The prognostic significance of panic attacks has been a topic of renewed interest in recent years. Research efforts to examine the predictive strength of panic attacks with regard to psychopathology have included numerous studies that have documented associations between panic attacks and higher than expected rates of comorbid mental disorders
(1–
21). This evidence comes mainly from two sources. First, data from clinical samples have shown consistent links between panic attacks and the range of mental disorders
(17–
21). Second, epidemiologic studies have shown that panic attacks are common and highly comorbid among adults with depressive
(9,
10,
14–16), bipolar
(2,
14), anxiety
(7,
8,
11,
12,
14), substance use
(6), and psychotic disorders
(4,
5).
Although evidence cumulatively suggests a link between panic attacks and the range of mental disorders, there are several methodological features of previous research that limit the generalizability of these findings. First, previous studies have included adults, therefore these findings may not apply to adolescents or young adults. Second, studies to date have used cross-sectional designs. Third, previous studies from both clinical and epidemiologic samples have suggested that panic attacks are associated with a range of mental disorders, yet prior investigations have not measured the relationship between panic attacks and the severity of psychopathology in the community.
The goal of the current study was to address these questions by examining: 1) the relation between panic attack and mental disorders across the diagnostic spectrum among young persons and 2) the association between panic attack during adolescence and the risk of specific mental disorders and severity of psychopathology at follow-up during young adulthood by using prospective assessment of panic attacks and mental disorders within an epidemiologic study design. On the basis of previous findings among adults in the community
(5–
8), it was hypothesized that a history of panic attack would be associated with higher risk of mental disorders across the diagnostic spectrum. We also predicted that panic attack would be associated with severe psychopathology, reflected by multimorbidity, compared to a lack of panic attacks, among young adults in the community, based on previous evidence of the extensive comorbidity and psychosocial morbidity associated with panic attacks among adults
(12–
22).
Discussion
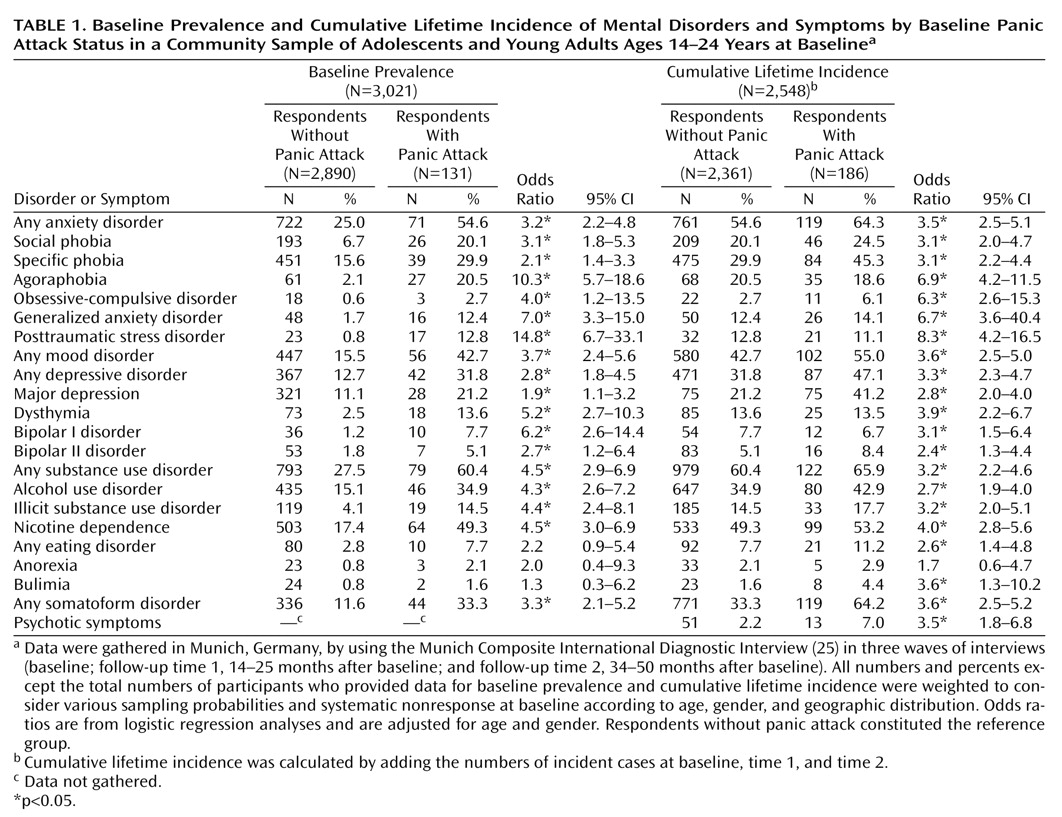
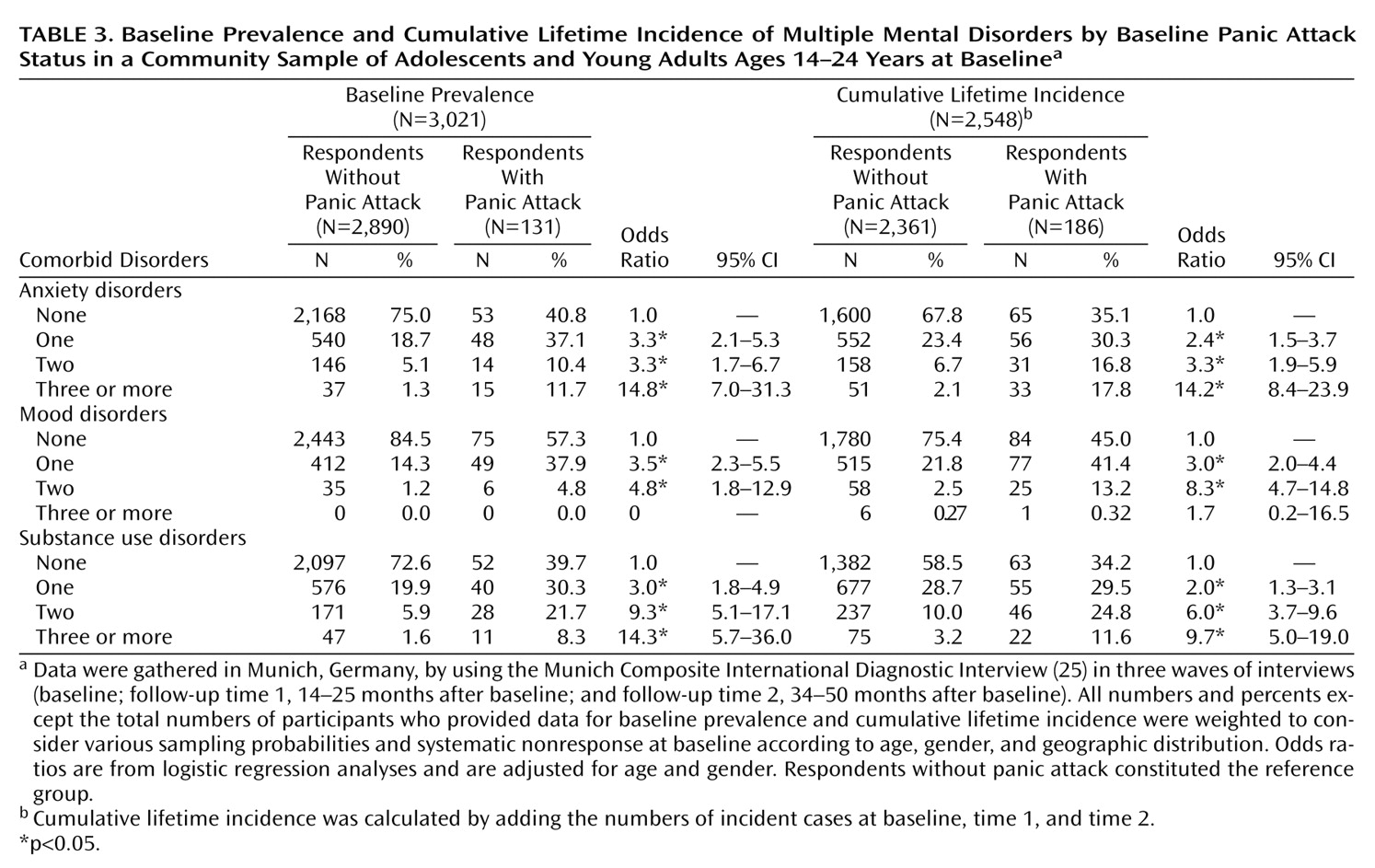
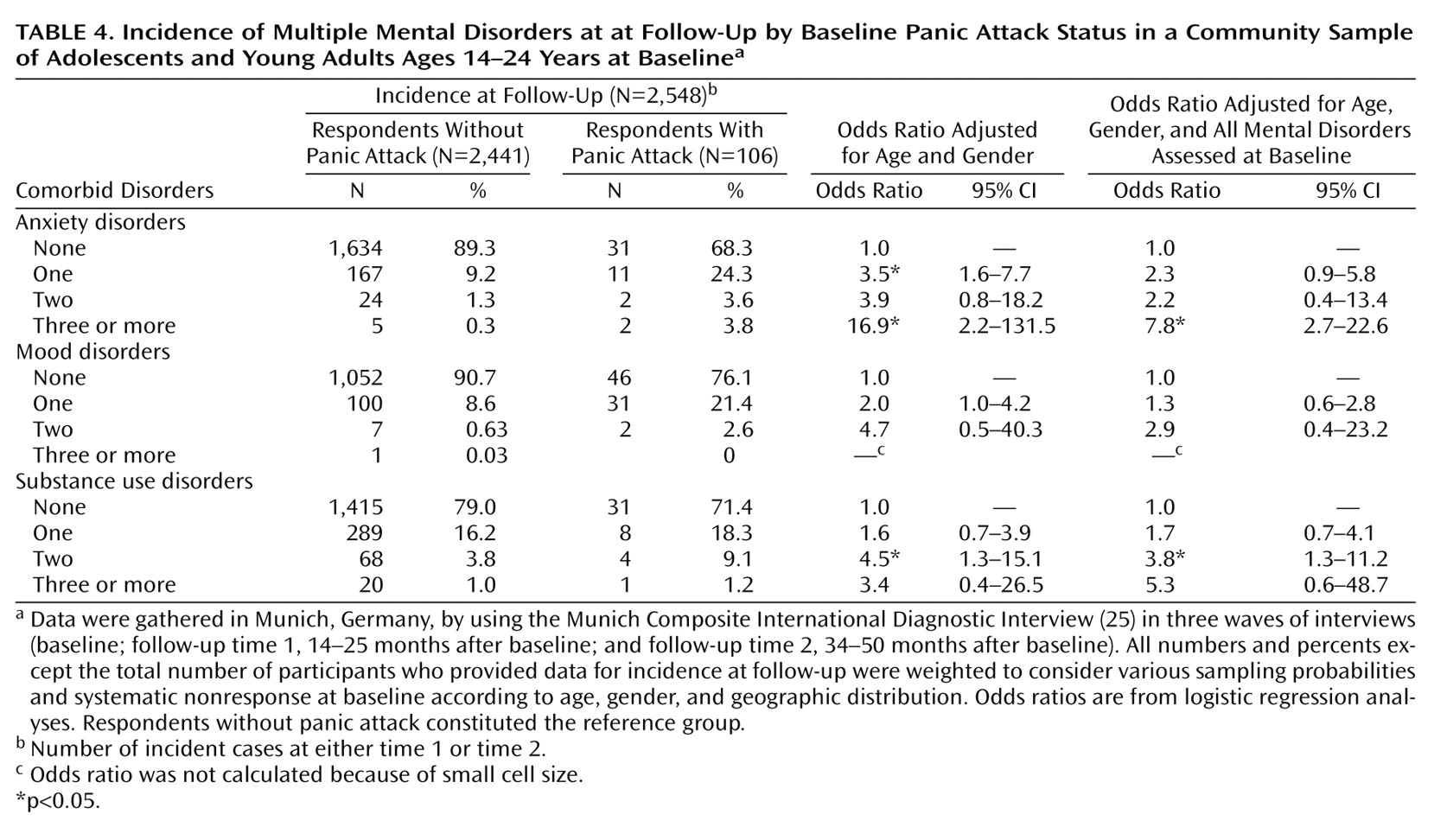
These data are consistent with and extend prior research with adults by showing that panic attacks are associated with high levels of comorbidity and multimorbidity across the diagnostic spectrum among adolescents and young adults in the community. Further, these results suggest that beyond the associations with panic disorder and agoraphobia, panic attacks are associated with increased risk of the onset of anxiety disorders (specifically generalized anxiety disorder, social phobia, and specific phobia), affective disorders, and substance use disorders, especially alcohol use disorders, by young adulthood. The findings also indicate that the majority of respondents who report panic attacks have at least one comorbid mental disorder during adolescence and that by young adulthood, more than one-half of those with panic attacks have multiple mental disorders, which is a significantly higher percentage than was found among their peers without panic attacks.
These data provide initial evidence suggesting that the high rates of comorbid mental disorders among adults with panic attacks are already evident among younger persons with panic attacks. The data suggest that while panic attacks in themselves are not considered a disorder or a condition that requires treatment (DSM-IV), more than one-half of those with panic attacks have at least one full-blown anxiety, mood, or substance use disorder, which may be relevant from both a clinical and public health perspective.
The type of associations as well as the strength of associations between panic attacks and comorbid mental disorders and multiple morbidity appeared fairly unique to panic attacks, despite the fact that there is a consistent association between having one mental disorder and a higher risk of comorbidity for all mental disorders. The results of our additional analyses for other mental disorders (e.g., major depression, eating disorders, specific phobia) also demonstrated higher rates of comorbidity; however, these associations were not consistent across the range of mental disorders nor were they associated with multiple mental disorders, in contrast to the consistent associations between panic attacks and the range of mental disorders. Therefore, the results appear consistent with previous data in finding a higher risk of comorbidity but provide new information regarding the strength, persistence, and comprehensiveness of panic attack as a factor associated with greater risk of the range of mental disorders.
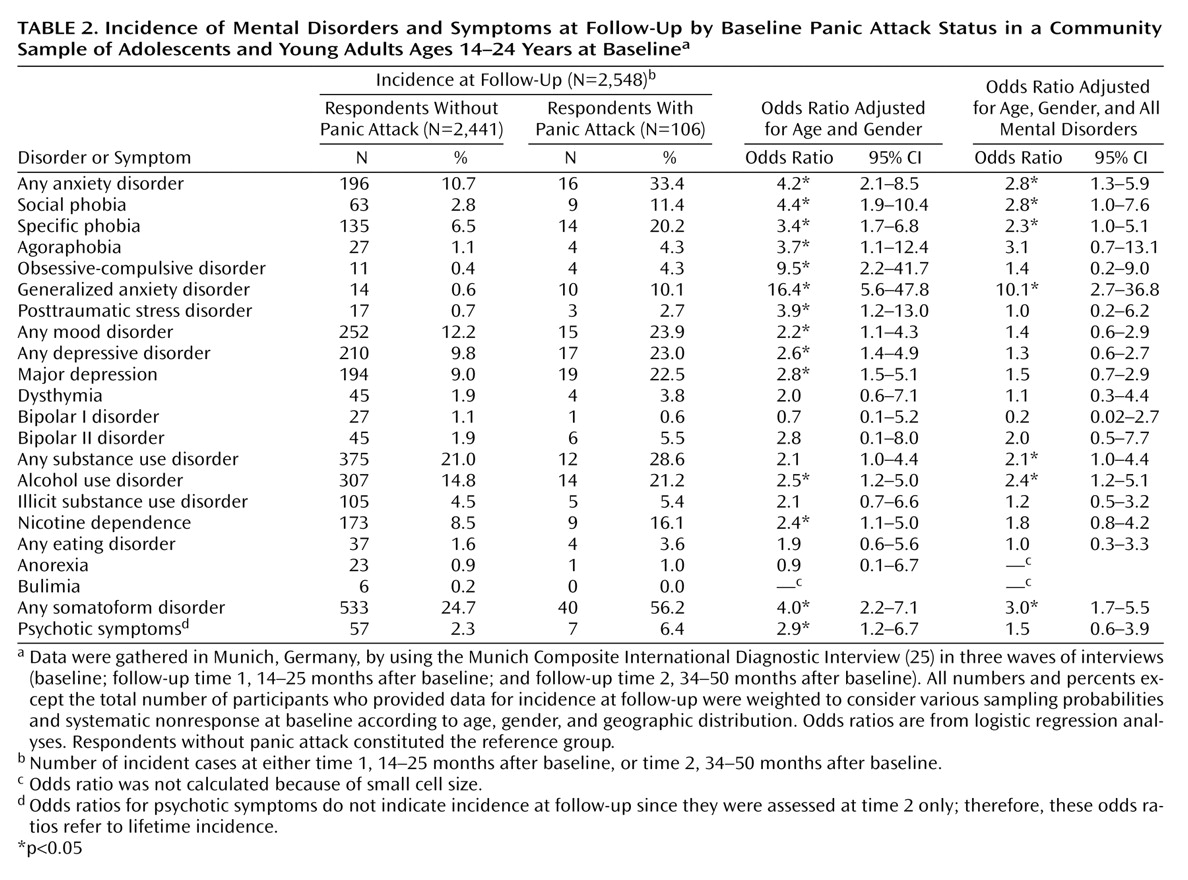
Our second set of analyses revealed that panic attacks are independently associated with a higher risk of the onset of anxiety and substance use disorders among young persons. The associations between panic attacks and the risk of phobias (i.e., specific phobia, social phobia) and generalized anxiety disorder remained statistically significant, albeit in an attenuated fashion after adjustment for comorbidity. In contrast, the observed relationship between panic attacks and the risk of OCD, PTSD, and major depression were no longer evident after adjustment. One possible explanation is that this clustering of disorders reflects a distinction in the nature of the underlying etiologic mechanisms between panic attacks and the onset of each mental disorder by young adulthood. For instance, it may be that there are genetic links between panic attacks and alcohol use disorders, a hypothesis that is consistent with family study results
(32,
33), while the relationship between panic attacks and PTSD may be mediated by comorbid mental disorders or stressful life events, rather than through a direct link. We found that a significantly greater percentage (22.5%) of those with panic attacks developed major depression by early adulthood, compared with those without panic attacks (9.0%), and this finding is consistent with results from cross-sectional studies among adults
(9,
10,
16). Yet, when we adjusted this association for the presence of comorbid disorders at baseline, it was not statistically significant. It may be that the younger age of this sample did not allow for enough time in the period of highest risk for onset of depression for this link to become observable, leading to small cell size. It could also be that the link is entirely due to comorbidity, although studies in adults have found a significant association, even after adjustment for the range of psychopathology
(6,
9,
14,
15). It is also conceivable that the relationship between panic attacks and risk of depression is more strongly related to age or differentially related to age, compared with the associations between panic attacks and anxiety and substance use disorders, in light of the contrast between our findings and those from adult samples. In an attempt to determine whether there was one specific comorbid disorder that accounted for this decrease in the strength of each link (i.e., whether the relationship between panic attacks and major depression was not due solely to comorbidity with alcohol dependence but was the result of a small contribution to the relationship made by each comorbid disorder), we fitted additional logistic regressions and included each comorbid disorder in a separate model. The results of these analyses suggested that each comorbid disorder made a small contribution to this link and that no one specific disorder could be identified as accounting for these patterns. This result was consistent across disorders.
Future studies that use longitudinal data to investigate more closely the mechanisms of these relationships may lead to a more in-depth understanding of the possible etiologic links underlying each of these associations. It is interesting to note that the observed relationship between panic attacks and psychotic symptoms is consistent with and contributes to growing evidence from clinical and epidemiologic studies of an association between panic and various forms of psychosis
(4,
5,
34). Unfortunately, psychosis was not evaluated at the baseline assessment of the Early Developmental Stages of Psychopathology Study, so calculation of risk of psychosis associated with panic attacks was not possible.
The limitations of this study should be noted. Small cell size because of low prevalence of less common disorders may have limited our ability to detect significant effects (e.g., for bipolar disorder). Our findings were obtained in a sample of 14–24-year-olds living in Munich, a metropolitan area with a population that has a relatively high quality of life and high socioeconomic status. Thus, direct comparisons with other age groups and areas characterized by other sociodemographics must be made with caution. That the period of high risk for onset of mental disorders had not fully passed at the time of the final assessment suggests that these estimates may underestimate lifetime risks.
Despite these limitations, the current study confirms previous findings of linkages between panic attacks and the range of mental disorders seen cross-sectionally among adults
(9,
12–
15,
20) and extends these associations to adolescents and young adults. Use of prospective methods to examine the relationship between panic attacks and the onset of the range of mental disorders in young adulthood in this study provides preliminary evidence of links between panic attacks and greater risk of onset of anxiety and substance use disorders during young adulthood. Finally, these data suggest that panic attacks are associated with severe psychopathology (defined as the presence of multiple mental disorders), with a majority of young persons with panic attacks meeting diagnostic criteria for at least three comorbid mental disorders by young adulthood. Future studies that replicate and examine each association observed in this study in greater depth across time will be useful in untangling the observed links and in exploring the potential utility of preventive interventions among those at risk. Investigation of the predictors for panic attacks, including family, genetic, social, and environmental risk factors, is needed.