The estimated annual rate of presentation to general hospitals in the United Kingdom after self-poisoning has increased in recent years to 170,000 per year
(1). In the United States the number of presentations after deliberate self-harm has been reported as 650,000 per year, and the number of deaths by suicide as 30,000 per year
(2). A key risk factor for suicide is previous deliberate self-harm. Risk of suicide increases 50
(3) to 100
(4) times within the first 12 months after an episode of self-harm, compared to the general population risk. Approximately one-half of persons who die by suicide have a history of self-harm
(5), and this proportion increases to two-thirds in younger age groups
(6). A reduction of suicidal behavior is an explicit goal of national strategies for suicide prevention in the United Kingdom
(7) and the United States
(8). In England, the government’s national strategy
(7) supports the target of reducing the rate of suicides and undetermined deaths by one-fifth by 2010
(9). To achieve this goal, appropriate evidence is needed to inform preventive strategies and health service management.
Previous studies of suicide after deliberate self-harm have considered demographic and clinical risk factors and have involved comparatively small numbers of individuals followed up over a long period
(4,
10–12). In such studies temporal cohort effects may be operating, and findings may not be applicable to current service provision. We used a large database of self-harm cases to estimate suicide rates during a follow-up period of up to 4 years after a self-harm episode. We had three principal aims: 1) to estimate suicide rates after deliberate self-harm, 2) to investigate the timing of suicide in relation to a previous episode of self-harm, and 3) to investigate potential sociodemographic and clinical predictors of suicide.
Method
The Manchester and Salford Self-Harm Project is a collaboration between the University of Manchester and all four hospitals with an emergency department in the cities of Manchester and Salford. Information is collected on individuals presenting to these departments as a result of deliberate self-harm. Self-harm is defined as an act of intentional self-poisoning or injury irrespective of the apparent purpose of the act
(13). Previous studies in Manchester have suggested that about one-third of individuals in this population have psychiatric follow-up
(1). A more detailed account of service provision in the study area is discussed elsewhere
(14). The project covers a predominantly economically deprived urban population of about 600,000 people.
After an episode of self-harm, a standard assessment form is completed by the emergency doctor and by psychiatric staff for those patients who have a psychiatric assessment. The completion rate for assessment forms is monitored continuously, and for the study period, this rate was 78%. The form includes details of the self-harm episode, clinical and demographic data, and information about the patient’s mental state and clinical management. As reported in a previous study
(15), “low-risk” management refers to self-harm patients discharged from the emergency department without psychiatric follow-up, and “high-risk” management designates patients who are referred to medical or surgical services and/or seen by a mental health specialist.
We conducted a prospective cohort study of deliberate self-harm attendees at the four emergency departments between September 1, 1997, and August 31, 2001. A comprehensive matching process was used to identify deaths by suicide (ICD-9 codes E950–E959) and undetermined cause (ICD-9 codes E980–E989) during the study period, hereafter referred to as “suicides,” from the National Confidential Inquiry Into Suicide and Homicide by People With Mental Illness database obtained from the Office for National Statistics
(16). The overall risk of suicide within 1 year was calculated (excluding patients from the fourth year of the cohort whose follow-up period was less than 365 days). Age- and gender-specific suicide rates per 100,000 person-years were calculated and compared with equivalent rates for the populations of England and Wales and of Manchester; standardized mortality ratios (SMRs) were calculated for female subjects, male subjects, and all subjects. The reference populations for the SMRs were females in the general population for the female subjects and males in the general population for the male subjects. As the highest prevalence of suicide is in men ages 25–35 years and 15–24-year-old males had the highest rate of increase of suicide in the 1990s in the United Kingdom, we compared patients ages <35 years with those ages ≥35 years. Previous studies have also compared similar groups.
Potential risk factors were investigated by using hazard ratios generated by Cox’s proportional hazards models. For these models, explanatory variables were categorized into the following domains: sociodemographic, clinical (including circumstances of the index episode of self-harm, history of treatment and previous self-harm, and alcohol and drug use), mental state, and precipitants. Univariate associations were examined initially, and then multivariate models were generated within each domain by using backward stepwise procedures. Explanatory variables were retained in these models if the p value was less than 0.2. The independent predictors from all the domain-specific models were then fitted in a final multivariate model. Explanatory variables were retained in the final model if the p value was less than 0.1. Risk management by the emergency department was dichotomized (moderate- to high-risk management versus low-risk management) and compared by using Cox’s regression analysis. Analyses were carried out with SPSS
(17) and Stata
(18).
Results
Cohort Characteristics
The cohort consisted of 7,968 individuals presenting with deliberate self-harm from September 1, 1997, to August 31, 2001, for whom assessment forms were completed. An audit of records for episodes without a completed assessment form showed that the patients’ age and gender did not differ from those for episodes with an assessment form. The median age of the patients was 30 years (interquartile range=21–40 years, range=10–92 years); 4,500 (57%) were female. A total of 1,231 (15.5%) of 7,964 patients repeated self-harm before the end of the study period. Thirteen of the 60 cohort members who died by suicide (22%) had reported no previous deliberate self-harm at the index episode; 11 (18.3%) of the 60 repeated self-harm before their actual suicides.
Suicide Rates
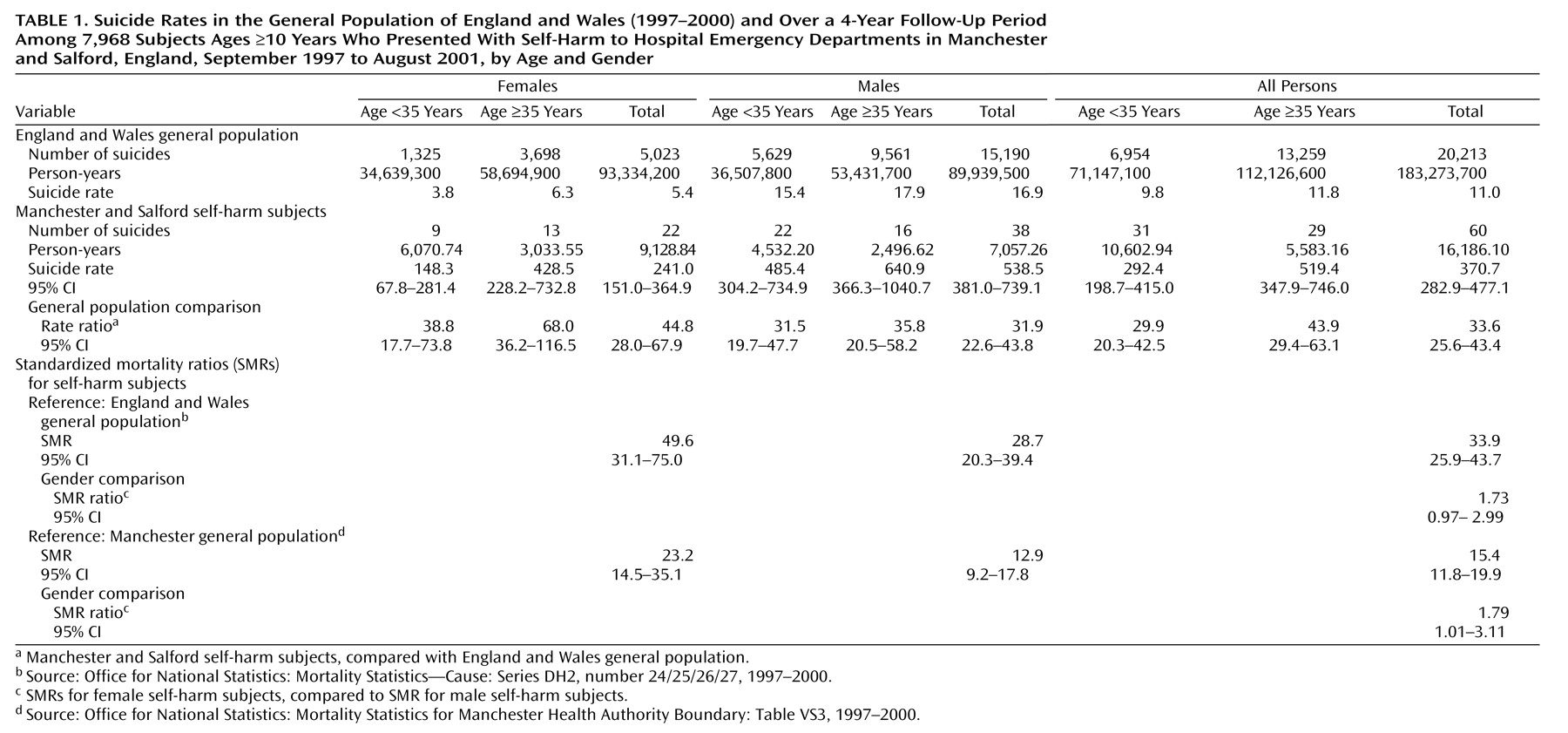
As
Table 1 shows, 60 of the 7,968 subjects subsequently committed suicide, a rate of 371 per 100,000. These deaths included 36 identified as suicide (ICD-9 codes E950–E959) and 24 identified as deaths of undetermined cause (ICD-9 codes E980–E989). Male subjects who harmed themselves were more likely to commit suicide than female subjects, and this gender difference was observed for both younger and older age groups. Using standardized mortality ratios to adjust for age and gender differences between the study population and that of England and Wales, we found that the number of suicides in the self-harm cohort was 34 times higher than expected; the number was 50 times higher for the female subjects and 29 times higher for the male subjects. The SMR for the female subjects was almost twice that for the male subjects.
Time-Period Effects
As
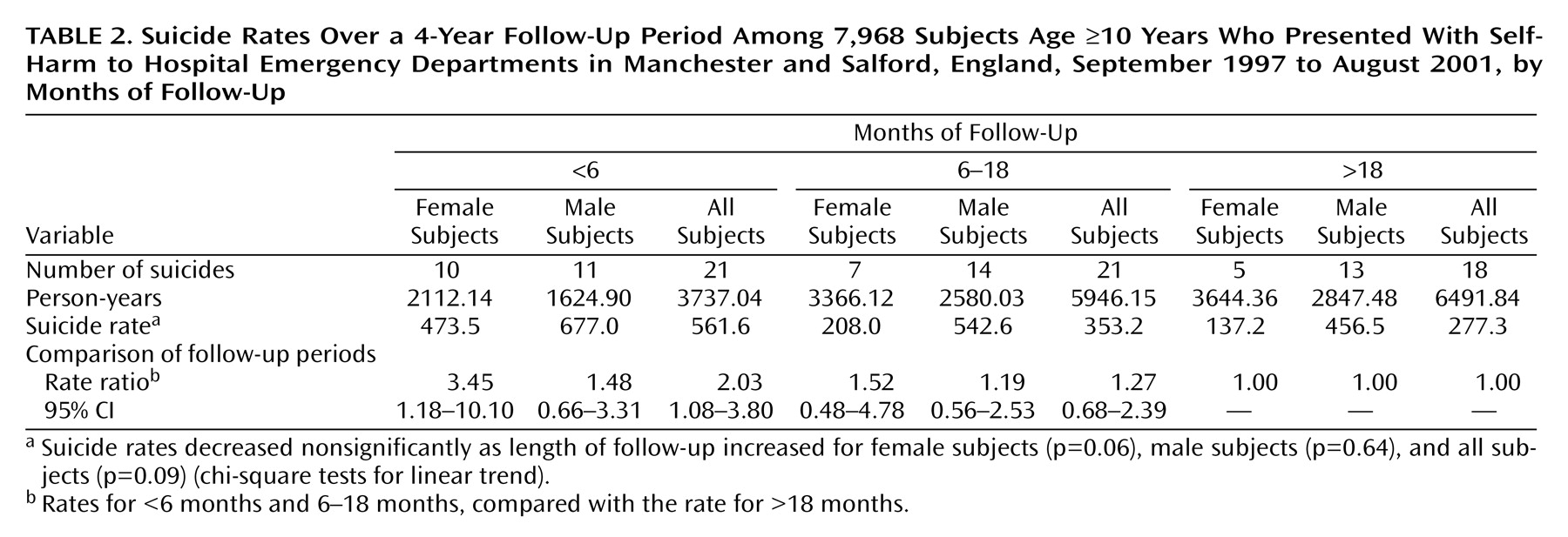
Table 2 shows, the risk of suicide in the first year of follow-up was 0.5% (95% confidence interval [CI]=0.4–0.8). The suicide rate for all persons in the cohort was highest in the first 6 months of follow-up (562 per 100,000). The suicide rate tended to decrease as length of follow-up increased; this result approached significance for the female subjects but not for the male subjects. Rates of suicide among the male subjects were higher than among the female subjects in all follow-up time periods.
Cox’s Regression
Univariate models
As
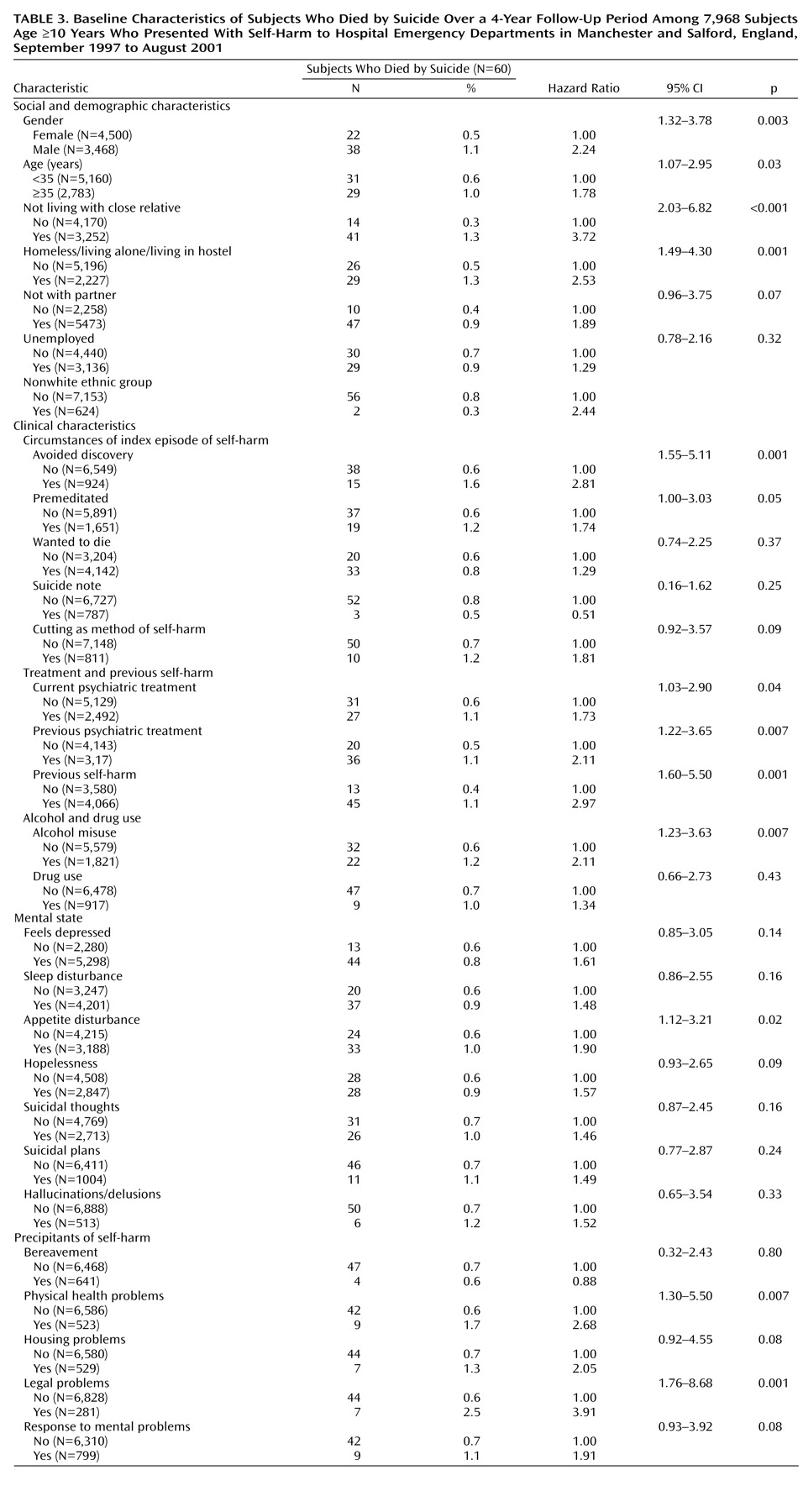
Table 3 shows, there were numerous associations of suicide risk with sociodemographic characteristics, clinical factors, and precipitants. The strongest associations within each domain were not living with a close relative, avoiding discovery (at the time of self-harm), previous self-harm, alcohol misuse, appetite disturbance, and legal problems. Apart from disturbance in appetite, symptoms of depression were not associated with future suicide. Data completeness in domain-specific models (before dropping any variables because of nonsignificance) was no lower than 86.8%.
Multivariate model
As
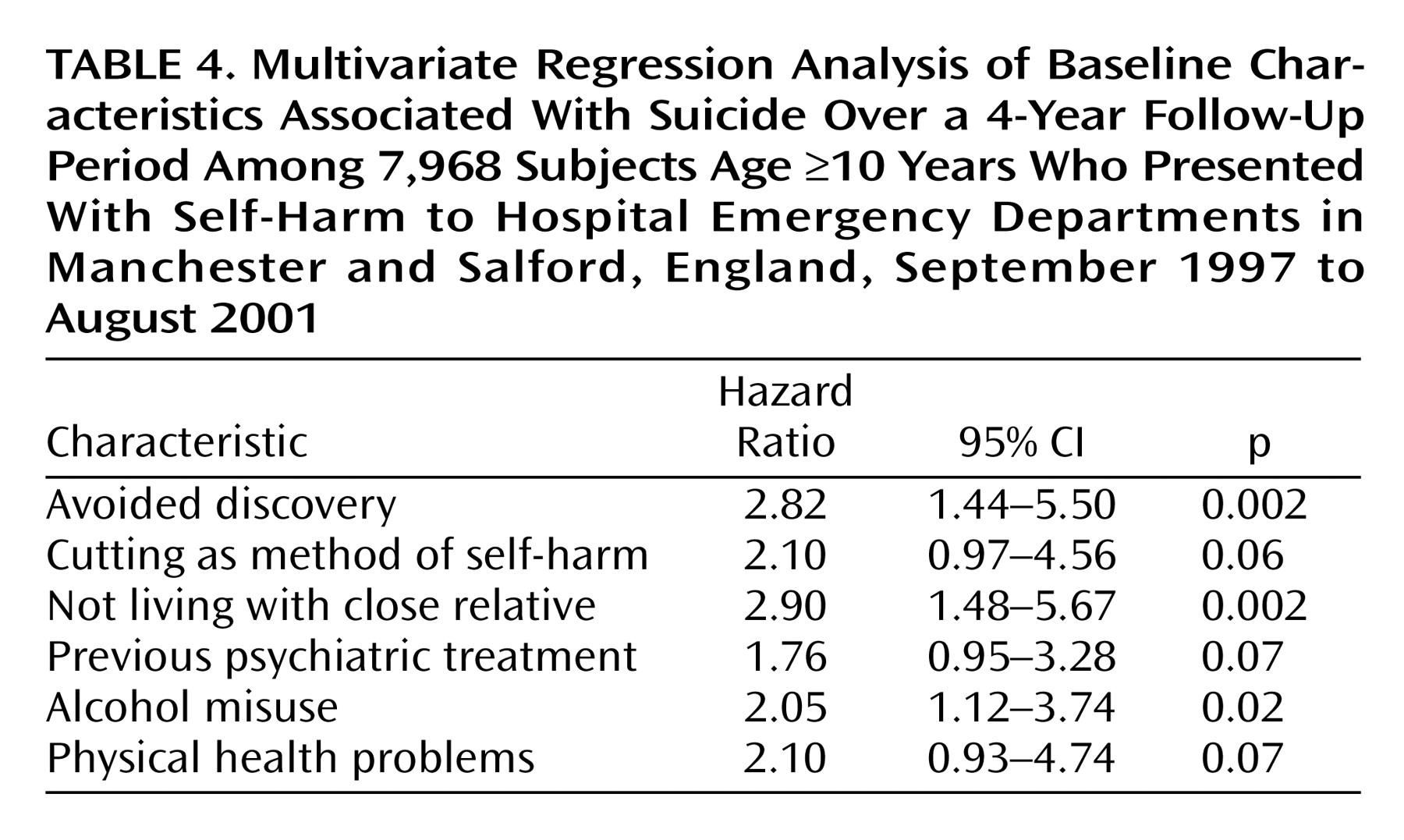
Table 4 shows, the independent predictors of suicide in a multivariate model were not living with a close relative, avoiding discovery at time of self-harm, and current alcohol misuse. The adjusted hazard ratio for these three variables indicated an approximate two- to threefold increase in the level of risk. In addition, the association of three variables—cutting as a method of self-harm, previous psychiatric treatment, and physical health problems—with suicide approached significance (p<0.1). Older age (p=0.26) and male gender (p=0.49) were found to be nonsignificant predictors and were dropped from the final multivariate model. The level of data completeness in the final model was 76.7%.
Interaction effects
The hazard ratios for four items in the multivariate model (avoiding discovery, cutting as a method of harm, physical health problems, and alcohol misuse) were higher for the male subjects than for the female subjects, suggesting that the effects might be restricted to male subjects. However, the interaction terms were not significant. The effect of alcohol misuse was restricted to subjects age <35 years (interaction term: p=0.04) (subjects age <35 years: hazard ratio=3.41, 95% CI=1.62–7.17; subjects age ≥35 years: hazard ratio=1.09, 95% CI=0.48–2.44). The effect of previous psychiatric treatment was also restricted to subjects age <35 years (interaction term: p=0.03) (subjects age ≥35 years: hazard ratio=3.59, 95% CI=1.58–8.14; subjects age ≥35 years: hazard ratio=1.06, 95% CI=0.50–2.25).
Clinical Management
High-risk management by emergency department staff was associated with an approximately twofold increase in risk of suicide (N=52 [0.8%] of 6,157 subjects), a result that approached significance (p=0.07; hazard ratio=1.99, 95% CI=0.95–4.19).
Discussion
Our results confirm a markedly high risk of subsequent suicide among patients who visit the emergency department after deliberate self-harm, relative to the general population. The cohort of deliberate self-harm patients in this study had more than 30 times the number of suicides that would be expected in the general population of England and Wales. However, the study cohort had 15 times more suicides than expected, compared with the population of Manchester, which has a suicide rate that is double the national average (20.5 versus 11.8 per 100,000)
(19,
20). Suicide risk was highest in the first 6 months after self-harm, and there was a higher risk in male subjects, compared to female subjects, that was consistent across time during the follow-up period. However, in terms of the observed versus expected numbers of suicides, the SMR was nearly twice as high for the female subjects as for the male subjects, and this ratio was higher than those found in previous studies in the United Kingdom
(4). The results suggest that hospital presentation with self-harm confers a higher risk of suicide (compared to the general population) in women than in men. Possible explanations for this finding include 1) the low rate of suicide in females in the general population, 2) a tendency of high-risk male self-harmers to not seek general hospital medical attention, and 3) inadequacy of hospital service provision for female self-harmers.
Several demographic, clinical, and management variables were associated with suicide in our study. In a multivariate model, not living with a close relative, avoiding discovery at the time of the index self-harm, and alcohol misuse were independently associated with suicide risk. These risk factors are similar to those identified in long-term follow-up
(21). In addition, previous psychiatric treatment and physical health problems—factors identified in other studies
(22–
24)—were shown to be important, and the risk associated with cutting as a method of self-harm emerged as a new finding. As these three factors were beyond conventional significance, perhaps because of low power, the results should be treated with caution. Another new finding was that the effects of alcohol misuse and previous psychiatric treatment were restricted to younger people in the study cohort.
Our finding that high-risk emergency department management is associated with a twofold increase in risk of suicide is difficult to interpret, but it does suggest that emergency department doctors are appropriately identifying a high-risk group. We know from a previous study that emergency department doctors’ assessment of suicide risk as high in self-harm patients is related to the finding of a high level of lethality of the self-harm method
(25).
Methodological Issues
Database studies that allow for record linkage are a highly valuable tool in psychiatric epidemiology
(26), but such studies are difficult to carry out in health care systems that are not centrally managed. In this large cohort study, we had access to databases that allowed investigation of suicides within a short period of time. The results are therefore applicable to contemporary service provision.
The relatively low number of suicides affected the power of the study, particularly within the subgroups studied. With the observed numbers of male (N=3,468) and female (N=4,500) subjects, there was 70% power to detect a significant relative risk of 2.0 (if 1% of the male subjects subsequently commit suicide compared with 0.5% of the female subjects) and 99% power to detect a significant relative risk of 3.0 (1.5%, compared with 0.5%). However, for explanatory variables with low exposure prevalence, the cohort lacked adequate power to detect relative risks of 2.0 or lower. This limitation is typical of many cohort studies
(27). Even though suicide was more common in our cohort than in the general population, a very large sample size is still required to study such a rare outcome. However, a number of variables were still significant, which highlights the importance of these factors.
We also did not ascertain those individuals who emigrated or who died from other causes, and all causes of mortality are known to have higher rates in self-harm patients. Nonresponse may be a potential source of bias, but responders were similar to nonresponders in age and sex. We are unable to say how many of the nonresponders died by suicide.
Previous studies have used age 35 years as a cutoff point in analyses of suicide by age
(6), and this division maximized power in our study (there were a similar number of suicides in each age group) but of course did not allow identification of any subgroup trends.
Implications for Clinical Practice
Previous studies have identified sociodemographic and clinical risk factors for suicide after self-harm. This study also identified factors related to hospital management that further inform understanding of the suicidal process and may be potentially modifiable. Our finding of higher risk of suicide during the first 6-month period after self-harm suggests that early intervention after self-harm might be helpful. To maximize the potential effect of suicide prevention strategies, interventions should target the high-risk group. However, our finding that the SMR was higher for women than for men is worth highlighting, because there may be a perception among clinicians that self-harm by women is not serious and that interventions should target young men in particular.
The multifactorial etiology of suicide means that prevention might best involve broad-based strategies
(6). Examples of preventive measures related to service provision include providing training in the recognition of risk and the treatment of suicidal patients. Treatment for suicidal patients would include treatment for alcohol misuse and concurrent physical illness. Further research might help clarify the nature of the relationship between physical illness (be it acute, chronic, or life-threatening) and suicidal behavior, and these findings could inform appropriate intervention. Population initiatives that increase the level of support for vulnerable groups, such as young men disengaged from society, might be also be beneficial.
Previous studies have compared suicide rates in study subjects with the rate for the population of England and Wales rather than the local rate. Future studies need to account for the local context. Our method could be attempted in other countries and in other settings, particularly in North America. Large randomized, controlled trials measuring a specific psychological intervention or type of service delivery for self-harm patients may be helpful. Problems with this research approach are well known and include difficulties with recruitment and with investigation of a rare outcome
(28). Cohort studies may yield useful data, especially studies with a larger sample size, which would allow for subgroup analysis. Such analyses may be possible if self-harm was monitored nationally, as recommended in the National Suicide Prevention Strategy. Prospective studies of patients with near-fatal self-harm may also be useful, although defining near-fatal self-harm is problematic
(29).
Our findings may help clinicians identify vulnerable individuals. The clinician should be cognizant of the likelihood that a suicidal process may be triggered in a vulnerable individual who has experienced a negative life event, such as relationship breakup or a self-imposed deadline that has come and gone without resolution. We do not have data on the condition of the person at the time of the suicide, but psychological autopsy could be used to obtain an in-depth picture of service delivery and antecedents of suicide in patients who have presented to an emergency department after an episode of self-harm. A multicenter research design would provide sufficient power to the study within a short enough time frame to minimize recall bias.