Angular and supramarginal gyri form the inferior parietal lobule, a heteromodal association neocortical region that is part of the neuroanatomical circuitry for language comprehension
(1). Consistent with their role in language, these structures are left-lateralized
(2), and functional neuroimaging studies
(3) show lateralized activation of these areas in normal subjects performing language tasks. Such functional lateralization appears to be diminished in schizophrenia
(4).
Volume reductions in the inferior parietal lobule
(5) and supramarginal gyrus
(6) have been reported in schizophrenia. Moreover, reversal of the normal left-greater-than-right angular gyrus asymmetry has been reported in chronic schizophrenia
(7,
8), consistent with the notion that abnormalities of normal hemispheric asymmetry are the primary neurogenetic deficit in schizophrenia
(9). We examined first-episode schizophrenia subjects to assess whether angular gyrus volume and asymmetry abnormalities were present at the first hospitalization.
Method
Twelve male and two female patients with a DSM-III-R diagnosis of schizophrenia were recruited within 3.5 months of their first hospitalization (mean time from admission to study scan=25.5 days). The majority of diagnoses were confirmed at 1.5-year follow-up. Our local institutional review board approved this study, and all participants provided written informed consent. Twelve male and two female comparison subjects, group-matched for age and parental socioeconomic status, were recruited through newspaper advertisements. Comparison subjects were screened for DSM-III-R-defined axis I or axis II psychiatric disorders. All subjects were right-handed, were 18–55 years of age, had IQs above 75, and had no history of seizure, head trauma with loss of consciousness, neurological disorder, or alcohol/drug dependence.
The Mini-Mental State Examination (MMSE) and WAIS-R
(10) were administered to all subjects. Handedness
(11) and socioeconomic status (subject and parental)
(12) were assessed. In patients, the Brief Psychiatric Rating Scale (BPRS) was used to quantify psychosis. Duration of psychotropic medication use before magnetic resonance imaging (MRI) scan was brief (one patient was receiving no antipsychotic medication at time of study). Daily chlorpromazine equivalents did not correlate significantly with MRI volumes.
MRI acquisition and postprocessing methods are detailed elsewhere
(13). Briefly, 124 T
1-weighted 1.5-mm contiguous coronal slices were obtained with a 1.5-T scanner (GE Medical Systems, Milwaukee); 3-mm axial dual-echo images were also acquired. The latter were registered to T
1 images, and information from both was used to classify voxels automatically into gray matter, white matter, and CSF.
For region of interest measurements, T
1 images were realigned and rotation measures were applied to segmented images, which does not alter region of interest volumes
(13). Tilt-corrected segmentations were edited slice-by-slice. Regions of interest were gray matter of the postcentral, supramarginal, and angular gyri. Coronal, axial, and sagittal views were used to determine gyral boundaries to facilitate precise localization of sulcal landmarks. An anatomical atlas was used to determine boundaries, consistent with methods reported elsewhere
(7,
14). The complete parcellation method is available on request. Interrater reliability was assessed among three raters, blind to diagnosis, and five cases. Intraclass correlation coefficients for the postcentral, supramarginal, and angular gyri were 0.97, 0.98, and 0.98, respectively.
Results
No group differences in age, handedness, parental socioeconomic status, MMSE scores, WAIS-R scores, or intracranial volume were found (t tests). The patients with first-episode schizophrenia showed significantly lower socioeconomic status than comparison subjects, consistent with reduced premorbid functioning.
Repeated-measures analysis of variance (ANOVA) was performed with one between-group variable (diagnosis) and two within-group variables (side and region). Comparisons of regions used relative gray matter volumes (absolute volumes/intracranial volumes), and measures were converted to z scores to eliminate the effect of absolute volume differences across regions of interest. Overall ANOVA revealed a significant group-by-hemisphere-by-region interaction (F=3.36, df=2, 52, p=0.04), suggesting regional laterality differences between groups. Follow-up ANOVA showed a significant group-by-side interaction for the angular gyrus (F=7.80, df=1, 26, p=0.01) but not for the supramarginal gyrus (F=1.14, df=1, 26, p=0.30) or postcentral gyrus (F=0.04, df=1, 26, p=0.86).
Paired t tests were used to assess volume asymmetries.
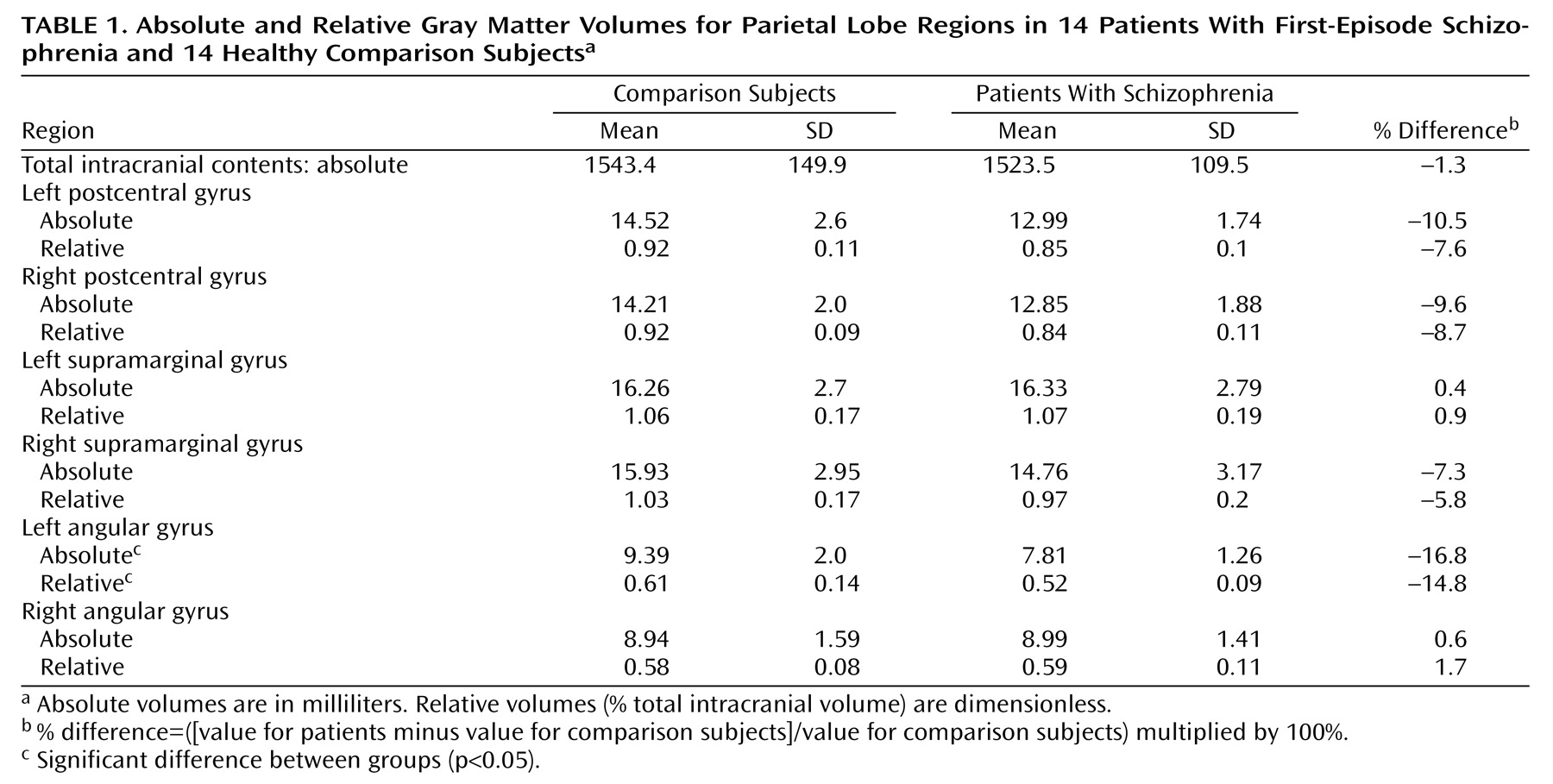
Table 1 shows absolute and relative regional gray matter volumes. In the left angular gyrus, both absolute (t=2.50, df=26, p=0.02) (16.8% less) and relative (t=2.25, df=26, p=0.03) (14.8% less) volumes were smaller in patients with schizophrenia than in comparison subjects. Groups did not differ in gray matter volumes of the right angular gyrus, whether absolute (t=0.09, df=26, p=0.93) or relative (t=0.44, df=26, p=0.67) volumes were compared. Differences in asymmetric angular gyrus volume were present whether intracranial volume was used as a covariate or not. Comparison subjects showed a nonsignificant leftward asymmetry in angular gyrus (paired t=1.05, df=13, p=0.31), but patients with schizophrenia showed a larger right-greater-than-left volume asymmetry (paired t=–3.53, df=13, p=0.004).
Regional asymmetry coefficients ([(left minus right)/(left plus right)] multiplied by 100) were similarly analyzed. ANOVA for asymmetry coefficients showed marginal regional differences in asymmetry (F=3.11, df=2, 52, p=0.05) and a region-by-group interaction (F=4.61, df=2, 52, p=0.01). Only the angular gyrus showed significant group differences (t=–2.46, df=26, p=0.02). To assess whether this difference was related to other regional asymmetries, we examined Pearson correlations between asymmetry coefficients for the angular gyrus and planum temporale for 21 of 28 subjects from previous analyses. This correlation was significant when the groups were pooled (r=0.49, N=21, p=0.02).
We found no relation between patients’ angular gyrus volumes or asymmetry coefficients and their BPRS thought disturbance factor (paranoia, hallucinations, or delusions).
Discussion
Patients experiencing their first hospitalization for schizophrenia showed a large rightward asymmetry in the angular gyrus, due to significantly reduced left angular gyrus gray matter volume. Parietal lobe gray matter abnormalities were specific to the angular gyrus. This finding is consistent with other reports of parietal lobe abnormalities in chronic schizophrenia
(5,
6), including reversal of left-greater-than-right inferior parietal lobule asymmetry
(6,
7), localized to the angular gyrus
(8). The present study extends earlier studies in chronic schizophrenia to patients experiencing their first episode of psychosis, where findings are not the result of chronic illness or factors related to long-term treatment.
It remains unclear when and why these inferior parietal lobule abnormalities develop. Crow
(9) hypothesized that genetic determinants of cortical asymmetry represent the primary prenatal abnormality in schizophrenia. Altered angular gyrus asymmetry, as noted here, is consistent with this etiology. An alternative hypothesis is that polymodal association cortices, particularly left posterior perisylvian language areas, which include the angular gyrus, undergo a process of degeneration in late adolescence at or near the time of first hospitalization for schizophrenia
(15).
We also found correlations between asymmetry measures for the angular gyrus and planum temporale, part of the superior temporal gyrus. Superior temporal and angular gyri are part of the left-hemisphere language network. Previous work from our laboratory revealed that the planum temporale had reversed asymmetry at first hospitalization
(13,
15). Together, these data suggest that both chronic and first-episode schizophrenia are characterized by abnormal asymmetry present in brain regions involved with semantic processing (the angular gyrus and planum temporale). Such abnormalities in the neural substrates for language and thinking are likely germane to the pathophysiology of schizophrenia
(9). The precise nature of this relationship and its etiological basis remain the subject of future research.