Psychiatric Diagnosis
Only three patients fulfilled criteria for a mental disorder according to DSM-IV. Two had major depression and one had alcohol abuse before experiencing acute respiratory distress syndrome. Signs of an earlier posttraumatic stress syndrome (e.g., PTSD) could not be determined in any of the patients.
At the time of dismissal from the intensive care unit or hospital, 43.5% of the patients (20 of 46) had PTSD, according to the SCID, and 8.7% (four of 46) had sub-PTSD. At the time of the follow-up evaluation, i.e., an average of 8 years after intensive care, 23.9% (11 of 46) continued to suffer from full-blown PTSD, and 17.4% (eight of 46) had sub-PTSD. None of the patients who had shown posttraumatic symptoms at the time of dismissal developed delayed PTSD.
In the patients with PTSD, psychiatric comorbidity according to the SCID could be determined at follow-up: two with major depression, one with an eating disorder (bulimia), one with alcohol abuse, and 11 with undifferentiated somatoform disorder. In the patients with sub-PTSD (N=4) and without PTSD (N=1), there were five cases of undifferentiated somatoform disorder (Fisher’s exact test: χ2=27.11, df=1, p=0.0003).
Psychological Assessments
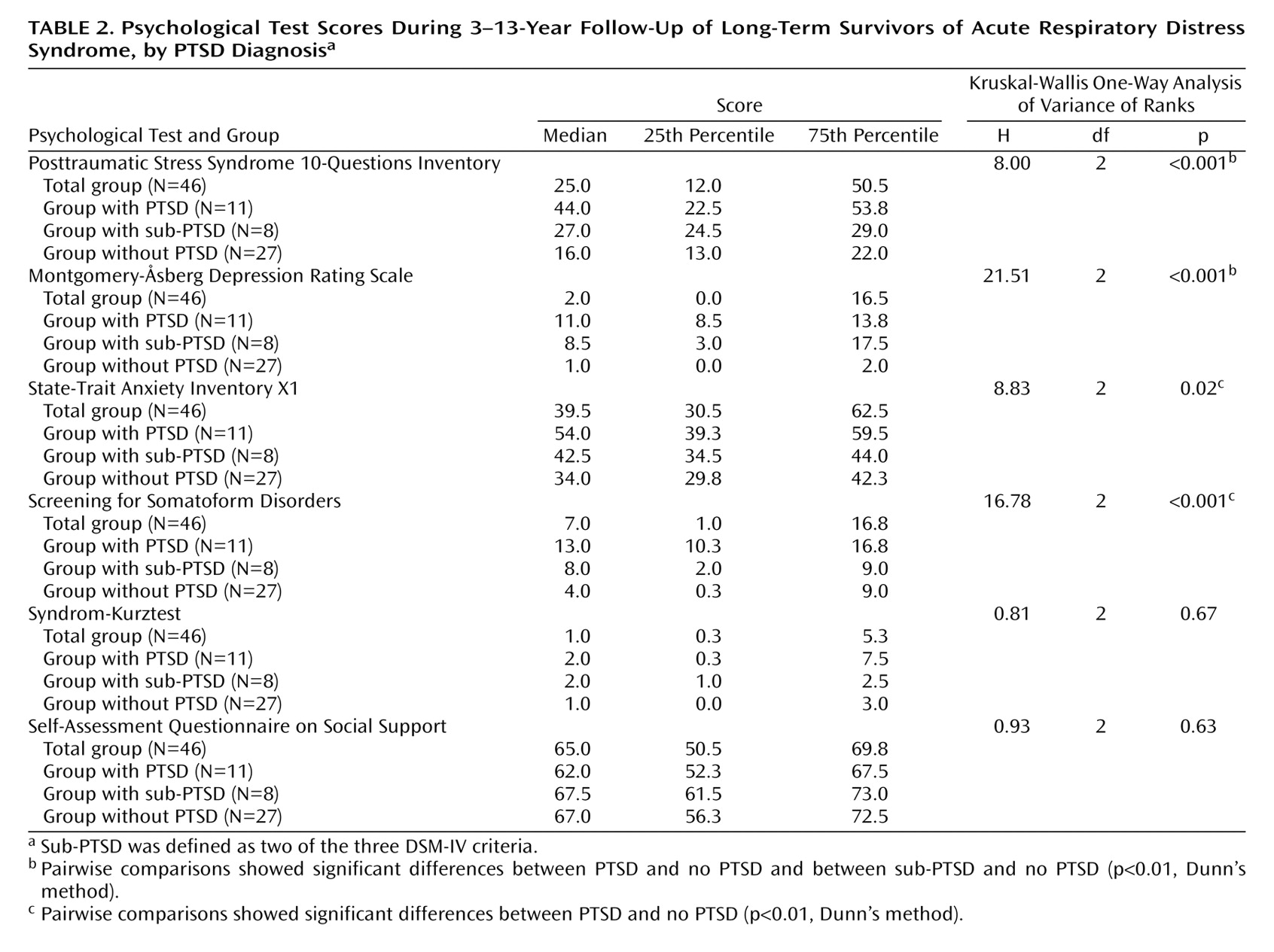
The results of the Posttraumatic Stress Syndrome 10-Questions Inventory self-questionnaire seemed to discriminate well with respect to the diagnostic status of PTSD, according to DSM-IV (Kruskal-Wallis H=18.00, df=2, p<0.001) (
Table 2). The scores of both the PTSD group and the sub-PTSD group were significantly different from those of the group without PTSD (p<0.01, Dunn’s method). The average Posttraumatic Stress Syndrome 10-Questions Inventory value of 44.0 in the PTSD group was well above the cutoff score of 35 reported in the literature.
Although the depression scores on the Montgomery-Åsberg Depression Rating Scale demonstrated statistically significant differences among the subgroups (PTSD, sub-PTSD, no PTSD), in terms of clinical relevance, however, they indicated only minor degrees of depressed mood. This was confirmed by the fact that, in addition, only two patients fulfilled the diagnostic criteria for depressive disorder.
There were statistically significant differences between the subgroups in respect to the amount of situational anxiety in the State-Trait Anxiety Inventory X1. The patients with PTSD significantly differed from the patients without PTSD (p<0.01, Dunn’s method). However, it should be noted that none of the patients fulfilled all of the criteria for an anxiety disorder according to DSM-IV.
The patients with a DSM-IV diagnosis of PTSD showed a marked tendency toward somatization. Their average score on the Screening for Somatoform Disorders was in the range that characterizes patients with somatoform disorders, according to the literature. There were significant differences between the groups. Only the pairwise comparison between the group with PTSD and the group without PTSD differed significantly (p<0.01, Dunn’s method).
There were no indications in any of the patient groups for relevant losses in cognitive function as evaluated by psychological tests. The average scores on the Syndrom-Kurztest fell well under the cutoff point of 5. However, four patients (two with PTSD, one with sub-PTSD, one with no PTSD) with respective scores of 7, 9, 11, and 16 demonstrated signs of a mild or moderately severe disturbance of cognitive functions. There were no statistically significant differences among the patient groups with respect to the degree of available social support.
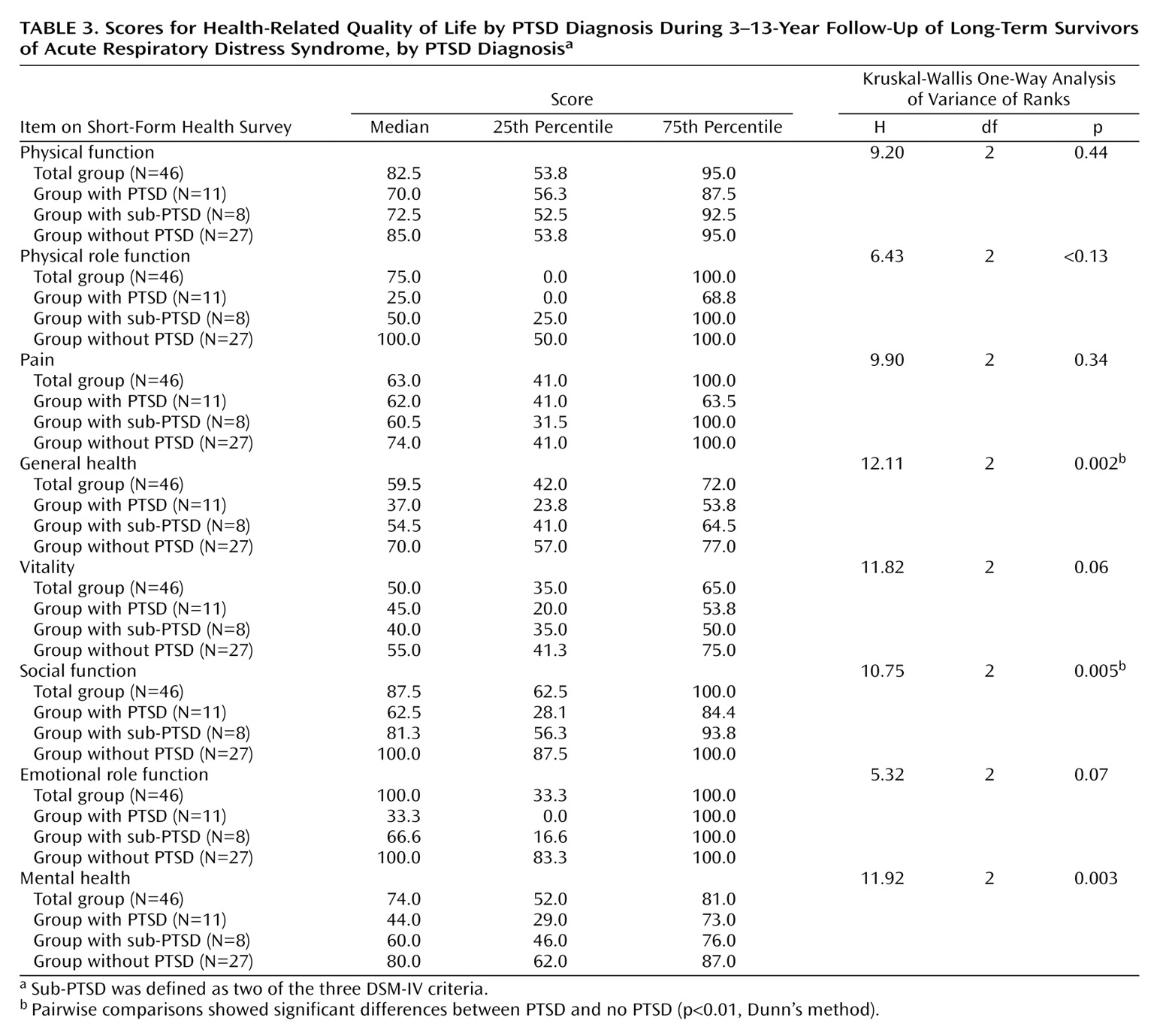
Patients with complete PTSD showed the most serious losses with respect to their health-related quality of life in the following Short-Form Health Survey dimensions (
Table 3): general health, social function, and mental health. The scores of the patients without PTSD were within the range for the general population
(18). All absolute scores from the patients with sub-PTSD were located near the median. However, only the paired comparison between the groups with PTSD and without PTSD demonstrated statistically significant differences (p<0.01, Dunn’s method).
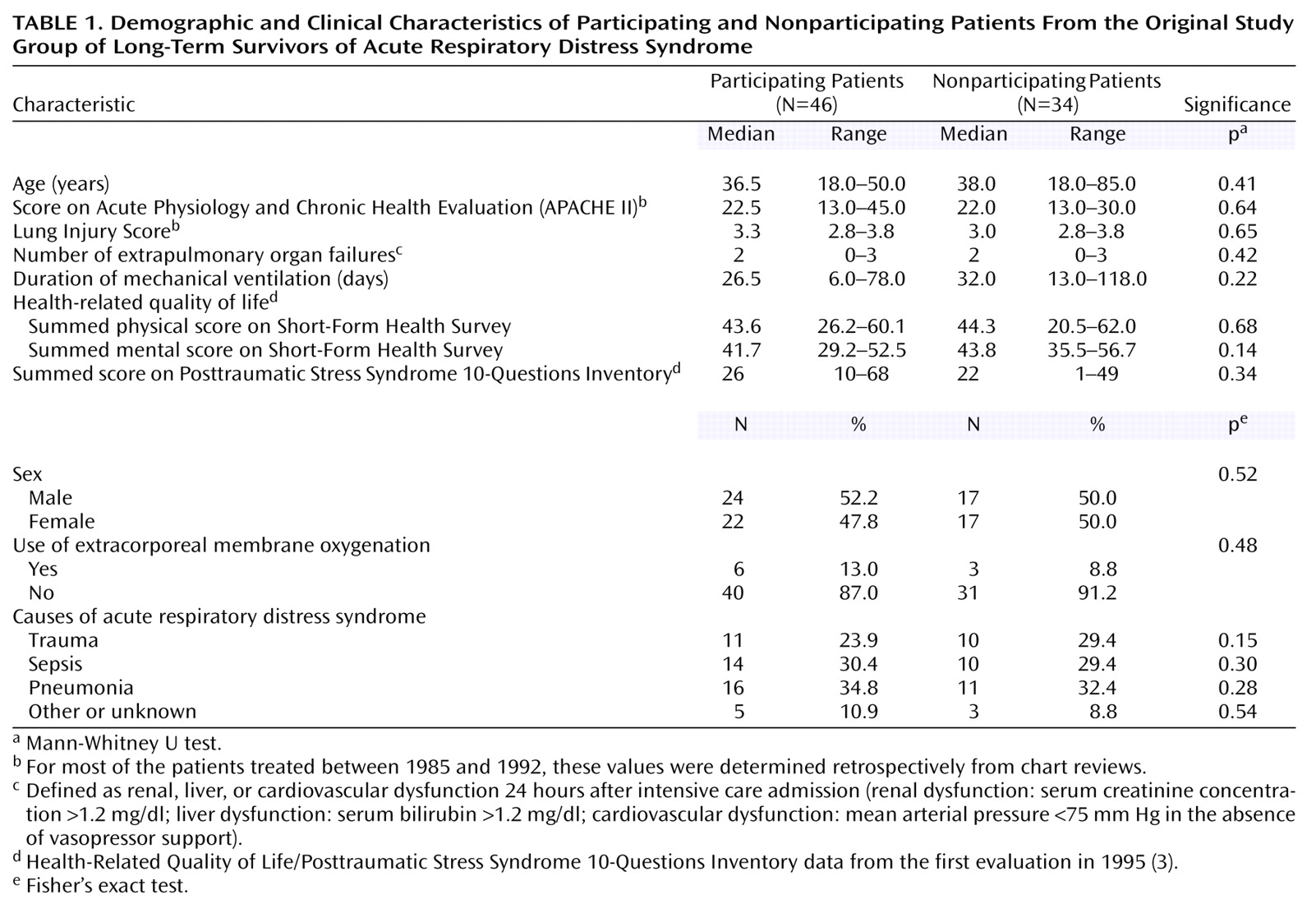
None of the variables (age, sex, sociodemographic or premorbid psychopathology) discriminated between the subgroups (PTSD, sub-PTSD, or no PTSD). With respect to the severity of the somatic disorder at the start of intensive medical care, neither the Acute Physiology and Chronic Health Evaluation (APACHE II)
(4) nor the Lung Injury Score
(4) discriminated between the subgroups. The duration of the stay in the intensive care unit correlated significantly with the risk for PTSD (patients with PTSD: median=70 days; patients with sub-PTSD: median=27.5 days; patients with no PTSD: median=27.5 days) (Kruskal-Wallis H=7.37, df=2, p<0.04).