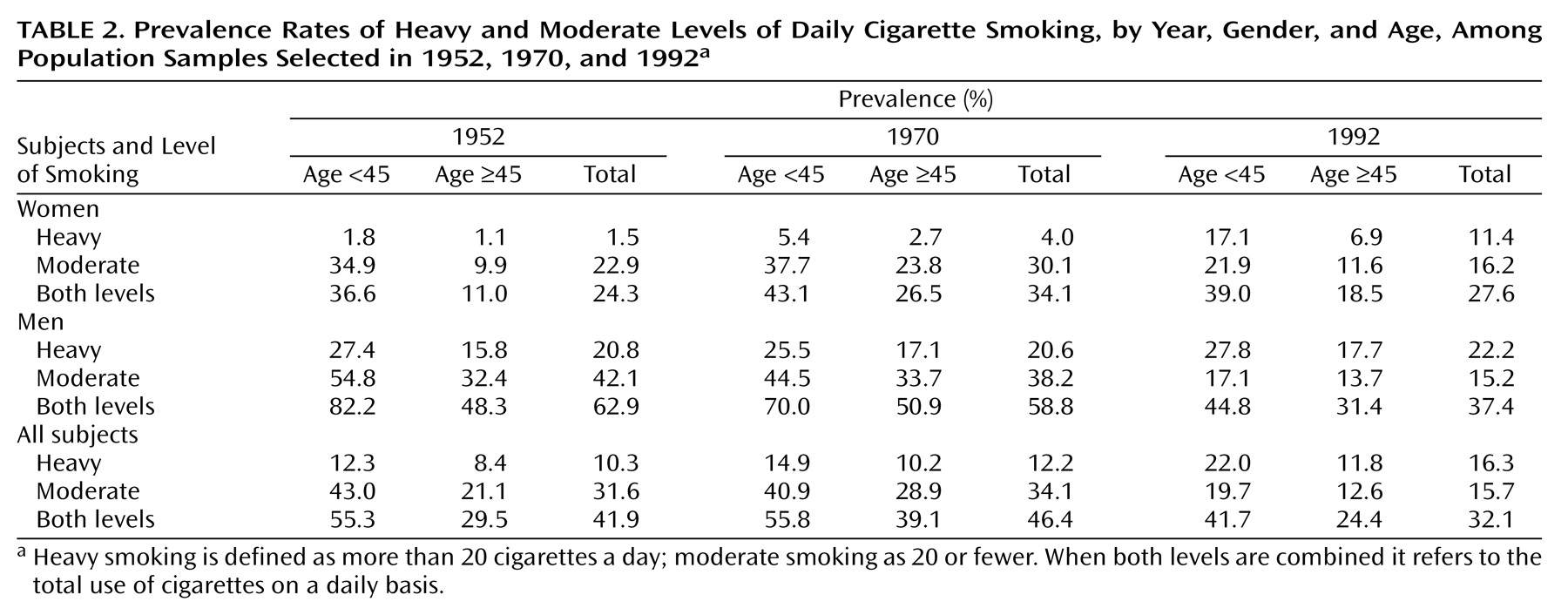
Our first analysis concerned population smoking trends.
Table 2 shows prevalence rates by year, gender, and age. Analysis of all those who smoked (combining both heavy and moderate levels) indicated that the main effects of year, gender, and age as well as the interactions with year and gender and with year and age were all significant at the level of p<0.0001. Smoking increased between 1952 and 1970 and decreased by 1992. Men were significantly more likely to smoke than women, but this difference attenuated over time. Similarly, more younger people smoked than older people, and this difference also reduced over time.
By 1992, moderate smoking had declined among both men and women. This was achieved by a sharp drop between 1970 and 1992 for men while the drop-off among women followed an increase. Men displayed a stable prevalence of heavy smoking at just over 20%, but heavy smoking increased among women (2% in 1952, 4% in 1970, and 11% in 1992). The increase of heavy smoking was somewhat more pronounced for younger women (2% in 1952, 5% in 1970, and 17% in 1992).
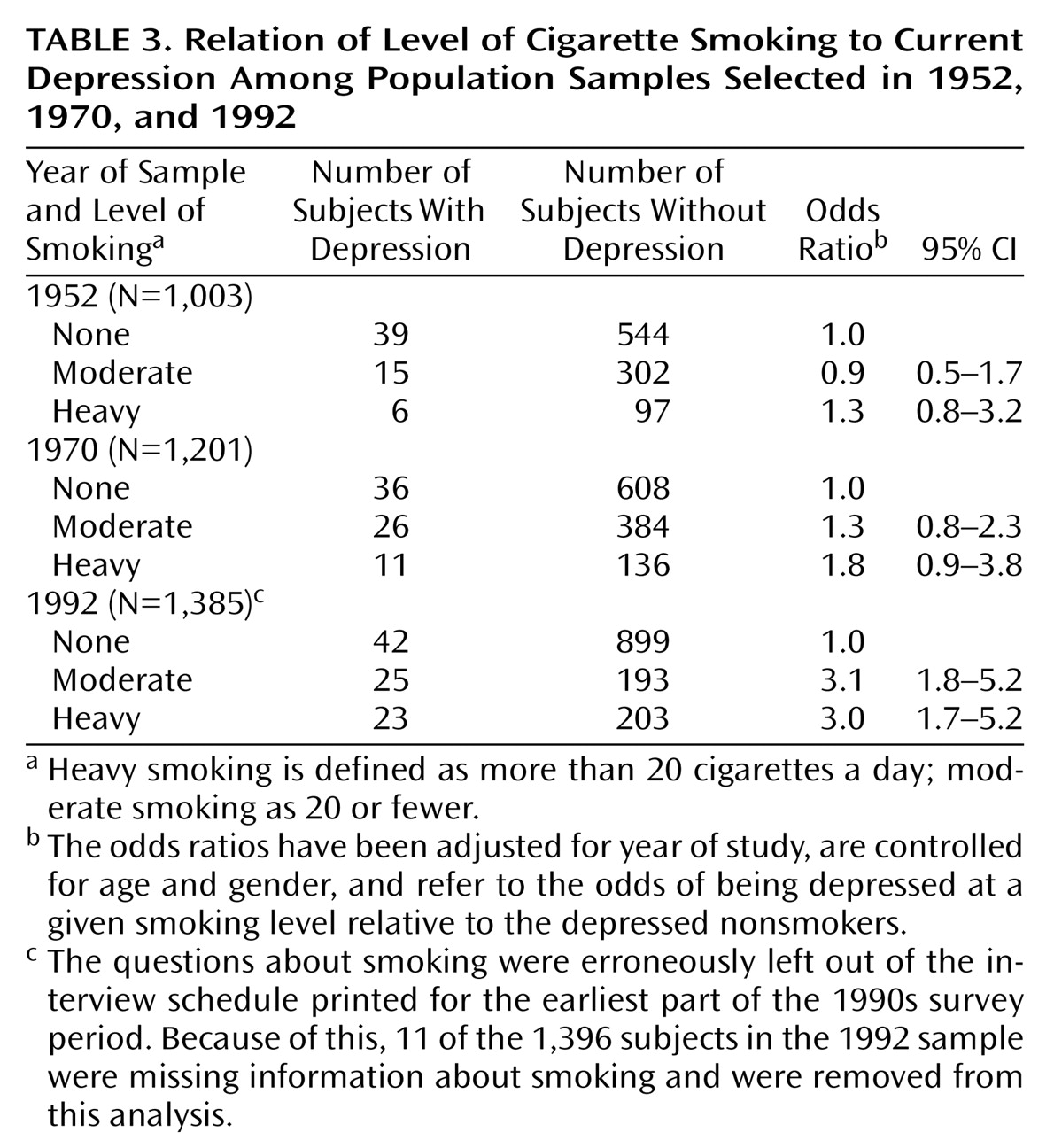
In regard to the associations between depression and smoking in the three samples, logistic regression indicated that smoking and study year exhibited a significant interaction (χ
2=10.2, df=4, p=0.04). The other pairwise interactions were not significant and were not used in the estimation of odds ratios. In 1952 and 1970, the associations between depression and smoking were not significant, but in 1992 they were strong and significant.
Table 3 shows that in the most recent sample the odds that a smoker would be depressed were three times the odds that a nonsmoker would be depressed. When stratified by age, the results were similar. When stratified by gender, the analysis suggested that the association had been present in 1970 for men but not at so strong a level as in 1992.
For individuals followed over time, we investigated the general patterns of change and stability in smoking. Because smoking was more common among younger subjects and because the prevalence of smoking declined after 1970, many subjects who were smoking at the beginning of the intervals were not smoking at the end. Such cessation increased over time (33% of the smokers in cohort 1 and 54% of the smokers in cohort 2 quit). Concomitantly, only a few of these adults started smoking, and this proportion decreased over time from 10% in cohort 1 to 4% in cohort 2. The patterns of starting and stopping tended to be similar for men and women, but older people were more likely to quit and less likely to start than younger people.
With regard to studying whether depression preceded smoking as might be disclosed by following individuals, we were unable to test whether depression at baseline predicted subsequent initiation of smoking. This was because smoking was so common in 1952 and 1970 that the cohorts were nearly halved when limited to those at risk and because so few adults started smoking that in cohort 1 there were only two depressed subjects who later became smokers and in cohort 2 none did so.
With regard to studying whether smoking preceded depression, we found that smoking at baseline was not related to the subsequent incidence of depression. In cohort 1 the average annual incidence of depression among smokers was 4.5 per 1,000; among nonsmokers it was 4.6 per 1,000. In cohort 2, comparable figures were 3.8 and 3.5.
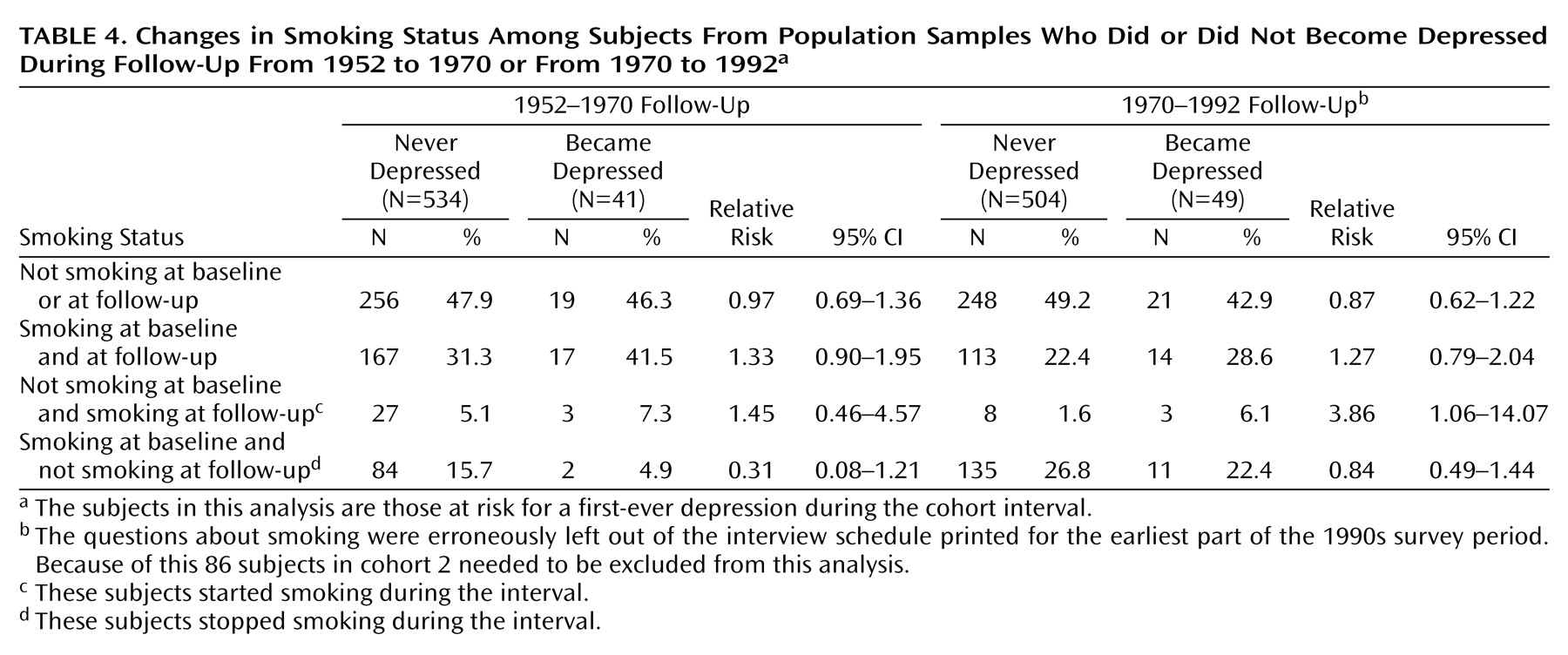
Given the historical trend toward smoking cessation, it was possible that some of the subjects who became depressed had already quit smoking before the onset of depression. This possibility led us to use information about all types of changes and continuities in smoking practices. We found that subjects who became depressed were more likely to begin or continue smoking and less likely to quit than those who never became depressed (
Table 4). Although the associations were modest, the same general pattern pertained in both cohorts. In cohort 2, subjects who became depressed were nearly four times more likely to start smoking at some point in the interval than those who were never depressed.
Discussion
This investigation began when cigarette smoking was very common and increasing, and it extended through the period when tobacco use was declining. The samples of 1952 and 1970 were studied before evidence began to appear in the psychiatric literature indicating an association between having a psychiatric disorder and using nicotine. The main finding from this study is that a significant association between depression and smoking did not appear until 1992, when the most recent sample was selected.
It was only when smoking was becoming nonnormative that a strong and positive association with depression appeared. Studies of other forms of substance use and abuse have suggested that there may be a relationship between the commonness of use and the degree to which it is associated with deviance or psychopathology
(33,
34). For example, fewer drug use problems seem to occur in inner cities where heroin is commonly used, and more alcohol use problems may be found in cultural areas where abstemiousness is the norm
(33). Although such illustrations point up cross-sectional differences by geographic locales, there is also some evidence about changing relationships over time. For example, as cocaine use has become more widespread its association with affective disorder appears to have declined
(34). Where tobacco use is concerned, our finding about the emergence of a strong association with depression when cigarette smoking was becoming less prevalent can be compared to evidence of a stronger relationship between smoking and the psychopathology of nicotine dependence in recent than in early birth cohorts
(17).
Following cohorts of individuals over time is a useful way to investigate whether depression tends to precede smoking or smoking to precede depression. Our analysis of “depression first and smoking later” was hampered by the fact that quitting was much more common than starting to smoke. Where “smoking first and depression later” was concerned, our evidence was negative. Given the trend toward cessation, however, it is possible that subjects who became depressed had already quit smoking.
Given these factors, our main finding about what happened over time among individuals comes from using all patterns of smoking change and continuity. This finding indicates that subjects who became depressed were more likely to continue smoking, to initiate smoking, and not to quit than those who never became depressed. The finding also suggests that subjects who became depressed were more involved with nicotine than those who were never depressed.
The Stirling County Study has several strengths for addressing the topic of this report. Among them are time-depth and the combination of repeated cross-sectional surveys with cohort follow-up of individuals. In addition, the definition of depression is explicit and quite congruent with contemporary criteria. The measurement of time trends in depression has benefited from attention to consistency of methods while making adjustments for changes in the vernacular for expressing depressed mood.
A limitation is that the Stirling County Study concerns adults, but there is strong evidence that smoking begins among adolescents and that trends among them differ from the trends for adults
(35). There are also several features of smoking practices that it would have been useful to explore through each individual’s history, but the data are limited to behavior at the time of interview.
It is very likely that the general decline in smoking prevalence was related to the markedly increased public awareness of health hazards of smoking. Given the numerous warnings and prohibitions on smoking that have come into effect, it is probable that everyone was aware of the dangers by the 1990s. Because of this, the knowledge about the risks needs to be considered in interpreting the findings.
If the self-medication hypothesis is correct, it is plausible that the positive effect of nicotine in diminishing dysphoric feelings might have been so strong that depressed subjects would smoke in spite of knowledge about the negative effects. They would resist quitting and would be more likely to start or continue to use tobacco. Support for the self-medication hypothesis would be strengthened if a dose response were found. Although not clear-cut, our findings are not inconsistent with such a response; it was suggested in 1970 when the association was beginning to be observed, especially among men. Further, although the odds for moderate and heavy smoking were similar in 1992, they had quite wide confidence intervals.
Another possible mechanism relates to the fact that depression may incline its sufferers to take risks of many kinds because they feel that life is not worthwhile. Thus, awareness of the risks associated with smoking may not have reduced the incentive to smoke. It is notable that some other recent studies have indicated that depression is associated with many risky behaviors, including use of chemical substances and poor attention to health care
(15,
16).
The hypotheses about self-medication and risk-taking flow from the view that depression leads to smoking rather than that smoking leads to depression. In this study, we found no positive association between previous smoking and subsequent depression. Further, the evidence that subjects who became depressed were more involved with tobacco than those who had never been depressed seems to give greater weight to the view that there is something about depression inclining its sufferers to use tobacco than that there is something about smoking engendering depression.
It would seem unwise, nevertheless, to rule out the possibility that smoking might be among the antecedent factors associated with the development of depression. One reason for caution is that both depression and heavy smoking were found to have increased among younger women in the 1992 sample. Other studies have also pointed to increasing rates of depression and have suggested that the increase seems to have appeared among subjects born after World War II
(36,
37). All of the younger women in our 1992 sample had been born after that war
(21).
The fact that both heavy smoking and depression increased among this particular segment of the population raises questions about whether the social changes that have particularly affected women over the last half of the 20th century are relevant to the increase in depression. Over this period, acceptability for women to smoke went along with acceptability to work outside of the home, to use the pill, to drink, to divorce, and to compete with men in many spheres. The consequences of these changes were probably variable: some were advantageous and others created a climate that may have put larger numbers of women at risk for depression.
The smoking trends among men were different from those among women, and the association with depression started earlier for men. The fact that the associations between depression and smoking were general in 1992 rather than being limited to a particular segment of the population suggests that the relationships may be multifaceted and not easily reducible to just one or two main factors.
The portions of the Stirling County Study following individuals through time have thus far indicated that depression is an extremely grave disorder, carrying a risk of chronicity, progressive disability, and premature death
(38,
39). The adverse consequences of nicotine use are well-known. Compared with other drugs, cigarettes are the most persistently used
(40). When depression and smoking coexist, the quality and quantity of life are doubly assaulted.