Although epidemiological studies report a high prevalence of anxiety disorders in schizophrenia, their clinical relevance is still underrecognized. The presence of anxiety in schizophrenia patients has been associated with a greater risk of suicide
(1), poorer social functioning, and an increased risk of relapse
(2). Bayle et al.
(3) reported that 47.5% of schizophrenia patients had a lifetime history of panic attacks, that in 31.2% of cases the onset of panic disorder preceded the onset of schizophrenia, and that the treatment of panic disorder improved clinical and social outcome.
While comorbid panic
(3) and obsessive-compulsive disorder
(4) have been investigated in schizophrenia patients, social anxiety in schizophrenia has received much less clinical attention. In fact, comorbid anxiety disorders are reported in more than 50% of schizophrenia patients, and in epidemiological studies, the rate of social anxiety disorder ranges from 13% to 39%
(5–
8). In a 90-day follow-up study, Blanchard et al.
(2) found that social anxiety disorder in schizophrenia was a stable phenomenon across assessments. However, it often remains unrecognized and therefore untreated because of its frequent confusion with negative symptoms in schizophrenia patients. This psychopathological debate was first discussed 40 years ago by Meehl in both his original
(9) and revised
(10) theories. He pointed out that anhedonia, a core negative symptom, could contribute to or be a consequence of what he described as “aversive drift” in schizophrenia, i.e., the tendency to take on a burdensome, threatening, gloomy, negative emotional charge
(10). He suggested that this aversive drift is intense and pervasive in the interpersonal domain, manifesting itself as ambivalence and interpersonal fear
(9).
People with social anxiety suffer considerable impairment in daily life activities, occupational role, and social relationships
(11). Social anxiety is itself a disabling disorder, and individuals with social anxiety disorder as a comorbid condition have a more severe level of disability
(12). Subjects with social anxiety disorder have a higher risk of developing substance/alcohol abuse or dependence, and in patients with schizophrenia, as in the general population, substance abuse or dependence appears to be associated with higher impulsivity and suicidality
(13). Social anxiety disorder also contributes significantly to decreased quality of life in schizophrenia
(14). Therefore, the assessment and treatment of social anxiety disorder comorbidity in schizophrenia patients should improve both clinical and social outcomes.
Penn et al.
(15) described the phenomenon of social anxiety in schizophrenia through a role-playing assessment and proposed an instrument (the Ward Fear Scale) for social anxiety disorder in schizophrenia inpatients. To our knowledge, no attempt to assess social anxiety symptoms in schizophrenia outpatients has been made until now. We attempted to precisely define the assessment, clinical correlates, impact, and consequences of comorbid social anxiety disorder in schizophrenia. We studied a consecutively enrolled group of schizophrenia outpatients and a comparison group of patients with social anxiety disorder as their primary diagnosis. Our hypotheses were that schizophrenia patients with social anxiety disorder, compared with schizophrenia patients without social anxiety disorder, would have 1) a higher prevalence of other comorbid anxiety disorders, 2) a greater number of suicide attempts in their history and attempts of greater lethality, and 3) lower social adjustment and quality of life. Moreover, we hypothesized that the Liebowitz Social Anxiety Scale for social anxiety symptoms would reveal a similar profile for social anxiety disorder patients and schizophrenia patients with social anxiety disorder.
Method
Eighty outpatients diagnosed with schizophrenia according to the Structured Clinical Interview for DSM-IV and 27 outpatients with a current primary diagnosis of social anxiety disorder were recruited consecutively at the Institute of Neurosciences during the period between December 2000 and November 2002. All the schizophrenia subjects were recruited from the outpatient unit of the institute. During the recruitment period, six subjects with schizophrenia and one patient with social anxiety disorder refused to be interviewed and to enter the study. These subjects have not been considered in the statistical analyses. All the recruited patients, after providing written informed consent, were evaluated for clinical symptoms, demographics, social adjustment, and quality of life. At the time of evaluation, all schizophrenia patients were receiving antipsychotic treatment (clozapine: N=19; olanzapine: N=21; risperidone: N=18; quetiapine: N=14; typical neuroleptics: N=8). Forty-one of the schizophrenia patients were women, 39 were men. They ranged in age from 19 to 45 years (mean=29.0, SD=5.9). Fifteen of the social anxiety disorder patients were women, and 12 were men. They ranged in age from 18 to 56 years (mean=33.4, SD=7.8).
The schizophrenia and social anxiety disorder patients were interviewed with the Structured Clinical Interview for DSM-IV Axis I Disorders
(16) and the Liebowitz Social Anxiety Scale
(17). Schizophrenia patients were also assessed with the Scale for the Assessment of Positive Symptoms (SAPS)
(18), the Scale for the Assessment of Negative Symptoms (SANS)
(18), and the Social Adjustment Scale
(19).
Suicide behavior was explored during the clinical interview with the subjects by asking whether they had ever attempted suicide and, if so, how often. A suicide attempt was defined as a self-destructive act carried out with the intention of ending one’s life. Ratings were based not only on the patient’s report but also on all available sources of information, including case notes and interviews with relatives and case managers.
The number of lifetime suicide attempts was ascertained, and the lethality of the suicide attempt was scored from 1 to 4 according to the medical/psychiatric treatment chosen by the clinicians to resolve the episode: 1=discharge from the emergency department without treatment; 2=psychiatric treatment recommended after discharge from emergency department; 3=psychiatric admission; 4=medical admission, including admission to the intensive care unit.
Quality of life was assessed with the Medical Outcomes Study 36-item Short-Form Health Survey
(20), which includes eight multi-item scales. The physical functioning, role-physical, bodily pain, and general health scales contribute to the composite physical health summary measure, while the vitality, mental health, role-emotional, and social functioning scales contribute to the mental health summary score. The raw scores on the eight Short-Form Health Survey scales range from 0 (worst possible health status as measured by the questionnaire) to 100 (best possible health status). The summary measures are scored by using norm-based methods for the general Italian population
(21) and standardized to have a mean of 50 and a standard deviation of 10.
Social anxiety disorder patients were given the evaluations immediately before the beginning of treatment for their disorder.
The two patient groups were compared by analysis of variance (alpha=0.05) and chi-square analyses. Interrater reliability was verified by a series of independent interviews conducted by the authors (S.P. and L.Q.); reliability for both the Liebowitz Social Anxiety Scale and the Social Adjustment Scale achieved interclass correlation values ranging from 0.80 to 0.92.
Discussion
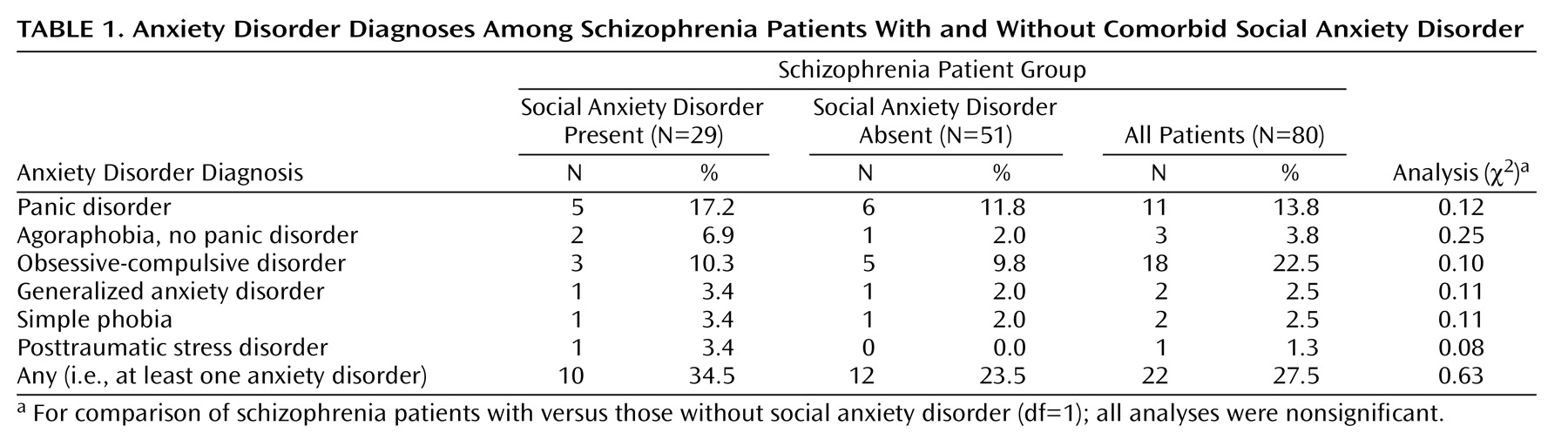
Consistent with other studies, we found that 36.3% of schizophrenia patients have a comorbid social anxiety disorder. Our findings also showed that in our group of schizophrenia patients receiving medical treatment, social anxiety disorder is by far the most common anxiety disorder. Cosoff and Hafner
(6) also found social anxiety disorder to be the most prevalent anxiety disorder in schizophrenia patients, but the rate that they found was about 17%. This difference of prevalence could be due to differences in subject recruitment: Cosoff and Hafner’s study was conducted in the open wards of an acute adult service, while all our subjects were in outpatient treatment.
To our knowledge, our study is the first to investigate social anxiety in outpatients with schizophrenia. All the schizophrenia subjects were recruited from the outpatient unit of the institute and were in a clinical remission or partial remission phase at the time of the assessment, as documented by the average low positive and negative symptom scale scores. It is noteworthy that social anxiety symptoms become evident when patients are in a phase free from schizophrenia symptoms; the former are a reflection of the patients’ greater efforts at social adaptation and increased expectations.
Our study was primarily a clinical and not an epidemiological investigation, and it involved clinical detection and assessment. This could enhance the accuracy of the assessment and could explain the prevalence of social anxiety disorder found in our group of schizophrenia patients.
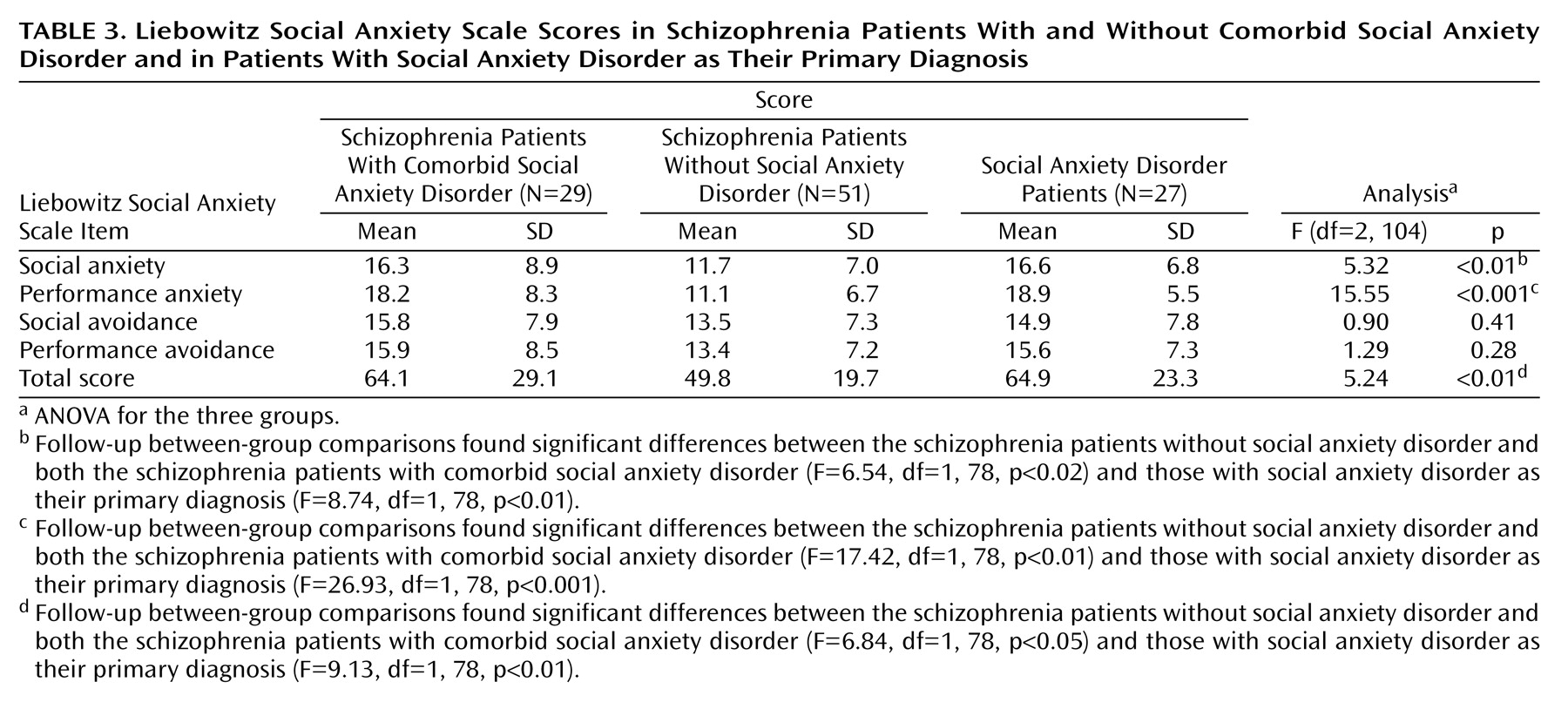
The use of the Liebowitz scale for assessment of social anxiety seems adequate and reliable. No differences were found on any single item score between schizophrenia patients with social anxiety disorder and patients with social anxiety disorder as a primary diagnosis. In other words, no differences resulted in social anxiety phenomenology when it appears as a primary diagnosis or when comorbid with schizophrenia. The Liebowitz Social Anxiety Scale could also reliably distinguish these groups from schizophrenia patients without comorbid social anxiety disorder. It seems that social anxiety in patients with schizophrenia, related or unrelated to treatment, has a similar clinical profile to that experienced by social anxiety disorder patients without schizophrenia. In any case, it seems that the Liebowitz Social Anxiety Scale can be regarded as a reliable instrument to assess social anxiety in schizophrenia outpatients, in a similar way to the scale devised by Penn et al.
(15) to measure social anxiety in inpatients.
In some preliminary assessments conducted with schizophrenia subjects before the beginning of the study, we found that the administration of the scale by a clinician ensures greater reliability than with self-administration. In particular, we found that the Liebowitz Social Anxiety Scale, SANS, and SAPS should be administered by the same clinician in order to avoid possible ambiguity between social anxiety symptoms and positive and negative symptoms. We observed a similar rate of positive and negative symptoms in both groups of schizophrenia patients, those with and without comorbid social anxiety disorder.
In the first attempt at a systematic study of social anxiety in schizophrenia, Penn et al.
(15) found that negative symptoms were related to observational ratings of anxiety during role playing, while positive symptoms were not. Undoubtedly, the experience of paranoia and the social withdrawal found in schizophrenia can mimic social anxiety disorder symptoms. Clinical attention needs to focus on the presence of anxiety symptoms associated with avoidance behavior and on the level of insight, both of which are reduced when negative symptoms are predominant in the clinical picture. In schizophrenia, withdrawal behavior linked to negative symptoms is phenomenologically sustained by detachment, while social anxiety is related to interpersonal sensitivity. On the basis of our observation, a patient typology profile of the following kind could emerge: good familiar adaptation; low positive and negative symptom scores; difficulties relating to specific key social situations like those investigated by the Liebowitz Social Anxiety Scale, i.e., not related to paranoid experience but to stress-elicited anxiety. Although the distinction between social anxiety disorder and negative/positive symptom-related behavior remains somewhat difficult, clinical experience shows that this clinical distinction is easier in schizophrenia patients than in patients with social anxiety disorder as their primary diagnosis.
One limitation of the investigation was that the social anxiety and the schizophrenia groups differed with regard to whether or not they were receiving medication at the time of assessment. May this have confounded the results in some way? It cannot be excluded that social anxiety in schizophrenia subjects could be related to treatment, in accordance with findings described by our group in a previous study of 12 schizophrenia subjects where social anxiety disorder was induced by clozapine treatment
(22,
23). It is also possible that antipsychotic treatments, particularly clozapine and olanzapine, contribute to make the prevalence of social anxiety disorder in our group higher than that reported by Cosoff and Hafner
(6).
Previous anamnestic examination of the clinical reasons why an atypical neuroleptic treatment was chosen for each single patient revealed that in no case was the choice based on the fact that the individual exhibited anxiety. However, in this study, the potential effect of treatment (1084 mg in chlorpromazine equivalents) and the association between atypical antipsychotics and social anxiety symptoms have still to be defined, since the therapy was chosen and not randomly assigned, and neuroleptic treatments with significant extrapyramidal side effects could contribute to confound the differential diagnosis between negative symptoms and social anxiety-related behaviors. Our results are in line with those of Stern et al.
(24), who found that social anxiety disorder symptoms are common, quite severe, and not correlated with psychotic symptom severity among schizophrenia outpatients. In our previous study of 12 schizophrenia subjects with social anxiety disorder induced by clozapine treatment
(22,
23), we also found that fluoxetine augmentation improved social anxiety symptoms but not negative and positive symptoms.
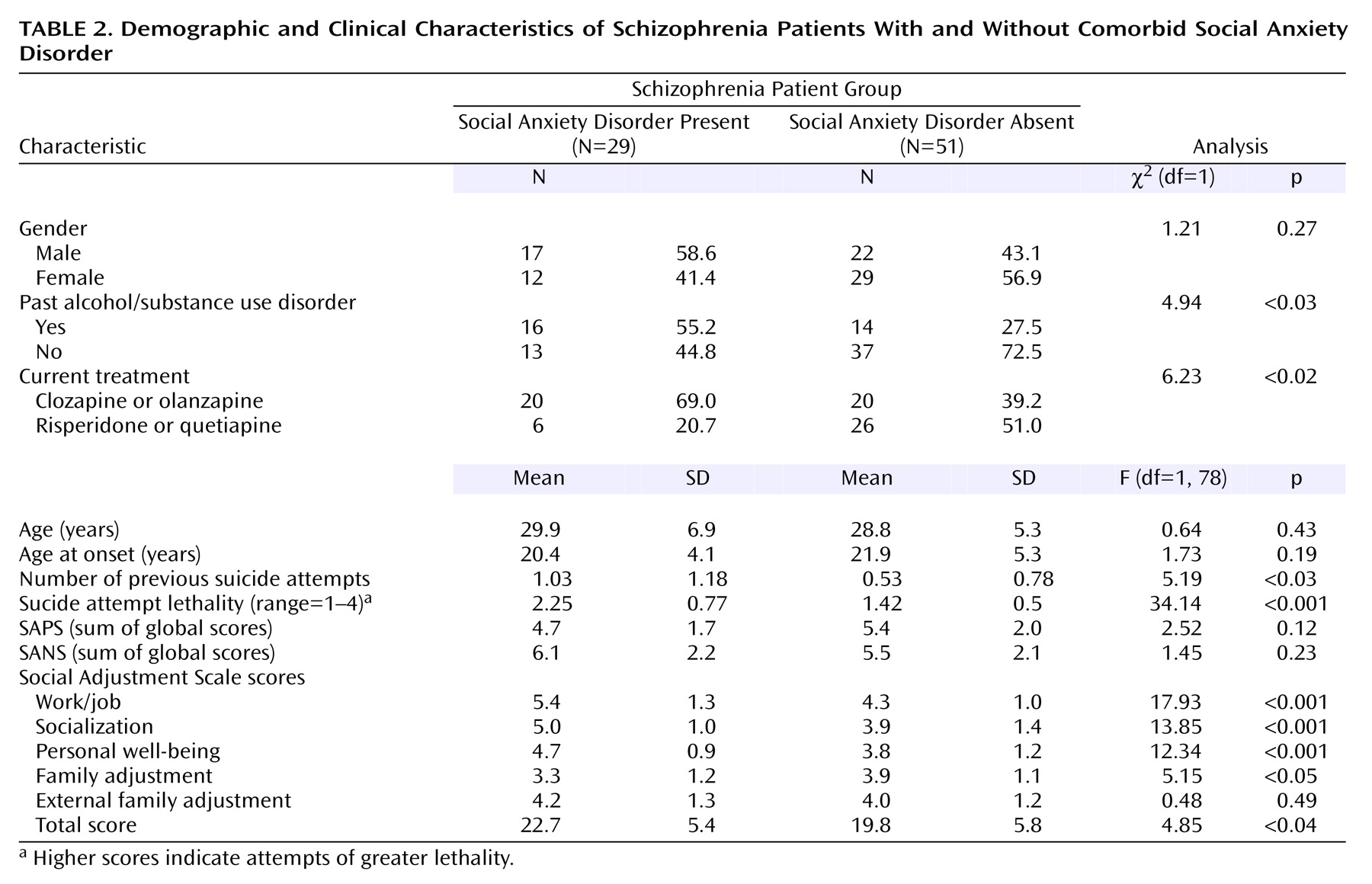
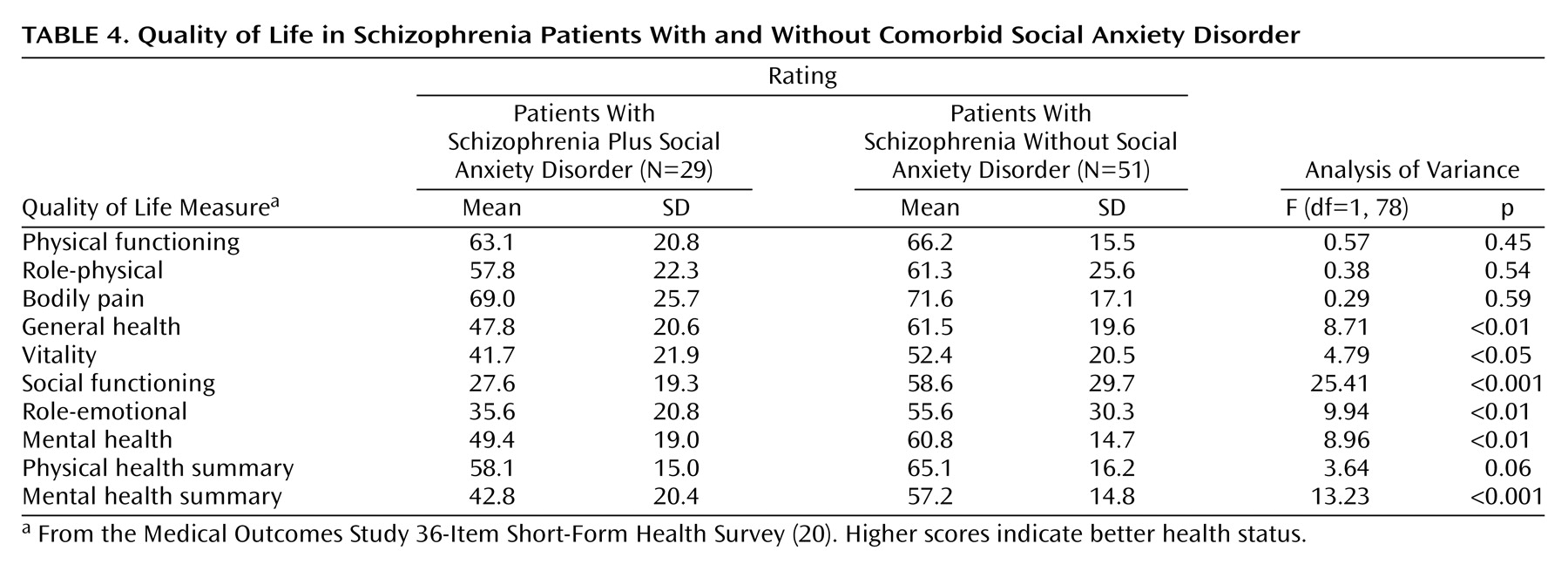
Schizophrenia subjects with comorbid social anxiety disorder showed indexes of lower social adjustment and lower quality of life compared with patients without social anxiety disorder. This was expected, taking into account that social anxiety, especially when present as a comorbid condition, causes substantial impairment in quality of life, lower work productivity and earnings, and greater utilization of health services
(25). The finding of a higher total number of suicide attempts and greater lethality of suicide attempts in patients with schizophrenia plus social anxiety disorder is also in line with the risk associated with social anxiety. Schneier et al.
(26) reported no increase in suicide risk among “uncomplicated social anxiety” (0.1%, N=11 of 9,953) and a higher rate among those with “complicated social anxiety” (15.7%, N=39 of 249). Katzelnick et al.
(25) found that suicide was attempted by 21.9% of subjects with noncomorbid generalized social anxiety disorder, a rate that is similar to that for current major depression. At the same time patients with schizophrenia plus social anxiety disorder had a higher rate of past alcohol or substance abuse/dependence.
In summary, social anxiety disorder is a common comorbid condition in schizophrenia, and it should be suspected in socially impaired subjects. Furthermore, its presence implies the need for both psychological and pharmacological therapeutic specificity and often a comprehensive treatment approach. Recently, Halperin et al.
(14) studied the efficacy of an 8-week, group-based cognitive behavior therapy for social anxiety in subjects with schizophrenia; they found clinically significant improvements in quality of life, social anxiety, and social phobia symptoms in the majority of treated patients. On the other hand, atypical neuroleptic treatments may accentuate the risk of the emergence of disorders like social anxiety (but also obsessive-compulsive disorder and panic symptoms); particular care is therefore required, especially when prescribing compounds like clozapine or olanzapine to schizophrenia patients.
If these observations are confirmed by further studies in larger samples, adequate next-step treatments will need to be sought. Currently there are no operational guidelines for the treatment of comorbid social anxiety disorder in schizophrenia. Fluoxetine augmentation of neuroleptic treatment has been shown to be effective in a previous study by our group
(23), but trials in larger samples are needed. No data are available for other possible options for schizophrenia patients with social anxiety disorder, such as a dose reduction in atypical neuroleptic treatment or the switch to another neuroleptic compound. At the same time, psychological intervention has been indicated as a possible effective strategy in a study on 20 subjects
(14). This observation needs to be confirmed.