Data from both epidemiologic and clinical samples indicate elevated rates of anxiety disorders among patients with bipolar disorder
(1–
7). Comorbid anxiety disorders have been reported at rates of 10.6%–62.5% for panic disorder, 7.8%–47.2% for social anxiety disorder, 3.2%–35% for obsessive-compulsive disorder (OCD), 7%–38.8% for posttraumatic stress disorder (PTSD), and 7%–32% for generalized anxiety disorder. The clinical significance of comorbid anxiety has been less well delineated, though greater severity and dysfunction are suggested. High levels of anxiety symptoms have been associated with greater suicidality, substance abuse, and lower lithium responsivity
(5,
8). Emerging data support a detrimental role for panic attacks, anxiety, and panic spectrum symptoms on bipolar disorder outcome
(9,
10).
In this article, we provide a comprehensive perspective on the correlates of comorbid anxiety in the largest well-characterized sample of bipolar disorder patients published to date. We extend previous findings by examining specific current and lifetime anxiety disorders and their link to measures of bipolar severity, suicide attempts, and functional impairment in 475 patients. We also examine bipolar I and bipolar II subtypes, delineate the impact of anxiety from substance use disorders, and separately examine the impact of comorbid anxiety in different phases of bipolar disorder. We hypothesized that comorbid anxiety would be associated with markers of greater bipolar disorder severity and that the correlates of comorbid anxiety would exist independently from those of substance use disorders.
Results
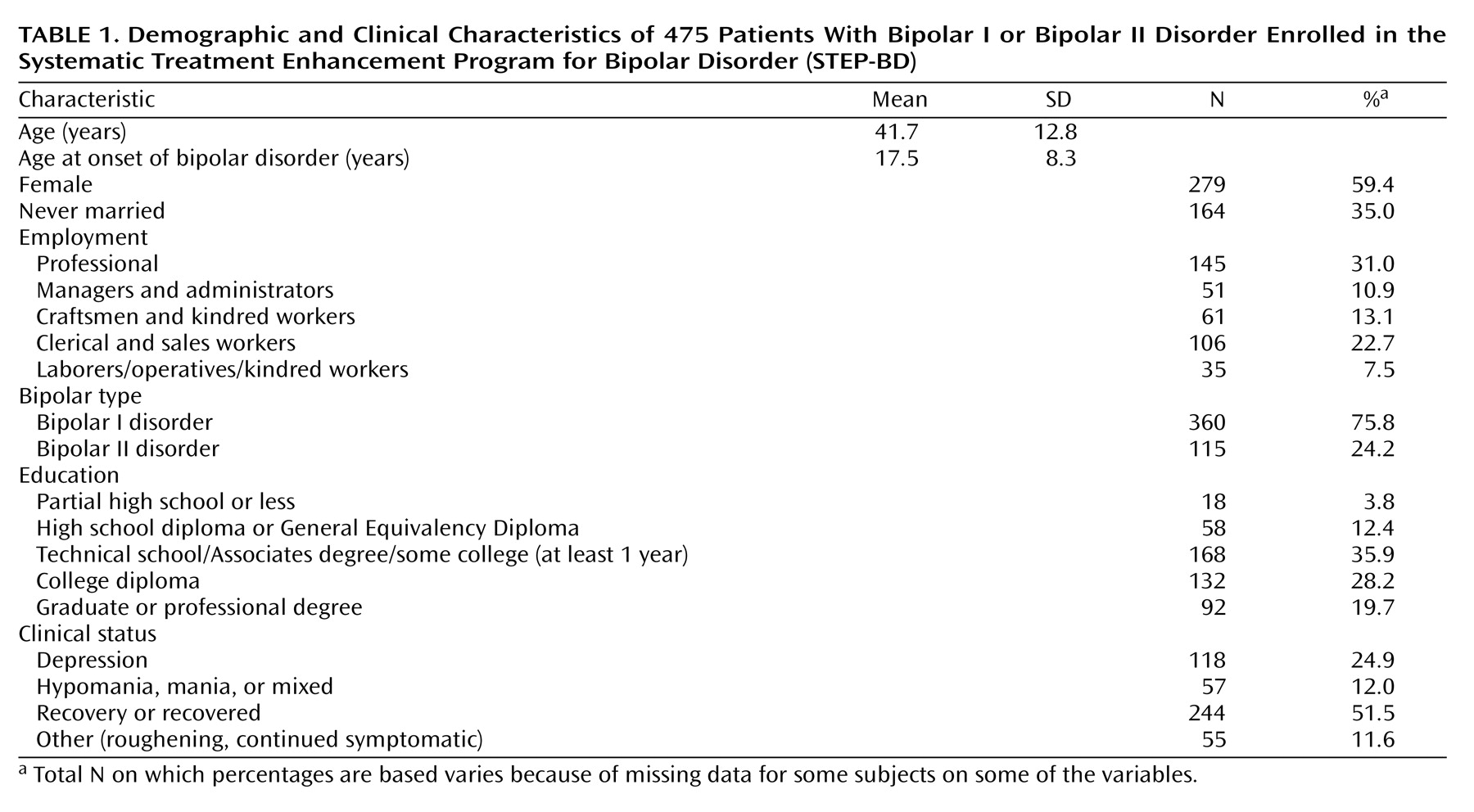
Patient characteristics are presented in
Table 1. Twenty-five patients of the original 500 were excluded because of missing diagnostic or clinical status data at baseline.
Comorbid Anxiety and Bipolar Disorder Type
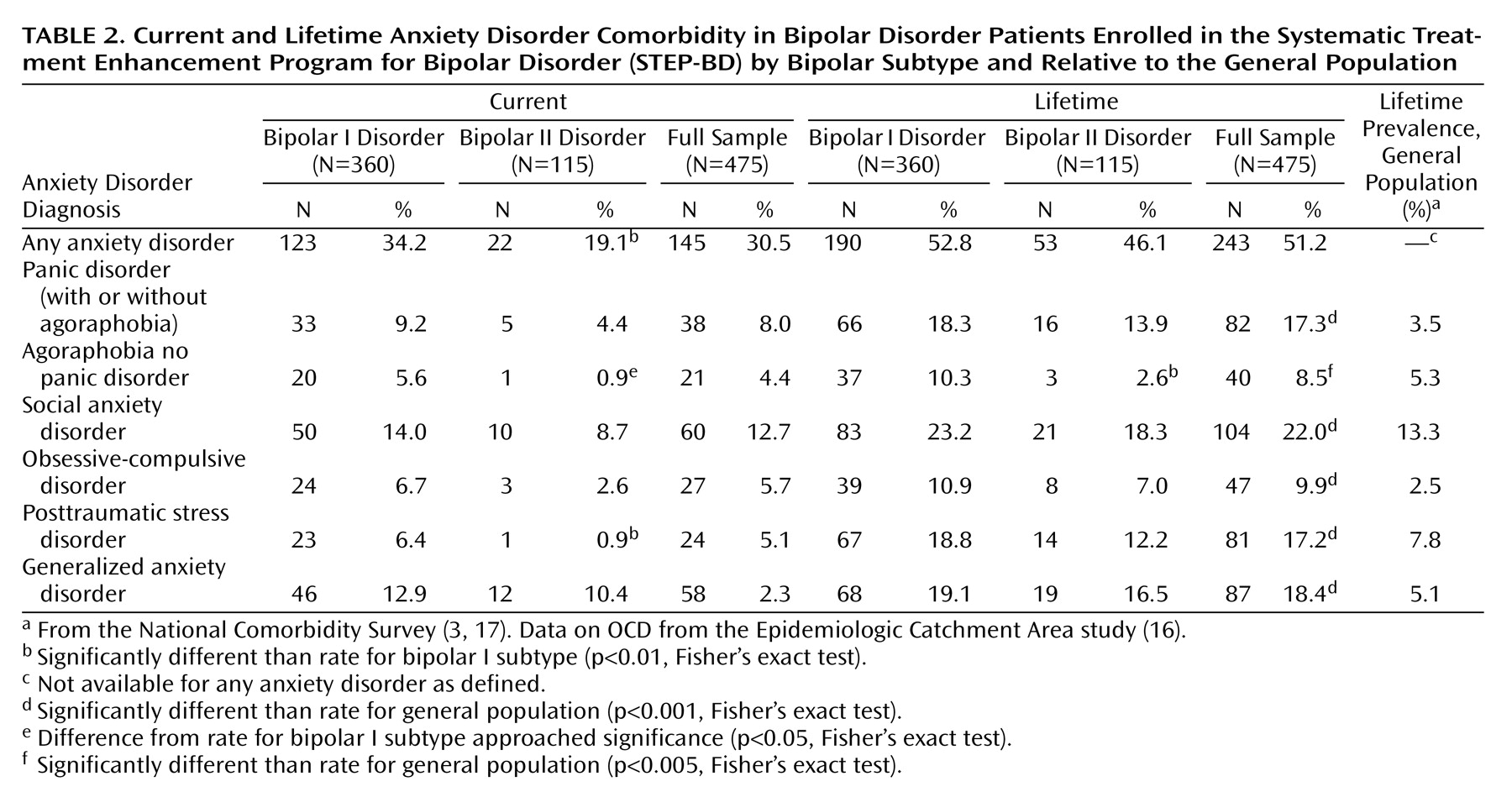
The prevalence of any lifetime anxiety disorder for the entire sample was 51.2% and was 30.5% for any current anxiety disorder. Greater overall anxiety comorbidity was seen among patients with bipolar I disorder relative to bipolar II disorder (
Table 2), reaching significance only for the presence of at least one current anxiety disorder, current PTSD, and lifetime agoraphobia without panic. The lifetime prevalence of each individual anxiety disorder in the STEP-BD participants was compared with each respective anxiety disorder’s general population prevalence rate from the National Comorbidity Study
(3,
17), with the exception of OCD, for which only an Epidemiologic Catchment Area study prevalence rate is available
(16). The STEP-BD participants uniformly demonstrated significantly higher lifetime prevalence rates for each individual anxiety disorder than the general population (one-sample test of proportions: all p<0.005) (
Table 2).
Comorbid Anxiety and Bipolar Disorder Severity
Age at onset of bipolar disorder was significantly lower for patients with any lifetime anxiety disorder (mean=15.6 years, SD=7.9) than in patients without an anxiety disorder (mean=19.4 years, SD=8.3) (t=5.03, df=471, p<0.0001) and in the presence of each single anxiety disorder except agoraphobia without panic and OCD. Patients with a lifetime anxiety disorder diagnosis had completed less education (Cochran-Armitage Test for Trend z=3.40, p<0.001).
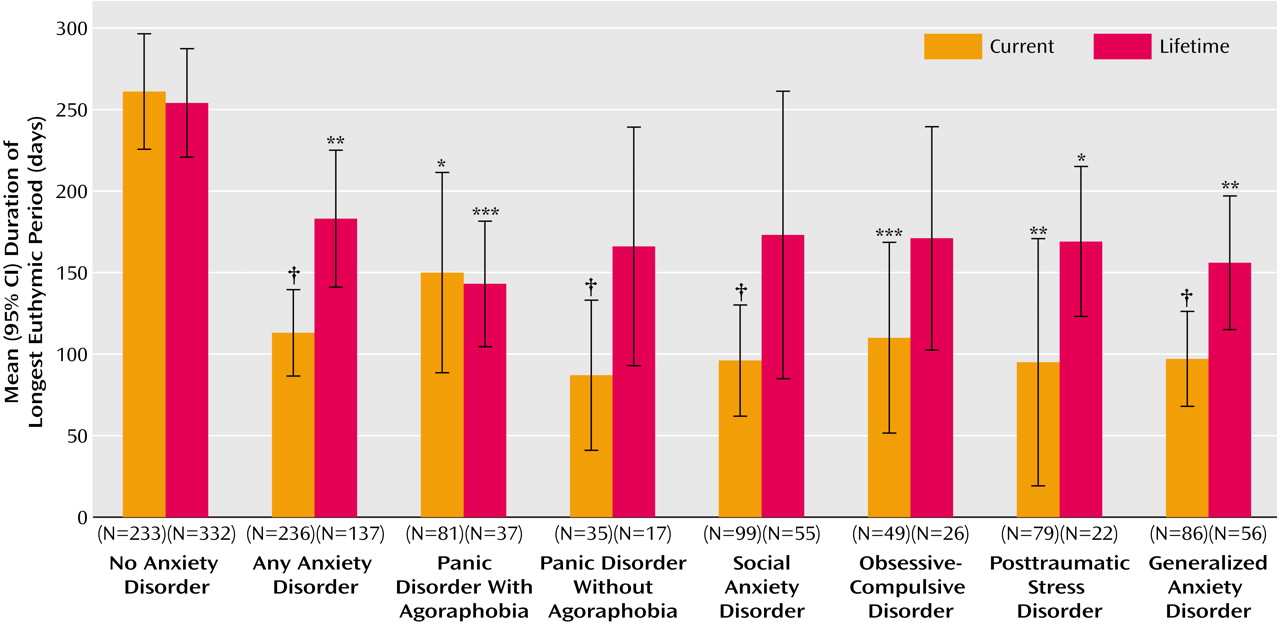
There was wide variability across the sample in the reports of the maximum number of continuous euthymic days in the 2 years before study entry (mean=218, SD=290). Nonetheless, the presence of at least one or any individual current anxiety disorder was associated with a dramatically shorter time euthymic; the longest number of euthymic days was reduced to less than half in the presence of almost all individual anxiety disorders (
Figure 1). This effect was also present, but to a lesser degree, for participants with a lifetime history of any anxiety disorder. When both a history of anxiety disorders and current (persisting) anxiety were entered as predictors in a multiple regression equation, only current anxiety offered significant prediction. Furthermore, at baseline evaluation, 59.3% of participants with no current anxiety disorder were recovering or recovered, compared with only 33.8% with at least one anxiety disorder, (p<0.0001, Fisher’s exact test). The proportion of participants currently recovering or recovered was significantly lower in the presence of most individual current anxiety disorders (p<0.01, Fisher’s exact test) with the exception of OCD and panic. For example, only 21% of those with PTSD and 33% of those with generalized anxiety disorder were recovering or recovered.
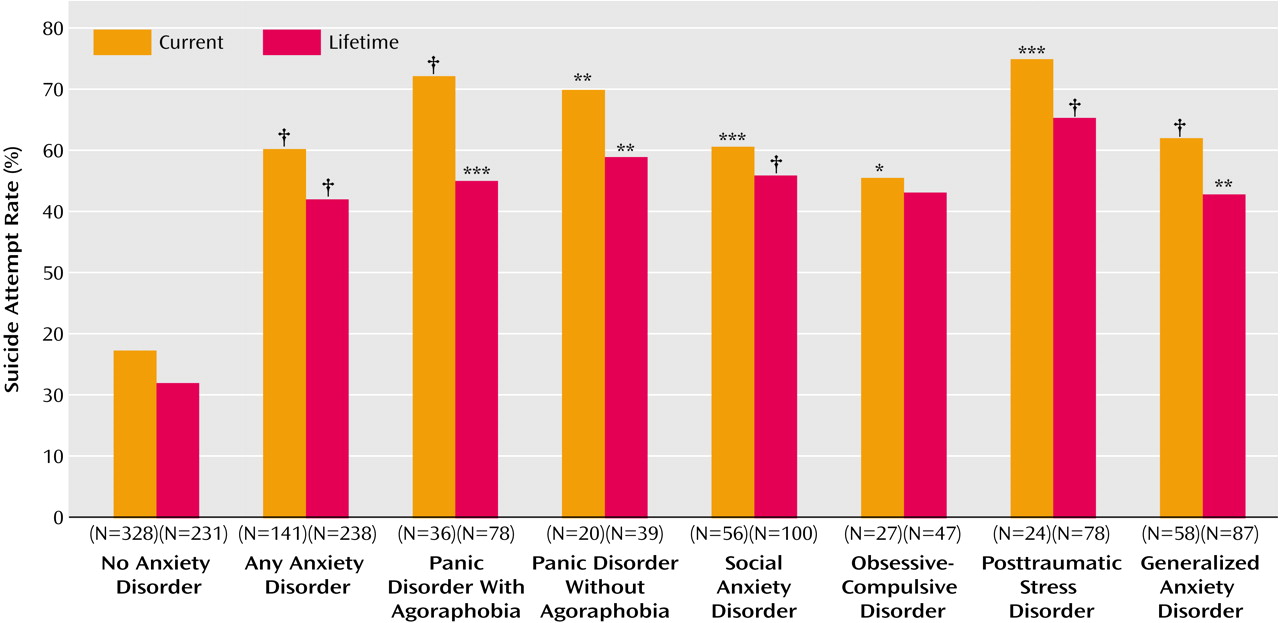
Rates of lifetime suicide attempts were significantly elevated for patients with at least one lifetime anxiety disorder and for each individual anxiety disorder, with the exception of OCD (
Figure 2).
Alcohol and Substance Abuse and Anxiety
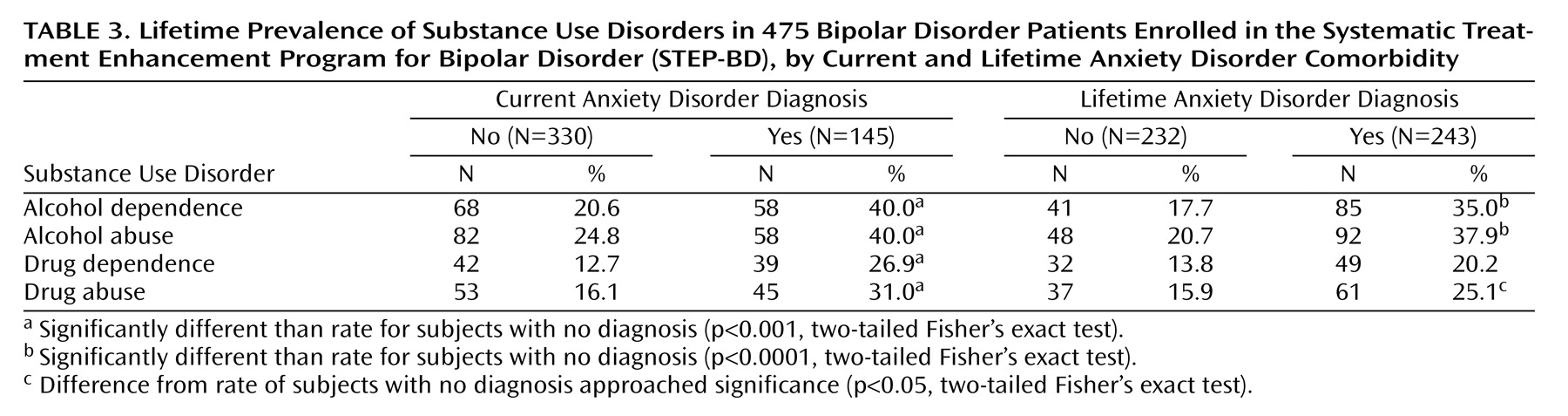
Although lifetime alcohol and substance use disorders were prevalent for the entire sample (37.8% with alcohol abuse or dependence, 26% with substance abuse or dependence), prevalence rates were significantly elevated for those with a current or lifetime anxiety disorder (
Table 3). For example, the presence of at least one current anxiety disorder was associated with a doubling of the rate of lifetime alcohol dependence, with 40%–50% of patients with lifetime panic disorder, agoraphobia, social anxiety disorder (all p<0.001) and PTSD (p<0.01) affected (data not shown).
Quality of Life and Function
Anxiety disorder comorbidity was also significantly associated with diminished quality of life and role functioning. The presence of each current anxiety disorder (with the exception of OCD) was associated with poorer functioning (as measured by the Range of Impaired Functioning Tool) and poorer quality of life (as measured by the Quality of Life and Enjoyment Scale) (data not shown). For both of these variables, a lifetime history of comorbid anxiety disorder offered only redundant prediction to the presence of a current anxiety disorder. When the impact of at least one current anxiety disorder on these measures was examined on the basis of current bipolar status, this effect was significant for the Range of Impaired Functioning Tool only for recovered or recovering patients (t=–5.8, df=235, p<0.0001). However, quality of life was worse as determined by the Quality of Life and Enjoyment Scale regardless of bipolar state (t=6.9, df=344, p<0.0001).
Independent Association of Anxiety Disorders With Bipolar Disorder Severity
Because the presence of nonrecovered/recovering bipolar state and alcohol or substance use disorders were common in patients with anxiety disorders, we examined the independent association of anxiety comorbidity with measures of illness severity. We examined three regression models with the Quality of Life and Enjoyment Scale, the Range of Impaired Functioning Tool, and longest euthymic period within the preceding 2 years serving as separate outcome variables. For each model, we examined the impact of at least one current comorbid anxiety disorder after lifetime alcohol or substance abuse/dependence and current bipolar clinical state (e.g., depressed, manic/hypomanic/mixed, euthymic) were controlled. A current anxiety disorder was associated with a robust and consistent detrimental impact on quality of life (t=4.67, p<0.0001), role functioning (t=4.09, p<0.0001), and number of days euthymic (t=3.41, p<0.001), even after current clinical state and the presence of lifetime substance use disorders were controlled. For example, anxiety comorbidity was associated with reduction in length of euthymia from 262 to 113 days. Further, for all three regression models, there was no interaction of anxiety with substance use, suggesting that the detrimental effect associated with anxiety occurs independent of lifetime drug or alcohol abuse or dependence.
Similarly, even when each of the aforementioned covariates was controlled, the presence of a lifetime anxiety disorder was associated with an odds ratio for suicide attempt of 2.45 (95% confidence interval [CI]=1.4–4.2; Wald χ2=11.07, p<0.001) relative to patients without comorbid anxiety, with a similar tendency (odds ratio=1.9, 95% CI=1.09–3.4; Wald χ2=5.19, p<0.05) for those with a current anxiety disorder. Finally, to ensure that differences in functioning and suicide history among patients with anxiety disorders were not dependent on the duration of the bipolar disorder, we examined this variable as a covariate in multiple regression analyses. In the multiple regression analyses including duration of bipolar illness, the presence of comorbid anxiety disorders continued to predict each of the four indices of poorer functioning: less time euthymic, poorer quality of life, greater functional impairment, and an elevated risk for suicide attempts.
Multiple Anxiety Comorbidity
We evaluated the additive influence of multiple anxiety comorbidity by examining the association of number of anxiety disorders (i.e., none, one, two, or more than two) with measures of quality of life, functional impairment, and period of time euthymic, after controlling for current clinical status and substance use in regression models. The presence of multiple anxiety comorbidity was independently associated with added impairment in quality of life (t=2.87, p<0.01) and functioning (t=3.01, p<0.01) and tended to be associated with longest period euthymic (t=2.12, p<0.05).
Discussion
In the largest clinical sample of patients with bipolar I and bipolar II disorder reported to date, we found high levels of anxiety comorbidity, consistent with the growing literature from epidemiologic and outcome studies. We found elevated anxiety comorbidity in bipolar I disorder as did McElroy and colleagues
(1), in contrast to reports of an anxiety association specific to bipolar II disorder derived primarily from primary anxiety disorder samples, not primary bipolar cohorts
(18,
19).
Our findings of a worse course and poorer functioning among patients with a comorbid lifetime anxiety disorder are consistent with previous observations
(1,
5,
9,
10), although our study extends these findings by examining the independent influence of substance abuse and anxiety comorbidity.
In our study, the degree of overlap between anxiety disorders and substance use disorders was striking. Nonetheless, in regression analyses examining the independent prediction afforded by each comorbidity, anxiety comorbidity continued to be significantly associated with poorer outcome (less time euthymic, poorer quality of life, greater functional impairment, and elevated risk for suicide attempts).
In particular, there was a dramatic and significant prediction of past suicide attempts by the presence of a lifetime anxiety disorder, with an odds ratio of 2.45, even after controlling for potential confounding by alcohol and substance disorder comorbidity and clinical bipolar state. Thus, lifetime anxiety comorbidity appears to be a significant marker of risk for a reported history of suicide attempts.
Our finding of a significantly younger age at onset of bipolar disorder in those with lifetime anxiety comorbidity is consistent with epidemiologic data suggesting that the presence of anxiety disorders may predict the onset of bipolar disorder
(4), and research work by the Stanley Foundation group
(1). Similarly, panic disorder with onset prior to age 21 has been reported to have a significantly higher association with bipolar disorder than later-onset panic disorder
(20). Further, a 10-year prospective study of 717 adolescents found that, after controlling for adolescent mania, the presence of a childhood anxiety disorder predicted onset of bipolar disorder in young adulthood
(21). However, the precise nature of the relationship between anxiety and bipolar illness remains unclear. Early anxiety may represent a prodromal symptom of bipolar disorder, or alternately, anxiety and bipolar disorders may share an associated biology or genetic risk. For example, recent genetic and family studies have supported a specific panic disorder-bipolar disorder connection, with evidence for a comorbid subtype with shared genetic transmission in some families
(22,
23). Moreover, we found that the link between comorbid anxiety disorders and greater disability in bipolar disorder patients was independent of the duration of the bipolar disorder. In addition, anxiety symptoms may, in some cases, represent an inherent component of a more severe bipolar disorder subtype, perhaps attributable to dysphoric stimulation rather than a distinct disorder.
Although there is a growing awareness of the need to treat comorbid disorders such as panic and PTSD
(24), anxiety interventions have not been highlighted as critical for high-risk bipolar patients nor for integration into suicide prevention strategies. In our study, anxiety disorders were consistently associated with poorer functioning. More than a decade ago, Fawcett and colleagues suggested anxiety symptoms may be a modifiable risk factor for suicide in individuals with mood disorders
(25), but the field has been slow to develop specific anxiety-targeted interventions for patients with bipolar disorder and anxiety comorbidity. Although Frank, Cyranowski, and Shear are developing a modification of interpersonal psychotherapy for patients with unipolar depression and panic comorbidity (MH-49115, E. Frank, principal investigator), there are currently no data examining the efficacy of any anxiety treatment for the prevention of suicide attempts or improvement of clinical course specifically for patients with bipolar disorder. Furthermore, little is known about the precise mechanism by which anxiety elevates suicidality, and study of this issue may need to precede the development of interventions specifically aimed at suicide prevention in this population. Patients with acute anxiety may be less capable of tolerating uncomfortable affects and utilizing other resources, such as social supports or cognitive strategies, to reduce suicidality. Psychosocial interventions to prevent suicide should focus in part on problem-solving skills and improved tolerability of distress
(26).
Conclusions drawn from the present study are limited by the cross-sectional nature of the assessments. Specifically, we are unable to address issues of causality and whether anxiety disorders predispose individuals with bipolar disorder to a worse course, or whether it is the characteristics of the bipolar disorder itself that determine anxiety onset. However, inclusion of patients at all levels of symptom severity, treatment, and phase of illness allows for broad generalizability. Nonetheless, conclusions based on some of our subsample analyses with less prevalent anxiety disorders or affective states (e.g., manic/hypomanic/mixed) are limited by relatively low power. In addition, the performance of multiple statistical comparisons may have increased the risk of false positive findings (type I error), although this is tempered to some degree by the use of a significance level of 0.01.
We do not know the extent to which comorbid anxiety motivates patients to seek care. Hence, our clinical sample may overrepresent this comorbidity relative to non-treatment-seeking populations (i.e., Berkson’s bias)
(27) and may contribute to our finding of elevated anxiety prevalence compared with rates from epidemiologic samples. However, our results concur with the high levels of overall comorbidity (59.3%) found for bipolar I disorder in the epidemiologically derived National Comorbidity Survey sample
(4). In contrast, our rates of substance abuse may be low, given that patients with substance use disorders may be more likely to present at or be referred to primary substance abuse treatment programs than general psychiatric settings. Finally, our reliance on retrospective self-report for lifetime disorders and severity of illness at this cross-sectional assessment does not protect from the possible bias that patients with greater severity of illness may have been more likely to acknowledge a history of anxiety in a structured interview.
Of note, our results do not address the impact of differential anxiety severity nor subsyndromal anxiety features. Anxiety symptoms below the threshold to meet criteria for diagnosis may still exert a pernicious effect on the course of bipolar disorder. For example, lifetime panic spectrum symptoms and traits, regardless of formal panic disorder diagnosis, are associated with greater bipolar severity and longer time to remission with treatment
(10). Similarly, poorer treatment outcome has been reported for patients with panic or anxiety symptoms and bipolar I disorder
(9). Further research to address these issues is currently ongoing.
In conclusion, anxiety disorder comorbidity is prevalent and appears to be an independent marker of greater severity of bipolar illness and suicide attempts. The presence of anxiety comorbidity should signal a need for enhanced clinical monitoring of suicidality, and a greater understanding of this connection is critical. Little is known about whether effective treatment of anxiety symptoms can lessen bipolar severity, improve response to treatment of manic or depressive symptoms, or reduce suicidality. Further research examining the impact of anxiety on treatment response and course in bipolar disorder is ongoing as part of the STEP-BD study. These efforts may further elucidate the impact of anxiety on bipolar disorder and the need for additional or alternate intervention for patients with bipolar disorder and anxiety comorbidity.
Acknowledgments
Core investigators and collaborators for the Systematic Treatment Enhancement Program for Bipolar Disorder are as follows: Contract: Gary S. Sachs, M.D. (principal investigator), Michael E. Thase, M.D. (co-principal investigator). Site principal investigators and co-principal investigators: Lauren B. Marangell, M.D., and James M. Martinez, M.D. (Baylor College of Medicine); Joseph R. Calabrese, M.D., and Melvin D. Shelton, M.D. (Case Western Reserve University); Michael W. Otto, Ph.D.*, Andrew A. Nierenberg, M.D., and Gary S. Sachs, M.D. (Massachusetts General Hospital and Harvard Medical School); R. Bruce Lydiard, M.D.* (Medical University of South Carolina); Joseph F. Goldberg, M.D. (New York Presbyterian Hospital and Weill Medical College of Cornell University); James C.-Y. Chou, M.D., and Joshua Cohen, D.O. (New York University School of Medicine); John Zajecka, M.D.* (Rush-Presbyterian St. Luke’s Medical Center); Terence A. Ketter, M.D., and Po W. Wang, M.D. (Stanford University School of Medicine); Uriel Halbreich, M.D.* (State University of New York at Buffalo); Alan Gelenberg, M.D.* (University of Arizona); Mark Rapaport, M.D.* (University of California, San Diego); Marshall Thomas, M.D., Michael H. Allen, M.D., and David J. Miklowitz, Ph.D. (University of Colorado Health Sciences Center); Rif S. El-Mallakh, M.D. (University of Louisville School of Medicine); Peter Hauser, M.D.* (University of Maryland); Jayendra Patel, M.D. (University of Massachusetts Medical Center); Kemal Sagduyu, M.D. (University of Missouri-Kansas City School of Medicine, Western Missouri Mental Health Center); Mark D. Fossey, M.D., and William R. Yates, M.D. (University of Oklahoma College of Medicine); Laszlo Gyulai, M.D., and Claudia Baldassano, M.D. (University of Pennsylvania Medical Center); Michael E. Thase, M.D., and Edward S. Friedman, M.D. (University of Pittsburgh Western Psychiatric Institute and Clinic); and Charles L. Bowden, M.D., and Cheryl L. Gonzales, M.D. (University of Texas Health Science Center at San Antonio). Executive Committee: Mark S. Bauer, M.D., Charles L. Bowden, M.D., Joseph R. Calabrese, M.D., Jennifer Conley, M.A., Maurizio Fava, M.D., Gary Gottleib, M.D., Ellen Frank, Ph.D., Terence A. Ketter, M.D., Jane N. Kogan, Ph.D., David Kupfer, M.D., Leslie Leahy, Ph.D.*, Lauren B. Marangell, M.D., David J. Miklowitz, Ph.D., Michael W. Otto, Ph.D., Jerrold F. Rosenbaum, M.D., Matthew V. Rudorfer, M.D., Gary S. Sachs, M.D., Linda Street, Ph.D., Michael E. Thase, M.D., and Sean Ward. NIMH Liaisons: Matthew V. Rudorfer, M.D., Joanne Severe, M.S., and Linda Street, Ph.D.
*No longer participating in this role.