Although diagnostic crossover to bulimia nervosa often occurs in patients with anorexia nervosa, our ability to predict crossover is limited
(1–
4). Antecedent overanxious disorder, childhood sexual abuse, and recovery from anorexia nervosa have been associated with crossover from anorexia nervosa to bulimia nervosa
(1). One study
(4) examined a range of predictors of the emergence of binge-eating in individuals with the restricting subtype of anorexia nervosa. Ten to 15 years after anorexia nervosa onset, hostile attitudes toward family and lack of parental expressed empathy/affection were the strongest predictors of binge eating onset. This study explored only predictors of the emergence of the symptom of binge eating and not predictors of the emergence of frank bulimia nervosa. However, of the 95 patients who entered the treatment program for restricting-type anorexia nervosa, 29% developed binge eating during the follow-up, of whom about 65% developed a full bulimia nervosa syndrome. Studies of crossover from bulimia nervosa to anorexia nervosa are rarer, have generally included small numbers of participants (mean N=77, range=30–196), and suggest a lower rate of occurrence (0%–4%) than has been observed for crossover from anorexia nervosa to bulimia nervosa
(13,
19–24). To our knowledge, no data exist regarding predictors of crossover from bulimia nervosa to anorexia nervosa.
To our knowledge, the present study represents the first attempt to study crossover both from anorexia nervosa to bulimia nervosa and from bulimia nervosa to anorexia nervosa. We explored variables previously shown either to be associated with crossover from anorexia nervosa to bulimia nervosa or to differentiate women with anorexia nervosa from those with bulimia nervosa.
Method
Participants
Participants were from the International Price Foundation Genetic Study of bulimia nervosa
(35). Probands and affected relatives were assessed for psychological and personality features that are associated with, and may underlie vulnerability to, eating disorders. Probands and biological relatives affected with anorexia nervosa, bulimia nervosa, or eating disorder not otherwise specified were recruited from 10 sites (Pittsburgh [W.H.K.], New York [K.A.H.], Los Angeles [M.S.], Toronto [A.S.K., D.B.W.], Munich [M.M.F.], Philadelphia [W.H.B.], Pisa [G.C., M.M., A.R.], Fargo [J.M.], Minneapolis [S.C.], and Boston [P.K.]). Informed consent was obtained from all participants, and all sites received approval from their institutional review boards.
Screening and Diagnostic Procedures
If—in an initial screening—a proband met the criteria for bulimia nervosa, had no exclusion criteria (see next paragraph), and reported a possible history of an eating disorder in a nonparent, nonchild, or a nonmonozygotic twin blood relative, the proband was asked to discuss the study with the affected relative and obtain permission to be contacted by study personnel. If both the proband and affected relative met the inclusion criteria, informed consent was obtained and both were scheduled to complete assessments. If participants lived near one of the study sites, interviews were completed in person. Others were interviewed by phone.
The participants for this study included both probands and affected relatives. Probands met the following criteria: 1) modified DSM-IV lifetime diagnosis of bulimia nervosa, purging type (purging must have included regular vomiting [with other means of purging allowed], and bingeing and vomiting must have occurred at least twice a week for a duration of at least 6 months) and 2) ages between 13 and 65 years. The exclusion criteria for probands were mental retardation (IQ <70); dementia; organic brain syndromes; psychotic disorders, including schizophrenia, schizophreniform disorder, delusional disorder, and schizoaffective disorder; Turner’s syndrome; any medical condition that could affect appetite, body weight, or eating (e.g., individuals with diabetes and thyroid conditions were excluded if the onset of the disease preceded the onset of the eating disorder); bipolar I disorder or bipolar II disorder only if symptoms of bulimia nervosa occurred exclusively during manic or hypomanic episodes; and neurological problems, except for participants with a diagnosis of a seizure disorder resulting from trauma after the onset of the eating disorder. Probands whose premorbid weight exceeded the body mass index for the 95th percentile for gender and age on the Hebebrand index (36) or whose high lifetime body mass index was greater than 35 kg/m2 were also excluded.
Affected relatives were biological family members who 1) were between ages 13 and 65 years and 2) met the criteria for lifetime bulimia nervosa, purging type or anorexia nervosa, restricting type. The eating disorder diagnoses for the relatives were defined as follows: 1) DSM-IV bulimia nervosa, purging type, and 2) modified DSM-IV anorexia nervosa (i.e., criterion D not required). To be defined as having persistent restricting-type anorexia nervosa, participants had to have never binged or purged except experimentally (defined as less than five times ever). The exclusion criteria for affected relatives included those for probands plus 1) being a monozygotic twin of the proband; 2) being a biological parent with an eating disorder, unless there was another affected family member with whom the parent could be paired; and 3) having a diagnosis of binge-eating disorder as the only lifetime eating disorder diagnosis.
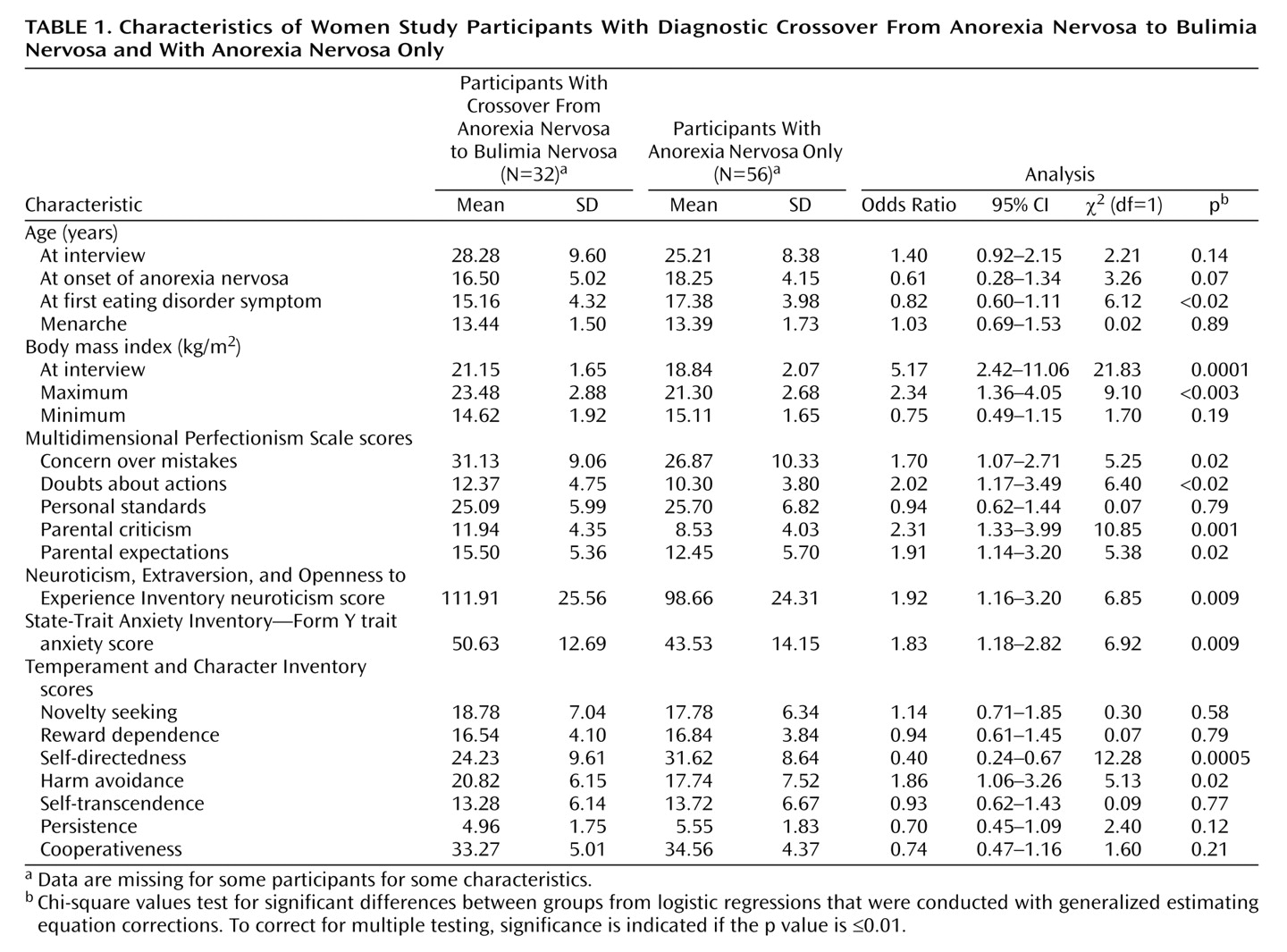
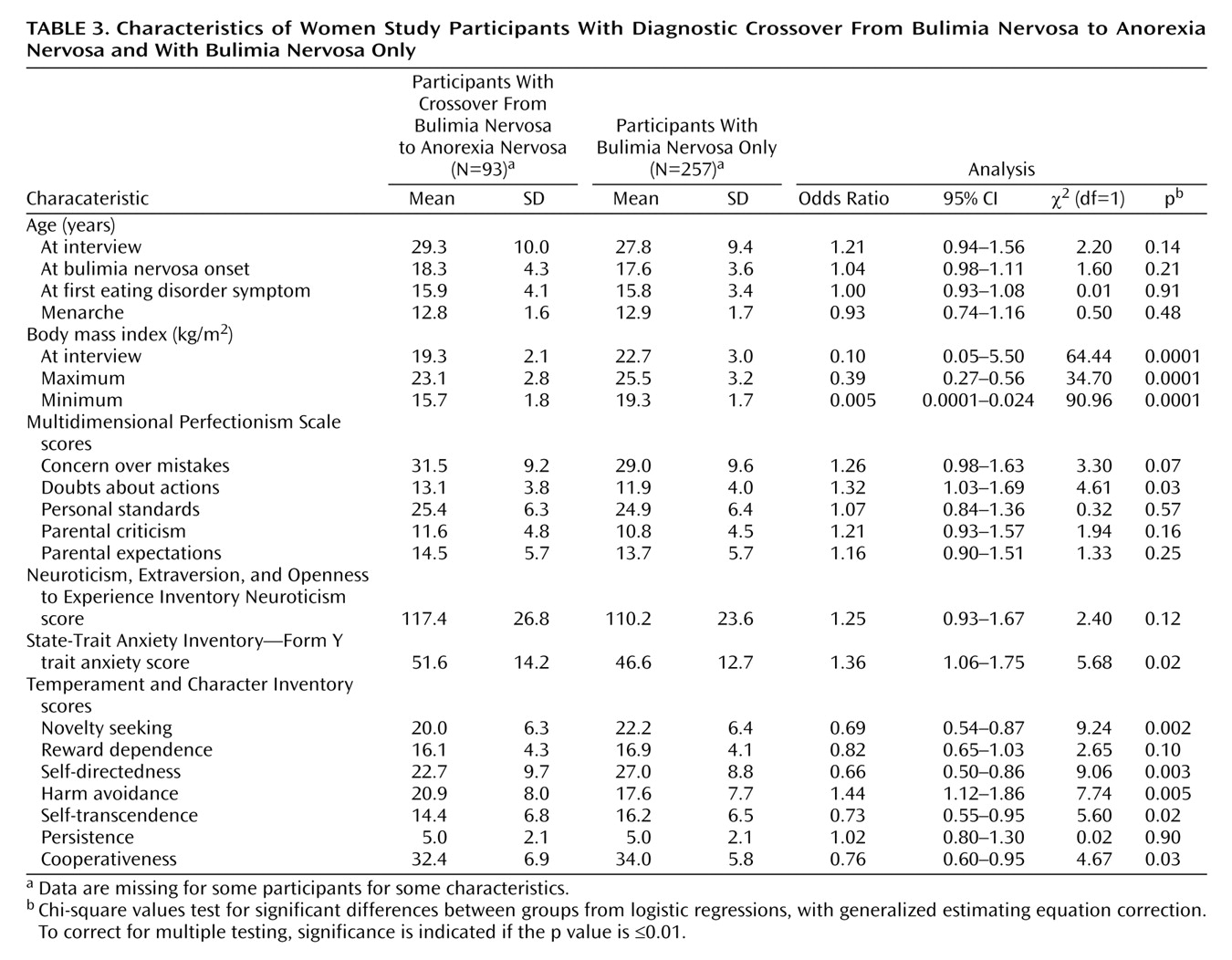
We conducted two series of analyses. First, to explore crossover from anorexia nervosa to bulimia nervosa, we compared 1) individuals with persistent restricting-type anorexia nervosa (N=56) and 2) individuals with an initial diagnosis of restricting-type anorexia nervosa who developed bulimia nervosa (N=32). Second, to explore crossover from bulimia nervosa to anorexia nervosa, we compared individuals who met the criteria for a diagnosis of 1) persistent normal weight bulimia nervosa, purging type (N=257) and 2) individuals who initially had normal weight bulimia nervosa followed by the development of anorexia nervosa, binge-eating/purging type (N=93). As a result of the recruitment procedure (i.e., probands had to have bulimia nervosa), all individuals with a diagnosis of anorexia nervosa were affected relatives, and all individuals with bulimia nervosa or both diagnoses were either probands or affected relatives.
Male participants were excluded from analyses, as the number of male participants with these diagnoses was too small for meaningful comparison. We were unable to examine other types of crossover (e.g., normal weight bulimia nervosa to restricting-type anorexia nervosa) because of the low frequency of these crossover types.
Measures
Physical characteristics
We evaluated self-reported current, past minimum, and past maximum body mass index (kg/m2) and age at menarche.
Eating disorder psychopathology
The Structured Interview for Anorexic and Bulimic Disorders for DSM-IV and ICD-10
(37) was used to assess specific and general psychopathology of eating disorders and lifetime history of eating disorders among probands and relatives.
Psychiatric diagnoses
The Structured Clinical Interview for DSM-IV (SCID) Axis I and Axis II Disorders
(38,
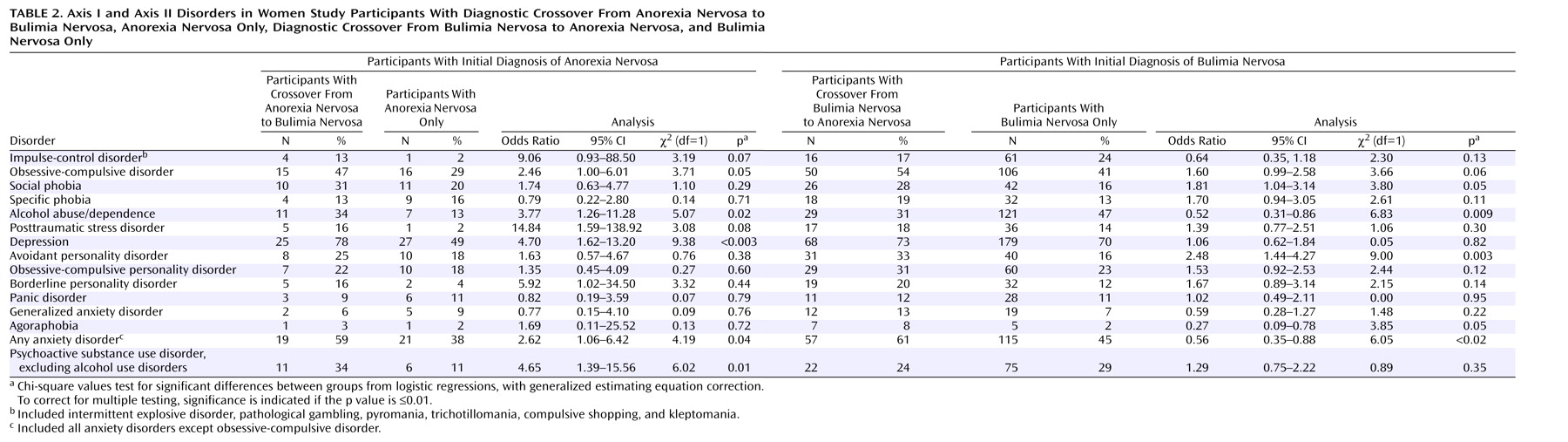
39) was used to assess lifetime axis I and axis II diagnoses. Among axis I diagnoses, we excluded bipolar I disorder and bipolar II disorder, because the frequencies were too low among the study participants. Impulse-control disorders (intermittent explosive disorder, pathological gambling, pyromania, trichotillomania, compulsive shopping, and kleptomania) were grouped together as an umbrella impulse-control disorder diagnosis. Among axis II diagnoses, we included only those disorders with adequate frequency, including avoidant, obsessive-compulsive, and borderline personality disorder. Lifetime diagnoses of eating disorders were determined by using information from both the Structured Interview for Anorexic and Bulimic Disorders and the SCID.
Perfectionism
The Multidimensional Perfectionism Scale
(40) is designed to assess multidimensional facets of perfectionism. Although the instrument includes six subscales, we included only those subscales that have been shown to be most relevant to eating disorders, including concern over mistakes, doubts about actions, personal standards, parental criticism, and parental expectation.
Temperament and character
Temperament, as measured by the Temperament and Character Inventory
(41), is postulated to be largely biological in origin
(42,
43) and to include the dimensions of novelty seeking, harm avoidance, reward dependence, and persistence. Character dimensions on the Temperament and Character Inventory are thought to develop with experience
(41) and include self-directedness, cooperativeness, and self-transcendence.
Anxiety
Although the State-Trait Anxiety Inventory—Form Y
(44) measures two aspects of anxiety (i.e., state and trait anxiety), we included only the trait anxiety scale in the present analyses.
Neuroticism
The present analysis included data from the neuroticism scale of the Neuroticism, Extraversion, and Openness to Experience Inventory
(45), as neuroticism has been consistently associated with eating disorders
(46,
47), particularly a bulimic symptom presentation
(48,
49).
Statistical Analyses
Logistic regressions with generalized estimating equation
(50–
52) corrections for dependent data were used to predict crossover. As status of illness (i.e., acutely ill or recovered) can influence scores on personality measures
(53), this variable was included in the models as a covariate. Women were considered recovered if they had an absence of eating disorder behaviors (e.g., binge eating, purging, dieting, nonpurging behaviors) for a period of at least 1 year, as reported on an expanded version of Module H of the SCID
(38). In addition, women with anorexia nervosa had to have their body mass index above the fifth percentile of their ideal body mass index for their age for at least the past year.
Variables that emerged in the initial logistic regressions as significantly associated with crossover were then entered into a stepwise logistic regression. All continuous measures were standardized before the analyses to have a mean of zero and unit variance. Given that we performed multiple statistical tests, we set the significance level to p≤0.01, representing a compromise between the more stringent Bonferroni correction and the exploratory nature of this study.
Discussion
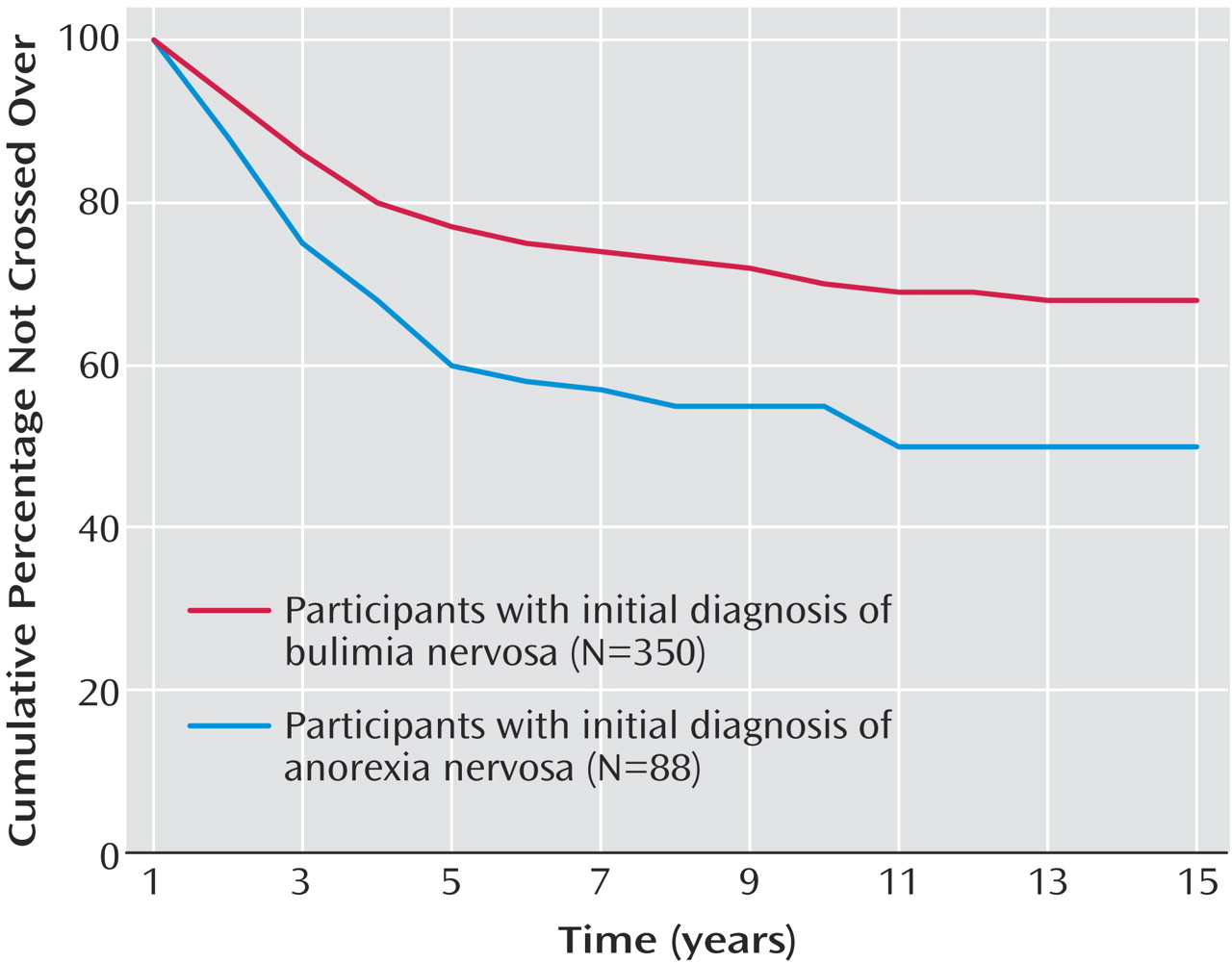
This study is, to our knowledge, the first to examine crossover both from anorexia nervosa to bulimia nervosa and from bulimia nervosa to anorexia nervosa. Supporting previous research, we observed that for most individuals, crossover occurred by the fifth year of illness. The crossover rate was higher for anorexia nervosa to bulimia nervosa than for bulimia nervosa to anorexia nervosa. However, the proportion of individuals with bulimia nervosa who eventually developed anorexia nervosa (27%) was substantially higher than previously reported rates (0%–4%)
(13,
19–
21,
23,
24). These results suggest that there is an elevated risk for diagnostic crossover in individuals with both anorexia nervosa and bulimia nervosa but that the clinical course tends to stabilize by the fifth year of illness.
Low self-directedness was consistently associated with both types of diagnostic crossover. This finding suggests that self-directedness may be a general character trait that influences the course of the eating disorder illness; individuals with low self-directedness, independent of diagnosis, may be characterized by an inability to regulate behaviors and affect adequately. This instability may then lead to alternations between the cognitive and behavioral restraint common to restricting-type anorexia nervosa and the disinhibition present in bulimia nervosa.
However, the relation that emerged in our study between low self-directedness and crossover may also be the result of an indirect association of self-directedness with other factors characteristic of individuals with eating disorders with fluctuating clinical features. For example, low self-directedness has been associated with greater comorbidity
(54,
55) and a poorer outcome
(9). Consequently, it may be that individuals with diagnostic crossover represent cases with greater comorbidity in which additional eating disorder diagnoses simply reflect greater psychopathology in general.
Whereas low self-directedness appeared to be a common factor characterizing both types of crossovers, other factors were specifically related to each crossover type. Family factors, namely perceived parental criticism, were particularly salient for individuals with anorexia nervosa who crossed over to having bulimia nervosa. This finding is noteworthy given early observations of family environment across eating disorder subtypes, suggesting that families of individuals with bulimia tended to exhibit greater conflict and disorganization and less cohesion than families of those with anorexia nervosa
(56), that mothers of individuals with bulimia nervosa were reported to be more domineering and have higher expectations of their daughters than were control individuals
(57), and that women with bulimia nervosa reported maternal deficits in nurturance and empathy
(58). Our findings also corroborate those of Strober et al.
(4), who found low levels of parental empathy and affection to be significant predictors of the onset of binge eating in women with anorexia nervosa. These observations are particularly noteworthy, given the finding in expressed emotion research that maternal critical comments are strongly predictive of treatment outcome for adolescents with eating disorders
(59).
Low scores on impulse-related personality traits (e.g., novelty seeking) and the presence of certain behaviors (e.g., alcohol abuse/dependence) were important in crossover from bulimia nervosa to anorexia nervosa. Lower levels of impulsivity may enable the maintenance of rigid dietary regimes of sufficient duration to lose the amount of weight necessary for an anorexia nervosa diagnosis.
We did not find anxiety, neurotic personality traits, or depression to be significantly associated with crossover in the hierarchical models, although they were often significant predictors in univariate analyses. These findings are somewhat contradictory to previous observations of anxiety as an important predictor of crossover from anorexia nervosa to bulimia nervosa
(1). However, earlier studies used different instruments and methods and are not entirely comparable to the current study.
Although our study had many strengths (e.g., carefully defined diagnostic phenotypes, examination of a range of variables), several limitations should be noted. First, we were unable to examine all possible diagnostic crossovers (e.g., purging-type bulimia nervosa to restricting-type anorexia nervosa) because some were rare. Future research should examine whether similar types of predictors also characterize these diagnostic changes. Second, participants may not have reached the “steady state” of their illness. Approximately 57% of the anorexia nervosa participants and 38% of the bulimia nervosa participants were interviewed before the fifth year of illness. Therefore, additional crossovers that were not captured in the present analyses could still occur.
Third, few details were available about changes in severity of illness over time (e.g., periods of partial or full recovery between anorexia nervosa and bulimia nervosa onset). These data would have provided a more comprehensive picture of the course of eating disorders and may have revealed additional correlates of diagnostic instability. Fourth, data about childhood psychiatric disorders or sexual abuse, which emerged as predictors of crossovers in previous studies
(1), were not available. Fifth, onset of diagnoses and determination of crossover were based on retrospective reports and may be subject to recall biases. However, the rate of crossover from anorexia nervosa to bulimia nervosa observed in our study was similar to that reported in longitudinal studies
(2–
4), suggesting that recall biases may have been minimal.
Finally, the study included individuals who had at least one family member with a disorder, which may have influenced the results. For example, we found a higher rate of crossover from bulimia nervosa to anorexia nervosa, compared with previous studies. Although this discrepancy might be related to the particular group of participants selected (e.g., all anorexia nervosa probands had a family member with bulimia nervosa), it could also be a more accurate reflection of true crossover rates, given that the number of participants was substantially larger than in previously reported studies. In addition, none of the cited studies, except for one
(1), had the specific goal of exploring the crossover phenomenon, and most of them were designed as longitudinal outcome studies. Thus, with respect to crossover, the earlier studies present limitations, such as lack of study groups strictly defined with respect to crossover (i.e., at recruitment, the bulimia nervosa group in these earlier studies may have included individuals with a history of anorexia nervosa). In addition, earlier studies reported rates of crossover that refer only to individuals who still had an eating disorder diagnosis at follow-up, and thus these studies did not explore possible crossovers before recovery. Moreover, we focused on crossovers between full syndromal anorexia nervosa and bulimia nervosa, whereas the majority of previous studies evaluated the development of bulimic behaviors, rather than the full bulimia nervosa syndrome, in individuals with restricting-type anorexia nervosa. Our study, although exploratory in nature, has the advantage of diagnostic rigor and specific attention to the crossover phenomenon. However, the extent to which our findings were biased by our recruitment procedures, rather than depicting an accurate association between bulimia nervosa and anorexia nervosa crossover, is unclear. Resolution of this issue awaits future research employing less select groups of participants that parallel the group in our study in size and diagnostic characterization.
In summary, this study furthers our understanding of diagnostic crossover in eating disorders by suggesting that there are features, such as self-directedness, that affect general diagnostic instability, while there are other factors specifically related to the initial eating disorder diagnosis that influence crossover in one direction but not the other. If findings from this exploratory study are confirmed, they may have important treatment implications. Low self-directedness has been associated with negative outcome
(9,
60,
61). Indeed, high self-directedness predicts rapid and sustained response to cognitive behavior therapy in bulimia nervosa patients
(62), and there is evidence that cognitive behavior therapy leads to increased self-directedness
(63). Thus, self-directedness may influence not only the diagnostic stability of eating disorders but also their course and response to treatment. The development of additional therapeutic approaches aimed at increasing levels of self-directedness may enhance the efficacy of existing treatments. Additional techniques aimed at enhancing familial communication in cases of anorexia nervosa and at addressing impulsivity in bulimia nervosa are also likely to promote diagnostic stability and possibly shorter recovery times.