Mania During Treatment of Chronic Hepatitis C With Pegylated Interferon and Ribavirin
Case History
Mr. C is a 39-year-old African American man with a remote history of injection drug use who was referred to the general psychiatry inpatient unit of Johns Hopkins Hospital for evaluation and treatment of psychotic mania characterized by elation, irritability, grandiosity, impulsive generosity, insomnia, hypersexuality, delusions of external control, and excessive religiousness. These symptoms occurred within 3 weeks of his receiving treatment with pegylated IFN-α and ribavirin for chronic hepatitis C.
Past History
Mr. C’s father’s personal and psychiatric history was unknown. His mother, who died in her 50s from complications of diabetes mellitus, had abused alcohol. Mr. C had seven siblings; six had abused illicit drugs (one brother died in drug-related violence and another was still in active addiction), but no sibling had any other psychiatric history. A maternal aunt suffered depression; another aunt died of Alzheimer’s disease. Several cousins were addicted to heroin and cocaine.Mr. C is the product of a normal pregnancy and birth. He had normal developmental milestones and a happy childhood. The family was lower-middle-class, his mother a single parent who worked two jobs. Mr. C dropped out of school in the 10th grade because of addiction to illicit drugs. He has worked as a truck driver for 12 years. He had a teenage son from his first marriage and lived with his fiancée, their infant son, and his two stepsons. A few years ago he was arrested for domestic violence, but charges were dropped. He has no current legal problems. He is a committed Christian who attends church services and Bible study regularly.Mr. C smoked cigarettes occasionally in his early teens and started smoking marijuana at age 11 or 12. He started drinking alcohol at age 13 and abusing heroin and cocaine at age 14; physiological and psychological dependence on these substances quickly developed and continued until 1993. He has been abstinent from all substances, including cigarettes, for 11 years and is very actively involved in peer-led rehabilitation programs.Mr. C vaguely recalled a positive hepatitis C virus antibody test, possibly when he was 19. He was rediagnosed with hepatitis C virus infection 5 years ago during a self-referred screening examination for sexually transmitted disease. He has chronic hepatitis C and is HIV negative. He is receiving dietary treatment for diabetes mellitus but has been treated with insulin in the past. He has no known environmental or medication allergies.His medications at admission were fluoxetine, 40 mg, in the morning; pegylated IFN-α, 180 μg once a week; ribavirin, 1200 mg once a week; and zolpidem, 10 mg at bedtime (he had been taking up to 30 mg for several nights).During the early months of recovery from addiction, Mr. C experienced euphoria and heightened optimism for a few weeks after a religious conversion. He did not experience irritability, grandiosity, insomnia, restlessness, elevated libido, or other phenomena that would suggest affective disturbance. He has since maintained a satisfying spiritual life. Five years ago, he broke up with a girlfriend because she was actively using illicit drugs. He grieved the loss of the relationship, struggled with drug cravings (but did not resume drug use), and developed feelings of anger and despair. He eventually became suicidal and homicidal and was hospitalized in a psychiatric unit for about 7 days. He was treated for depression with fluoxetine, 20 mg/day. He continued to take fluoxetine and experienced no further episodes of depression.
Present Illness
Mr. C saw a hepatologist early in 2001 as recommended by his physician; the workup included liver biopsy, which showed stage 3 precirrhotic disease. Treatment with IFN-α and ribavirin (three times a week) was started in August 2001. Within the first few weeks of treatment Mr. C developed fatigue and a flulike syndrome. He also developed sadness and tearful episodes. His physician increased the dose of fluoxetine to 40 mg/day, and his mood improved. There was some evidence of viral suppression after 4 months, at which time the hepatologist recommended a switch to pegylated IFN-α and ribavirin, which had recently become available. While trying to fill the new prescription, Mr. C missed enough doses of IFN-α and ribavirin to be given a drug holiday. The fatigue and the flulike symptoms remitted.He started to take pegylated IFN-α and ribavirin injections (once weekly) in January 2002. Within 3 weeks, he developed restlessness and insomnia as well as episodes of unprovoked laughter, irritability, and tearfulness. These symptoms evolved into euphoria, impulsive generosity, increased libido, excessive religiousness, thought disorder (flight of ideas), ideas of reference, grandiose delusions, and delusions of external control (by mobile phone and telepathic communication).He confronted colleagues at work over religion; later he obeyed a “telepathic message” and quit his job. In the week before his hospitalization, he went 4 days without eating. He was belligerent when his family confronted him regarding his bizarre behavior, and he threatened his fiancée for “having sex with others.” He continued to take pegylated IFN-α and ribavirin despite instructions from his hepatologist to stop, and he did not comply with referral to a psychiatrist. After almost 2 weeks of psychosis, his fiancée took him to the emergency room for evaluation. He came to the emergency room in an agitated and disorganized state and was treated with haloperidol and diphenhydramine, with calming effect, before being involuntarily admitted to the inpatient unit.On admission, Mr. C was a tall, overweight African American man. He was alert and cooperative. He was not agitated. He was talkative, and his associations were loose. He was euphoric and grandiose. He denied having hallucinations, and delusions were not elicited. He denied suicidal or homicidal ideation as well as aggressive impulses. He did not have obsessions, compulsions, or phobias. Insight and judgment were poor. He could not answer questions on the Mini-Mental State Examination (MMSE). On physical examination, vital signs were found to be normal, and he looked healthy. The remainder of the physical examination was unremarkable.The initial formulation focused on Mr. C’s mania superimposed on a previous history of depression. The religious conversion was felt to be an earlier episode of mania, and Mr. C was diagnosed with bipolar disorder, type I, manic episode. The possibility that pegylated IFN-α triggered this mania was considered, given the temporal association and published reports of mania during interferon treatment. We did not think that fluoxetine precipitated the mania because he had been taking it for a few years and the dose increase had occurred several months earlier. Given his sustained alertness and a presentation typical for mania, delirium was considered unlikely. Resumption of heroin and cocaine use was excluded by history and laboratory testing during the emergency room evaluation.The initial goals for Mr. C’s treatment were to establish a diagnosis, interrupt the mania, encourage his participation in treatment (through discussion of the reasons for hospitalization, illness education, and family involvement), and initiate appropriate pharmacotherapy.Admission laboratory tests included CBC with differential, metabolic panel, tests of liver and thyroid function, urinalysis, urine toxicology screen, serum vitamin B12 and folate levels, and RPR. Thyrotropin (TSH) level was 0.36 μIU/ml and a repeat TSH level was 0.53 μIU/ml (range=0.50–4.50); free T4 and T3 were normal. Alanine aminotransferase (ALT) was 47 IU/liter and aspartate aminotransferase (AST) was 43 U/liter. Urinalysis revealed gross hematuria. Results of other tests were negative. Brain computerized tomography (CT) was normal.Mr. C cooperated with evaluation and treatment. Pegylated IFN-α, ribavirin, fluoxetine, and zolpidem were discontinued. He received haloperidol, 5 mg orally at bedtime, for the psychosis. The next day mild dystonia (jaw and neck stiffness) was relieved by a single oral 1-mg dose of benztropine, and the haloperidol dose was then decreased to 1 mg at bedtime. On the second hospital day, Mr. C gave voluntary consent for hospitalization. Lithium was prescribed at an initial oral dose of 150 mg twice daily. He participated actively in illness education, therapeutic groups, and occupational therapy.Ultrasound and CT scan of the kidneys revealed a benign cyst in the right kidney and a smaller cyst in the lower pole of the left kidney. A repeat urinalysis showed resolution of the hematuria; further evaluation was deferred to his primary physician. By the third day, the mania had remitted. Lithium was increased to 300 mg twice daily. Serum ALT and AST levels were normal. On the fourth day, haloperidol was discontinued and he was discharged home. The discharge plan included follow-up care with his physician and his hepatologist.
Follow-Up
Mr. C was to see the outpatient psychiatrist a week later. A few days after discharge, he developed nausea, malaise, and abdominal cramping. The outpatient psychiatrist (C.U.O.) reduced the lithium dose to 300 mg/day, and the symptoms resolved. Mr. C was seen in the hepatitis psychiatry clinic several days later in the company of his fiancée, who reported that he had completely recovered and was in his usual mental and physical state.During the office visit, Mr. C was calm, alert, attentive, and cooperative. He was talkative, but his verbal associations were normal. He had many questions about his recent mania and about lithium. He had a normal mood and a normal range of affect. Self-attitude, level of energy, and libido were normal. He denied suicidal, homicidal, and aggressive thoughts or impulses. He denied having hallucinations. Delusions and experiences of passivity were not elicited. He did not have obsessions, compulsions, or phobias. Insight and judgment were good. On the MMSE he scored 30 of 30.Mr. C’s psychiatric history was carefully reviewed during the initial office visit. He described his religious conversion 9 years earlier. That conversion experience differed qualitatively from the recent episode of mania. There had been no behavioral or perceptual disturbances, no grandiosity or delusions, and he had maintained his usual social and work habits. He had sought and received spiritual mentorship from his pastors, and under their guidance his spirituality had matured over the years. On the basis of this information, we concluded that he had not had a previous episode of mania. Thus the recent episode of mania was his first, attributable to treatment with pegylated IFN-α, and the DSM-IV diagnosis of substance-induced mood disorder, manic type, was made.Mr. C did not want to take medication indefinitely unless absolutely necessary. We decided to continue lithium treatment until he had resumed work and had several additional months of social and psychological stability. Fluoxetine was not restarted because of our concern that doing so might lead to recurrence of mania. Mr. C agreed initially with this approach, but he stopped taking lithium a few weeks later. He continued follow-up visits and has remained stable at his pre-episode baseline since. He has returned to work, is now married, and he and his wife have another child.Mr. C has declined pegylated IFN-α and ribavirin because of the mania experience, and his physician concurs because liver transaminase levels were normal at follow-up several months ago. Mr. C still maintains an active spiritual life; his confidence in his spirituality was initially shaken—this came up in psychotherapy, and he also sought spiritual counseling from his pastor—but that has resolved. He still participates actively in substance abuse rehabilitation programs, and he now does voluntary guidance counseling for prisoners about to be released as well as recently released prisoners.
Discussion
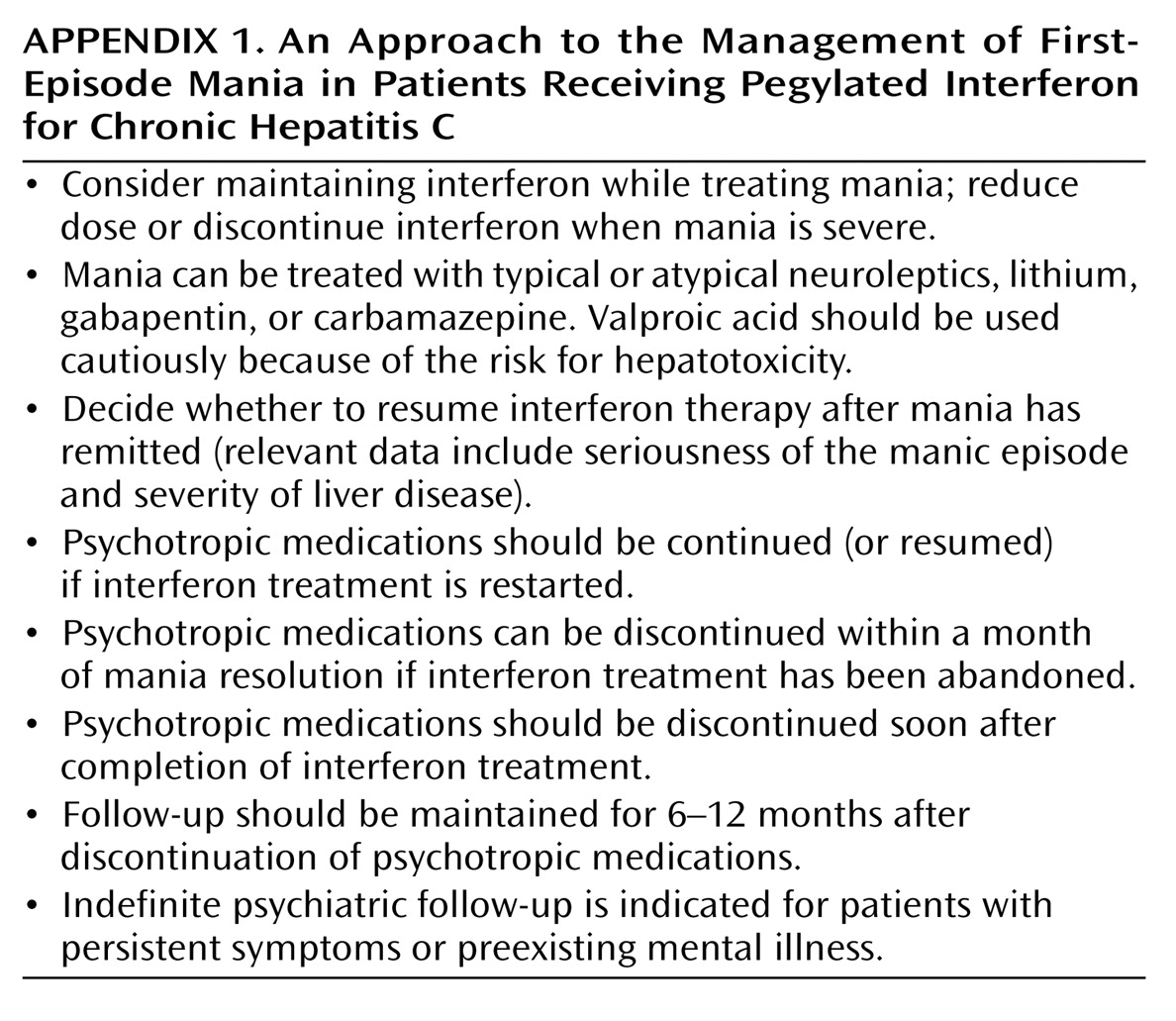
Recommendations
Conclusions
Footnote
References
Information & Authors
Information
Published In


History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
There are no citations for this item
View Options
View options
PDF/ePub
View PDF/ePubGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).