Neuroimaging and electrophysiological studies have found evidence that panic disorder is associated with lower than normal activation of the left parietal or superior temporal cortex and relatively greater activation of the right than of the left frontal or hippocampal regions
(1–
3). Although few studies have examined regional brain activation in social phobia, enhanced activation of the right frontal-temporal regions was found in the EEGs of patients with social phobia during provocation of fear or anxiety
(4). Greater activation of the amygdala has been found in social phobia, but there is conflicting evidence about whether this activation involves primarily the right or left amygdala
(5,
6).
Given the high rate of comorbidity of anxiety and depressive disorders
(7), an important issue is the extent to which these abnormalities of regional hemispheric activation are specific to anxiety disorders or reflect the presence of comorbidity with depression. In a study measuring EEG in a resting state
(8), patients with comorbidity of an anxiety disorder and major depressive disorder showed greater activity in the right than in the left hemisphere over frontal and more posterior sites. In contrast, patients with major depressive disorder alone showed less activity over the right than over the left posterior sites, and neither they nor the healthy comparison subjects in that study had asymmetry of activity in frontal sites.
Studies using behavioral laterality tests have found evidence of left hemisphere dysfunction
(9,
10) or bias favoring right hemisphere processing
(11,
12) in subjects with anxiety disorders or high levels of trait anxiety. We have used dichotic listening tests to examine lateralized cognitive processing in patients with comorbid anxiety and depressive disorders
(13). In dichotic tests, paired stimuli (two different words or two different tones) are simultaneously presented to the two ears, and the difference in perceiving the stimulus in the right and left ear provides an index of perceptual asymmetry. On the Fused Rhymed Words Test
(14), healthy adults are more likely to perceive the word in the right ear, i.e., to show a right-ear advantage, which reflects the dominance of contralateral left hemisphere regions for language-related processing. In contrast, the Complex Tone Test
(15) yields a left-ear advantage in healthy adults that is indicative of right hemisphere dominance for processing of tonal stimuli. In our prior study, patients with comorbidity of an anxiety disorder and major depressive disorder differed from patients with major depressive disorder alone in having less left hemisphere advantage for fused words and a greater right hemisphere advantage for complex tones
(13). It is not, however, clear whether this evidence of left hemisphere dysfunction or bias toward right hemispheric processing is associated with having an anxiety disorder or with comorbidity of anxiety and depressive disorders. Our prior study was limited by the lack of patients with an anxiety disorder alone and by inclusion of a heterogeneous mix of patients with different anxiety disorders.
The present study was designed to overcome these limitations by assessing dichotic listening measures of lateralized cognitive processing in groups of patients with social phobia alone, with a depressive disorder alone, or with comorbidity of social phobia and a depressive disorder. On the basis of prior findings, we predicted that patients with social phobia either with or without a comorbid depressive disorder would show a smaller left hemisphere advantage for fused words and a greater right hemisphere advantage for complex tones, compared to subjects without social phobia, i.e., patients with a depressive disorder alone and healthy comparison subjects. Moreover, the dichotic listening tests yield separate measures of accuracy for perceiving syllables or complex tones in each ear. Given the predominance of contralateral projections from ear to auditory cortex, these absolute accuracy measures provide additional information concerning the source of differences in perceptual asymmetry between groups. Thus, left hemisphere dysfunction in subjects with social phobia would be expected to result in poorer right-ear accuracy for perceiving syllables in that group, compared to subjects without social phobia, whereas right hemisphere hyperactivation would result in increased left-ear accuracy for perceiving complex tones in subjects with social phobia, compared to subjects without social phobia.
Results
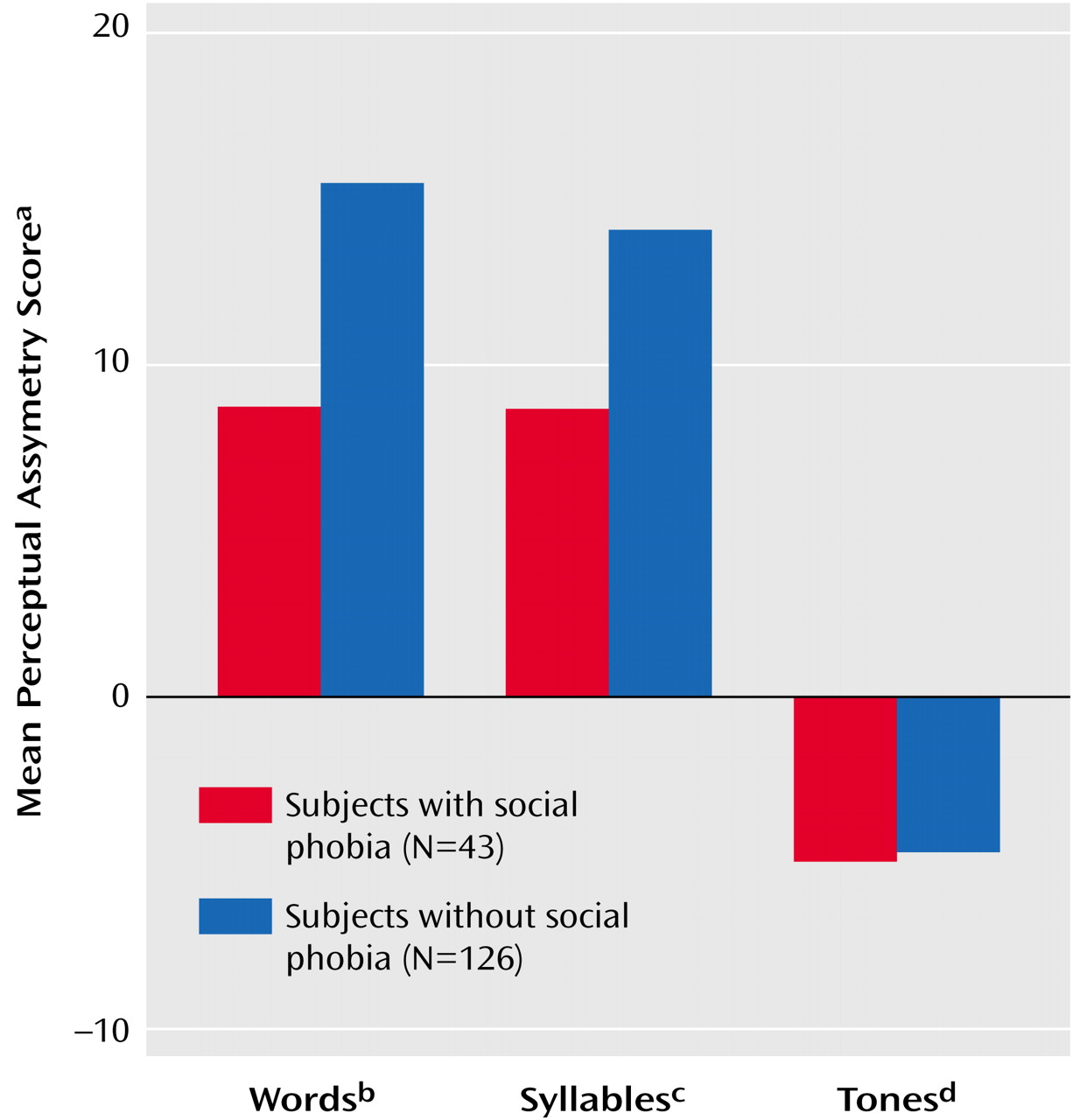
An ANOVA confirmed the expected difference in perceptual asymmetry across tests (F=66.94, df=2, 322, p<0.001), with the word and syllable tests yielding a left hemisphere advantage (i.e., positive asymmetry scores) and the tonal test yielding a right hemisphere advantage (i.e., negative asymmetry scores). The ANOVA revealed a significant main effect for social phobia (F=8.04, df=1, 161, p=0.005), which reflects the generally smaller left hemisphere advantage for words or syllables in subjects with social phobia (i.e., subjects with social phobia alone and those with comorbid social phobia and depressive disorder), compared to subjects without social phobia (i.e., those with depression alone and the healthy comparison subjects). Most important, a significant social phobia-by-test interaction was found (F=4.06, df=2, 322, p<0.05), indicating that the difference in perceptual asymmetry between the subjects with versus without social phobia was dependent on the test. This interaction is illustrated in
Figure 1, which shows the mean perceptual asymmetry scores on the word, syllable, and tone tests for subjects with versus without social phobia. A separate analysis of asymmetry scores on each test yielded a main effect of social phobia for both the fused-words test (F=7.33, df=1, 161, p<0.01) and the syllable test (F=6.82, df=1, 161, p=0.01), with a smaller left hemisphere advantage in patients with social phobia. In contrast, there was no significant difference among groups in right hemisphere advantage for complex tones. The difference in perceptual asymmetry between subjects with versus without social phobia was not modulated by the presence of a depressive disorder or by gender, as indicated by the absence of significant interactions of social phobia with these factors.
These findings were based on a design in which social phobia (present/absent) and depressive disorder (present/absent) were treated as independent variables. An alternative, less powerful, statistical design would treat the four groups as a single independent variable. Using this design, there were significant differences among groups in left hemisphere advantage for words (F=4.22, df=3, 161, p<0.01) and syllables (F=2.85, df=3, 161, p<0.05) but no difference in right hemisphere advantage for tones (F=1.36, df=3, 161, n.s.). For words, Newman-Keuls post hoc tests revealed a significant difference in left hemisphere advantage between the patients with social phobia alone and those with depression alone (p<0.05) but not between the groups in the remaining comparisons. Nor did the post hoc comparisons for the syllable test achieve statistical significance.
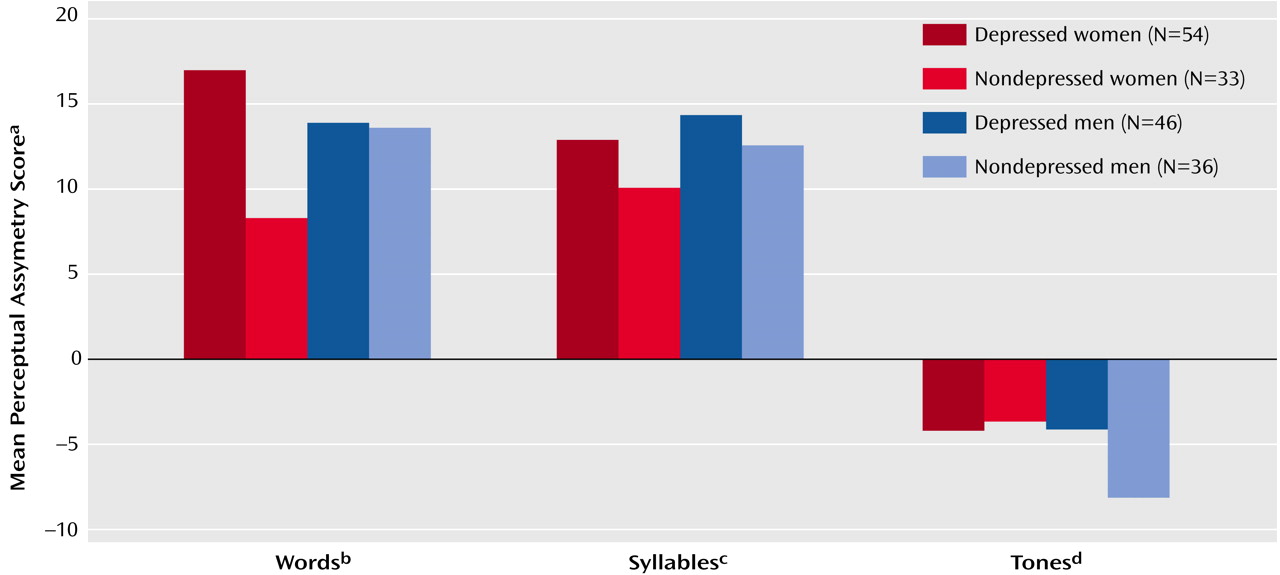
The only significant effect of depression in the ANOVA of asymmetry scores for the three dichotic tests was a depression-by-test-by-gender interaction (F=4.66, df=1, 322, p<0.05). The nature of that interaction is illustrated in
Figure 2, which shows the mean perceptual asymmetry scores for women and men with versus without a depressive disorder. Depressed women had a markedly larger left hemisphere advantage for words, compared to nondepressed women (t=2.88, df=85, p=0.005), but this difference was not evident for men, which was reflected in a depression-by-gender interaction in the ANOVA of the asymmetry scores for this test (F=4.64, df=1, 161, p<0.05). A similar depression-by-gender interaction was present in the ANOVA of the asymmetry scores for the syllable test (F=3.98, df=1, 161, p<0.05) but not for the tone test. However, in a result that approached significance, depressed men had a smaller right hemisphere advantage for tones, compared to nondepressed men (t=1.82, df=80, p=0.07). This difference was not evident for women.
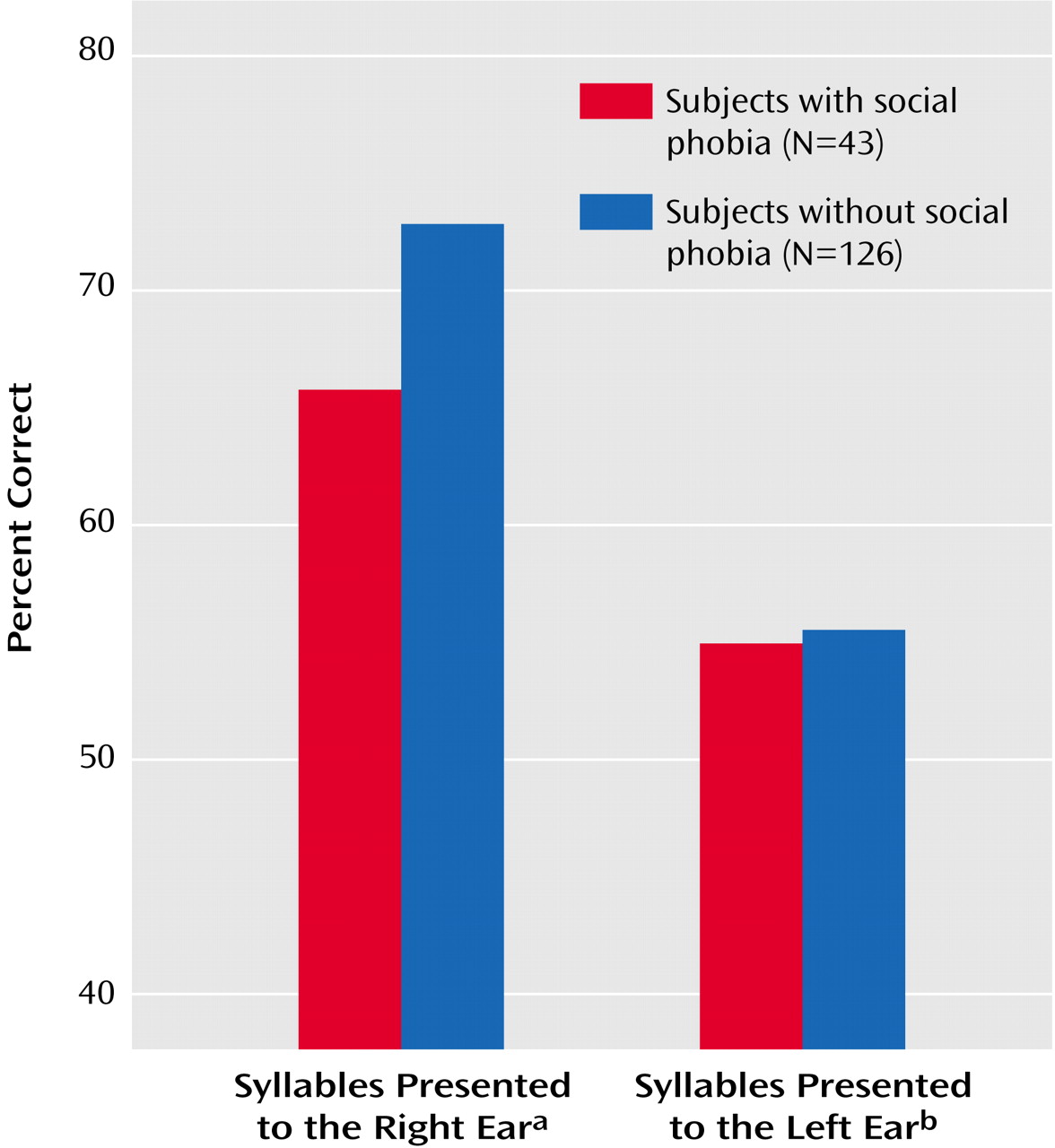
The syllable and complex tone tests also permit analyses of the absolute accuracy scores for each ear. These analyses provide important information about whether the smaller left hemisphere advantage for syllables in social phobia was due to poorer performance for items presented to the right ear or better left ear performance. An ANOVA of the accuracy scores for the syllable test yielded a significant interaction of social phobia and ear (F=6.97, df=1, 161, p<0.01).
Figure 3 shows the mean percentage of correct responses for subjects with versus without social phobia for syllables presented to the right or left ear. The smaller left hemisphere advantage for patients with social phobia was clearly due to their poorer right ear performance. Separate analyses of the accuracy scores for each ear revealed that subjects with social phobia had significantly poorer right ear accuracy, compared to subjects without social phobia (F=11.00, df=1, 161, p=0.001). In contrast, there was no significant difference between subjects with versus without social phobia in accuracy for perceiving syllables presented to the left ear. ANOVA of the accuracy scores for the complex tones test did not reveal any significant group difference for tones presented to the right or the left ear.
Correlational analyses examined whether the smaller left hemisphere advantage for words and syllables in social phobia was related to self-ratings of state anxiety on the State-Trait Anxiety Inventory. Perceptual asymmetry scores for words were not significantly associated with state-anxiety scores for the patients with social phobia either with or without a comorbid depressive disorder (r=0.001, df=42, n.s.), the patients with a depressive disorder alone (r=0.03, df=79, n.s.), or the comparison subjects (r=–0.02, df=43, n.s.). The only significant correlation between perceptual asymmetry for syllables and state-anxiety scores was seen for the comparison subjects (r=0.35, df=43, p<0.05), with greater state anxiety being associated with a larger left hemisphere advantage. When partial correlations were computed with the scores on the Beck Depression Inventory controlled, the correlations between perceptual asymmetry and state-anxiety scores remained essentially the same as those reported earlier.
Discussion
Patients with social phobia had a smaller left hemisphere advantage for perceiving dichotic words or consonant-vowel syllables, compared with subjects without social phobia. Their poorer accuracy for perceiving syllables in the right ear, compared to that for subjects without social phobia, as well as the absence of a group difference in perceptual asymmetry for complex tones, supports the hypothesis that social phobia is associated with dysfunction of left hemisphere regions mediating verbal processing. This finding is consistent with evidence that anxiety disorders are in general associated with left hemisphere dysfunction on behavioral laterality tests
(9,
10) and with lower than normal metabolism or cerebral blood flow in left temporoparietal regions
(1,
2) that are thought to mediate phonetic processing of dichotic words or syllables
(23,
24).
The reduced left hemisphere processing of verbal stimuli in social phobia is not specific to this disorder but has been found for obsessive-compulsive disorder
(10) and schizophrenia
(24,
25). Patients with comorbid anxiety and depressive disorders have also shown a smaller left hemisphere advantage for dichotic fused words, compared to those with a depressive disorder alone
(13). The findings of the present study support the conclusion that the smaller left hemisphere advantage in the patients with comorbid disorders was primarily due to the presence of an anxiety disorder.
Although the patients with social phobia showed less left hemisphere processing of verbal stimuli than the subjects without social phobia, they did not show the predicted enhancement of right hemisphere advantage for processing complex tones. In our prior study
(13), patients with comorbid anxiety and depressive disorders showed a greater right hemisphere advantage for perceiving complex tones, compared to depressed patients without an anxiety disorder and healthy comparison subjects. However, this difference was not due to better left-ear accuracy but to poorer right-ear accuracy. Given the predominantly contralateral projections from ear to auditory cortex, this finding is more suggestive of left hemisphere dysfunction than of right hemisphere hyperactivation. Patients with social phobia in the present study had poorer right-ear accuracy for perceiving consonant-vowel syllables, compared to subjects without social phobia, which is again supportive of the hypothesis of left hemisphere dysfunction in anxiety disorders.
One could argue that the smaller left hemisphere advantage for verbal processing in social phobia is due to greater performance anxiety during the tests in those patients. Previous research has found evidence that aversive arousal can reduce the left hemisphere advantage for dichotic consonant-vowels
(26). Although the lack of a correlation of state-anxiety and perceptual asymmetry scores provides no support for the effects of state anxiety on dichotic listening in patients with social phobia, self-ratings on the State-Trait Anxiety Inventory may not provide an accurate measure of performance anxiety during the dichotic tests. A study comparing dichotic listening performance of patients with social phobia before treatment and after clinical remission is needed to further examine the state-versus-trait issue.
Given the importance of verbal processing in social situations, the deficit in left hemispheric processing of verbal input in social phobia may be intrinsic to the disorder and may contribute to the stress and compound the anxiety experienced by patients with social phobia in these situations. Reports that persons with social phobia have difficulty taking in information when they are anxious and self-conscious could reflect reduced verbal processing resources. Cognitive behavior therapy techniques that enhance shifting patients’ focus of attention from self to the social situation
(27) may help patients allocate additional resources to improve processing of verbal input.
Adults and adolescents with a depressive disorder without an anxiety disorder have been found to show an abnormally large left hemisphere advantage for dichotic fused words
(13,
28). In the present study, depressed women had a larger left hemisphere advantage for words, compared to nondepressed women, but this difference was not seen among men. Depressed women had about twice the left hemisphere advantage, compared to nondepressed women. The enhanced left hemisphere advantage in depressed women is opposite the direction of the perceptual asymmetry seen in social phobia, and gender did not modulate perceptual asymmetry in social phobia. These findings underscore the importance of taking comorbidity and gender into account in studies of hemispheric asymmetry of function in depressive disorders.
A limitation of this study was the reliance on dichotic listening tests that provide only indirect measures of lateralized hemispheric function. The findings are, however, consistent with neuroimaging
(1,
2) and electrophysiological
(29) evidence of left temporoparietal hypoactivation in anxiety disorders. Further studies using neuroimaging and electrophysiological measures are needed to better understand the basis for the left-lateralized deficit in verbal processing in social phobia.