Gender Differences in Violence in the General Hospital Population
For the first 30 months of this 4-year study, we gathered information on all hospital admissions. There were 1,487 patients (459 women and 1,028 men) who met the inclusion criteria for the study. Of these, 189 patients (64 women and 125 men) engaged in one or more physical assaults during their first 2 months of hospitalization. The percentage of violent women (13.9%) in the hospital was similar to that of the violent men (12.2%).
We compared the violent and the nonviolent patients with regard to other demographic and diagnostic characteristics. The groups did not differ in ethnic background. The violent patients were younger than the nonviolent patients (mean age=33.0 years [SD=8.2] versus 36.5 years [SD=8.5], respectively; t=4.88, df=1486, p<0.0001). There was a significant difference in the number of patients who were violent in the different diagnostic categories based on chart diagnosis (χ2=5.36, df=2, p<0.05). There were more schizoaffective patients in the violent group relative to their number in the nonviolent hospital population. There was also a difference in the number of men and women in each diagnostic category, with more women in the schizoaffective and bipolar group and relatively fewer in the schizophrenia group. We conducted a multiple logistic regression analysis in which diagnosis was entered as a covariate; no difference was found in the proportion of violent male and female patients.
Overall Characteristics of the Violent Male and Female Patients
Over the 4-year duration of the study, 253 patients (174 men and 79 women) were eligible for the study. These patients had committed a physical assault during their first 2 months of hospitalization and met the inclusion criteria. Seven of these refused to participate, while 246 provided informed consent and underwent the initial evaluation within 3 days of the first incident. Of these, 24 did not complete the 4-week study period. Therefore, there were 222 patients (155 men and 67 women) who completed the 4-week study period with all evaluations. These 222 patients were used in the final data analyses reported here. They did not differ in demographic characteristics or diagnosis from the 31 patients who were not included in these analyses. There were no significant differences in violence between these two groups.
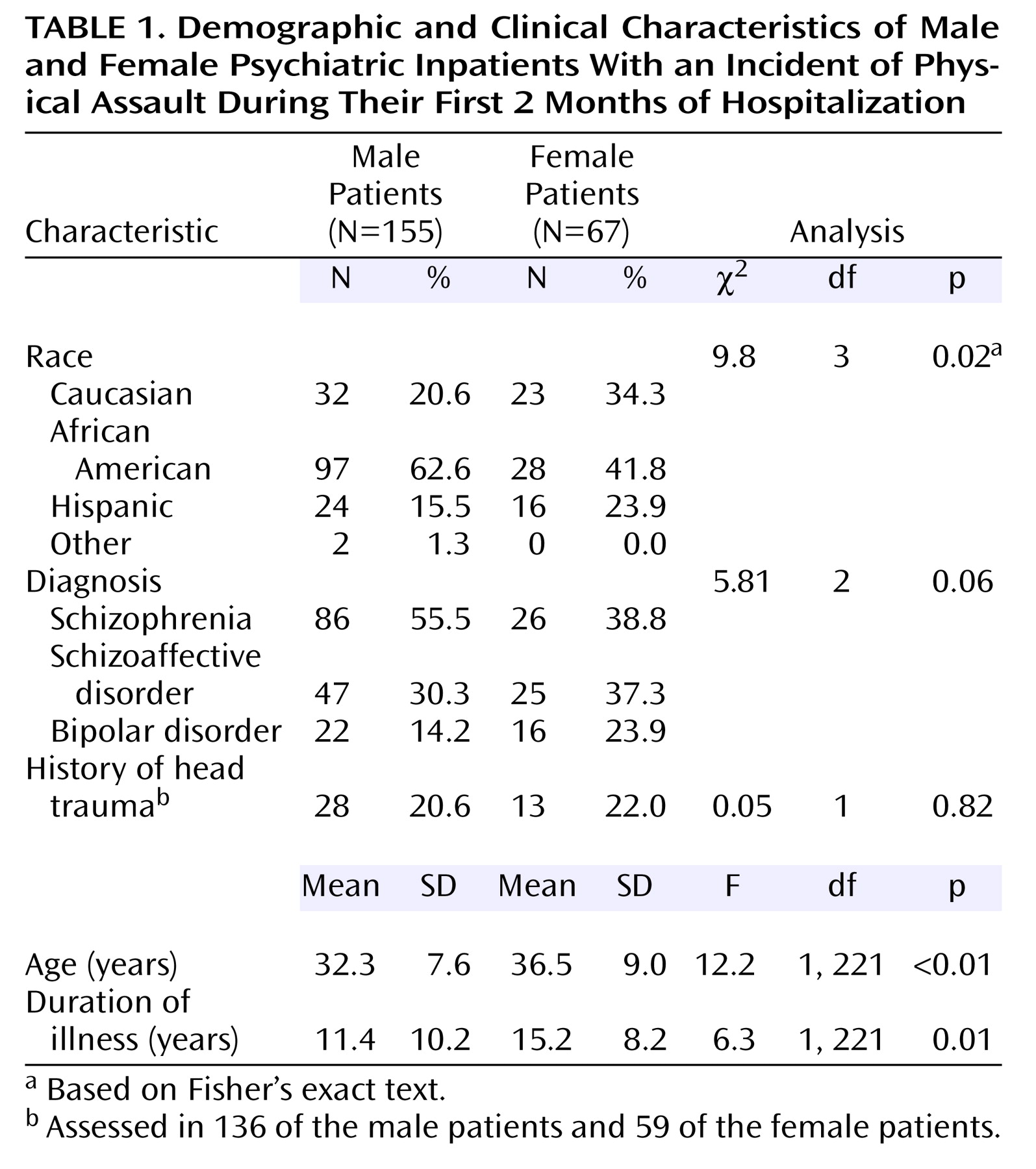
Table 1 shows the demographic, diagnostic, and other characteristics of the men and the women in the final sample. The men and women differed significantly in ethnic background, age, and duration of illness. The women were older and had a longer duration of illness. There were proportionately more African Americans in the male than in the female group. There was a marginal difference in diagnosis, with proportionately more women diagnosed with schizoaffective disorder and bipolar disorder than with schizophrenia. We entered these variables in the various analyses; the inclusion of age, duration of illness, and ethnic background did not have an impact on the results; diagnosis, however, did affect the results and was therefore entered as a covariate in all analyses.
There were no gender differences in head trauma. The average antipsychotic daily doses (in chlorpromazine equivalents) for the first and last weeks of the study were also calculated; there were no significant gender differences.
Gender Differences in Violent Behaviors
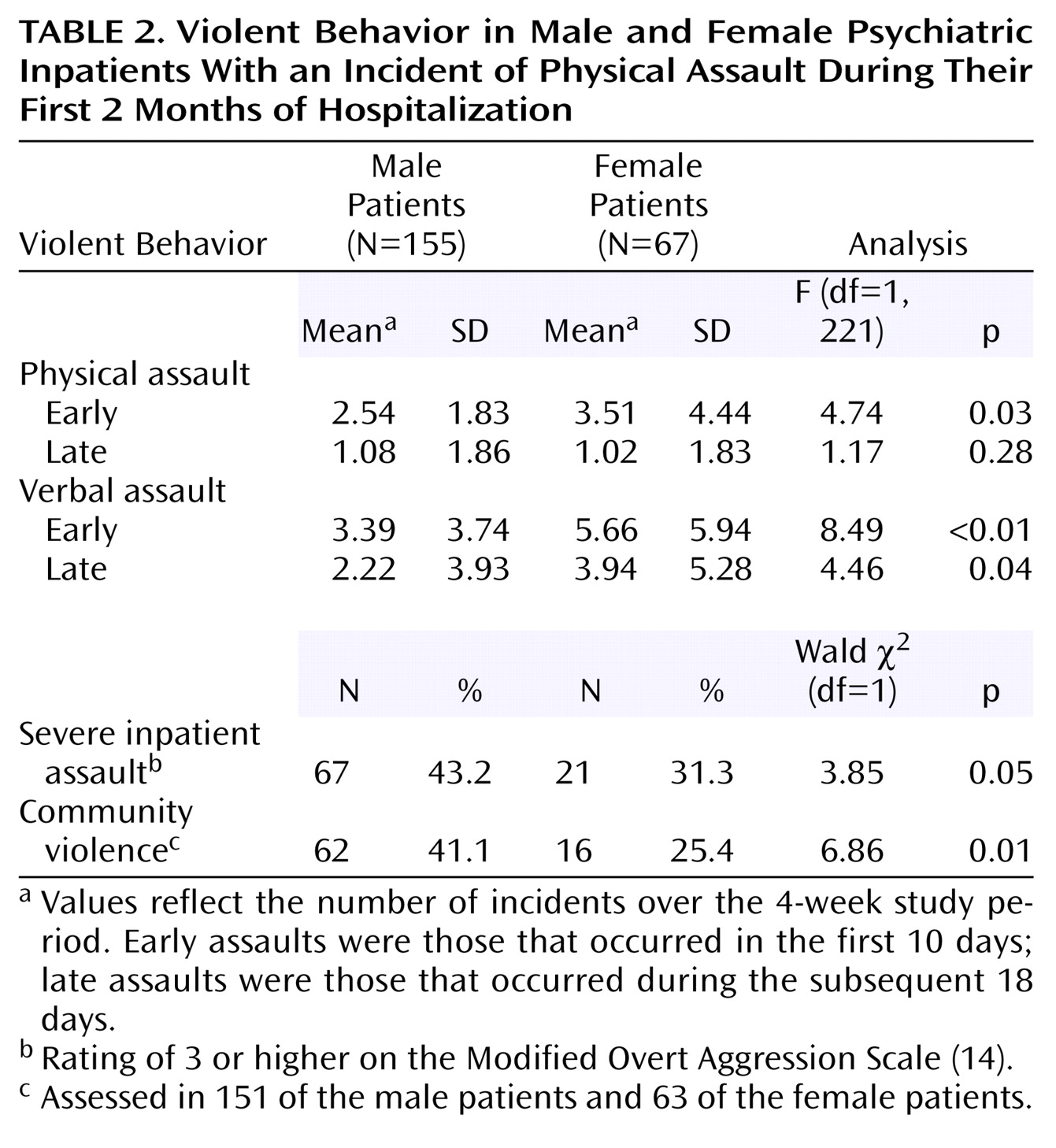
Gender differences in the frequency and course of physical and verbal assaults over the 4-week period were analyzed through hierarchical linear modeling (with diagnosis as a covariate). ANCOVA was then used to compare the number of assaults in men and women cross-sectionally during the two time periods. The number of inpatient assaults in the early and late periods is indicated in
Table 2.
Women tended to have a higher total number of physical assaults than the men during the 4-week period (F=3.45, df=1, 217, p=0.06). There was a statistically significant interaction between gender and change in physical assaults (F=5.20, df=1, 217, p=0.02), with a greater decrease in physical assaults for the women than for the men. Actual gender comparisons for the two time periods indicate that the women had significantly more physical assaults in the early period but not in the late period, where there was no difference (
Table 2).
Similar to the physical assaults, the total number of verbal assaults was higher in women than in men during the 4 weeks (F=12.98, df=1, 217, p<0.001). There was also a statistically significant interaction between gender and change in verbal assaults over the 4 weeks (F=3.93, df=1, 217, p<0.05), with a greater decrease for the women. ANCOVA indicated that the women presented with significantly more verbal assaults than the men both in the early period and in the late period (
Table 2).
There were gender differences in the severity of inpatient physical assaults. A higher proportion of men than women inflicted physical injury to their victim (i.e., assaults that were rated as “3” or higher on the Modified Overt Aggression Scale) (
Table 2).
History of physical assaults in the community was evaluated as a discrete variable (presence or absence of such assaults). As indicated in
Table 2, a significantly higher proportion of men (41%) than women (25%) were physically assaultive in the community. Six of the patients committed homicides; they were all men.
Clinical Differences in Violent Behaviors
There were no significant overall gender differences in BPRS positive or negative symptom scores or in NOSIE subscale scores.
Physical assaults and clinical symptoms
In both men and women, frequency of physical assaults was related to BPRS positive symptom score (F=5.39, df=1, 216, p=0.02). It was also related to the NOSIE irritability (F=11.42, df=1, 199, p<0.01), routine (F=20.17, df=1, 199, p<0.01), and social (F=8.22, df=1, 199, p<0.01) subscale scores, indicating that greater impairment on these scales was associated with a greater number of physical assaults.
There were no significant interactions between gender and BPRS factors in determining physical assaults. There was, however, a significant interaction between gender and score on the NOSIE routine subscale (F=3.92, df=1, 199, p<0.05), indicating that the impact of routine on physical assaults differed in men and women. There was also a tendency for gender to interact with score on the NOSIE social subscale (F=3.54, df=1, 199, p=0.06).
In order to interpret the direction of these two interactions, we computed least square means. At high impairment on the routine subscale, the women had much higher physical assaults than the men, whereas at low impairment, there were only small gender differences. Similar results were obtained for the NOSIE social subscale. Thus, impairments in the ability to follow ward routines and in social interactions are more likely to result in physical assaults in the women than in the men.
Verbal assaults and clinical symptoms
In both men and women, frequency of verbal assaults was related to positive symptom score (F=52.72, df=1, 216, p<0.01) and negative (BPRS anergia factor) symptom score (F=9.71, df=1, 216, p<0.01). Frequency of verbal assaults was also related to scores on the NOSIE irritability (F=50.79, df=1, 199, p<0.01), routine (F=27.60, df=1, 199, p<0.01), and social (F=4.08, df=1, 199, p=0.04) subscales, indicating that a greater impairment on these clinical scales was associated with a greater total number of verbal assaults.
For the verbal assaults, there was a significant interaction between positive symptoms and gender (F=6.85, df=1, 216, p=0.01). There were also significant interactions between gender and scores on the NOSIE irritability (F=17.48, df=1, 199, p<0.001), routine (F=12.36, df=1, 199, p<0.001) and social (F=6.91, df=1, 199, p<0.01) subscales.
The aforementioned clinical variables had a different impact on verbal assaults for women than for men. Similar to the analyses for physical assaults, the interactions between gender and these variables in determining verbal assaults were further interpreted through least square means. When these symptoms were more severe, the women were more verbally aggressive than were the men, whereas when the symptoms were not severe, there were essentially no gender differences in verbal assaults.
Course of inpatient physical assaults in men and women
In order to understand better the high level of physical assaults among women in the early period and its rapid decrease over time, we integrated the data in a multivariate model that allowed us to identify complex relationships among variable sets. First, canonical correlation analysis was performed in order to investigate the relative importance of clinical symptom configurations in relation to particular patterns of violent behaviors. This method can be thought of as extension of factor analysis for two sets of variables. Its objective is to obtain as high a correlation as possible between the two sets of variables (factors). This technique is an optimal linear method for studying interset associations: components (factors) from the two sets are extracted jointly in a way maximizing the correlation between the components. In our study, the two sets of variables that were used comprised the violence parameters and the clinical symptoms. The violence parameters consisted of early and late physical assaults as well as change in assaults over time. The clinical symptoms included baseline and endpoint measures of positive symptoms (BPRS psychosis/conceptual disorganization, activation, and hostility/suspiciousness) and negative symptoms (BPRS anergia).
Second, an additional analysis was performed to investigate how men differed from women in terms of the relationship between the basic dimensions of violence and the basic clinical correlates (identified through the canonical correlation analyses).
Canonical correlation analyses assessed the degree of association between the violence parameters and the clinical measures. The three violence parameters formed one side of the model, and the measures of positive and negative symptoms formed the other side.
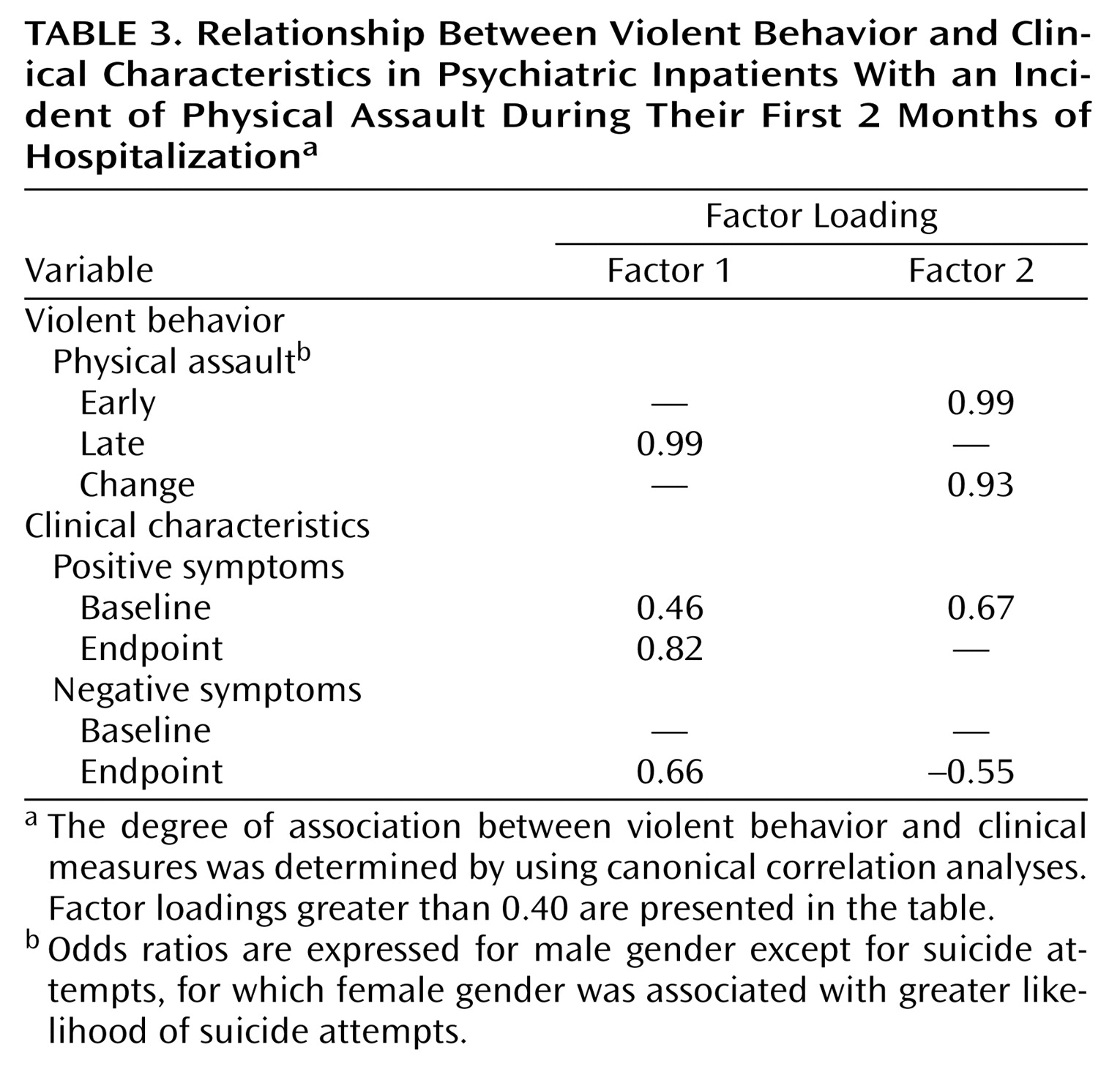
Two significant dimensions (canonical factors) of inpatient physical assaults were identified in relation to clinical symptoms (
Table 3).
As indicated by the canonical factor loadings, the first dimension (canonical factor 1) was characterized by late physical assaults and represents a more persistent form of violence associated with more enduring symptoms; it was positively related to both endpoint positive and negative psychotic symptoms. The second dimension (canonical factor 2) was characterized by early physical assaults and marked decrease in assaults over time. It was positively associated with early positive symptoms and negatively with late negative symptoms. Thus, it represents a transient form of violence that is accompanied by remitting positive symptoms and absence of enduring negative symptoms.
We looked at the difference in the above dimensions of violence (canonical factors) as a function of gender. There was no gender difference for the first dimension, but women had a significantly higher value than the men on the second dimension (F=6.14, df=1, 208, p=0.01). Thus, this early and remitting violence, which is strongly influenced by the symptom configuration of acute positive psychotic symptoms and absence of enduring negative symptoms, is more prominent in the women than in the men.
Psychosocial Factors
In the literature, factors such as drug abuse, school truancy, and property crime were related to community violence. We examined the relationship of these factors to community violence in our sample. We also investigated the contribution of gender to the risk factor with diagnosis as a covariate. Community violence was significantly related to substance abuse (odds ratio=2.2, 95% confidence interval [CI]=1.04–4.7; Wald χ2=4.2, df=1, p=0.04), theft and property crime (odds ratio=4.8, CI=2.4–10.0; Wald χ2=18.4, df=1, p<0.001), and to school truancy in childhood (odds ratio=2.9, CI=1.6–5.5; Wald χ2=11.4, df=1, p<0.001). There was no relationship, however, between community violence and a history of suicide attempts.
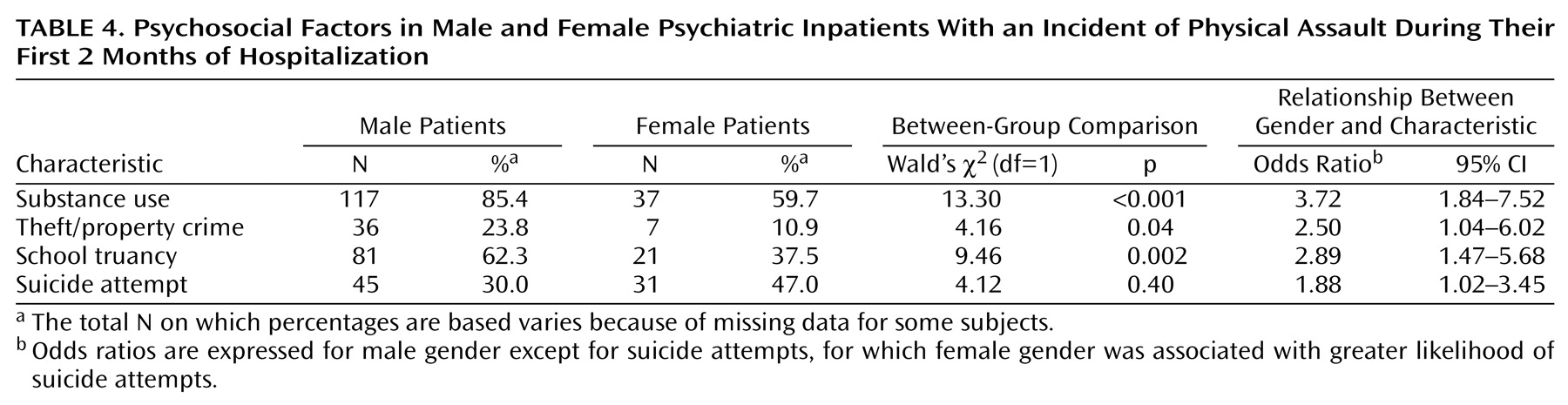
There were significant gender differences in these psychosocial factors (
Table 4). The men had a higher prevalence of substance abuse, theft and property crime, and school truancy in childhood than the women. The women, on the other hand, had a higher prevalence of suicide attempts than the men (
Table 4).