Objective: Quality improvement programs for depressed youths in primary care settings have been shown to improve 6-month clinical outcomes, but longer-term outcomes are unknown. The authors examined 6-, 12-, and 18-month outcomes of a primary care quality improvement intervention. Method: Primary care patients 13–21 years of age with current depressive symptoms were randomly assigned to a 6-month quality improvement intervention (N=211) or to treatment as usual enhanced with provider training (N=207). The quality improvement intervention featured expert leader teams to oversee implementation of the intervention; clinical care managers trained in cognitive-behavioral therapy for depression to support patient evaluation and treatment; and support for patient and provider choice of treatments. Results: The quality improvement intervention, relative to enhanced treatment as usual, lowered the likelihood of severe depression (Center for Epidemiological Studies Depression Scale score ≥24) at 6 months; a similar trend at 18 months was not statistically significant. Path analyses revealed a significant indirect intervention effect on long-term depression due to the initial intervention improvement at 6 months. Conclusions: In this randomized effectiveness trial of a primary care quality improvement intervention for depressed youths, the main effect of the intervention on outcomes was to decrease the likelihood of severe depression at the 6-month outcome assessment. These early intervention-related improvements conferred additional long-term protection through a favorable shift in illness course through 12 and 18 months.
Major depression is predicted to become the second leading cause of disability in the world by 2020 (1) . Depression is one of the most common mental health problems among adolescents and is associated with increased morbidity and mortality: 10%–15% of youths are estimated to suffer from major depression by age 18, 28.3% of high school students report periods of impairing depression during the past year, and youth depression is associated with an increased risk of suicide and suicide attempts, social impairments, substance abuse, and adult depression (2 – 4) .
Despite evidence of clinical and social morbidity and evidence of effective treatments, many depressed youths go untreated, and outcomes for depression treatment as delivered in routine clinical settings appear poor, with a meta-analysis suggesting a mean effect size near zero (5) . This state of affairs has underscored the need to identify effective strategies for delivering evidence-based care within practice settings and to understand the outcome consequences.
Primary care is a major point of health service contact for youths and offers valuable opportunities to improve depression care (6, 7) . Quality improvement interventions aimed at increasing rates of evidence-based depression care for adults in primary care have resulted in significant improvements in short- and long-term outcomes (7 – 11) . However, rates of detection and treatment of depression are low for youths in primary care settings, and research evaluating quality improvement in youth populations has just begun (6, 7) . Efficacy studies for adolescent depression treatment suggest that evidence-based psychotherapies, such as cognitive-behavioral therapy (CBT), are effective (4, 12) . Despite controversies over antidepressant medication in terms of both modest effects relative to adult studies and concerns about an increased risk of suicidality, the research supports the efficacy of fluoxetine and combined treatment with medication and CBT for moderate to severe depression in adolescents (4, 13 – 15) . Few studies of depression treatment in adolescents have included long-term outcome data, and it has been difficult to demonstrate long-term benefits from depression treatments in youths, given the high natural recovery rate in this population (16 – 18) .
The Youth Partners in Care study is a large randomized controlled trial designed to evaluate the effectiveness of a quality improvement intervention for depression, relative to treatment as usual enhanced by provider education, for depressed primary care patients 13–21 years of age (19) . The intervention was a 6-month quality improvement program designed to improve access to evidence-based CBT and antidepressant medication through primary care. The study was initiated prior to controversies over the risk of suicidality in youths on some antidepressant medications (14) . To support feasibility in primary care settings, depression status was assessed using a brief screening instrument that could be completed while patients waited for the primary care visit. As a result, some youths screened positive, meeting criteria for depressive disorders, and others had subsyndromal depressive symptoms. We previously reported short-term outcomes (19), which indicated significant advantages of the intervention relative to treatment as usual, on depression outcomes, quality of life, and satisfaction with mental health care at 6-month follow-up. Patients in the intervention group also reported increased rates of specialty mental health care, particularly psychotherapy or counseling, with no evidence for increased use of antidepressant medications.
In this study, we examined effects of the Youth Partners in Care intervention on process and outcomes of care through 18 months and considered evidence for an indirect long-term outcome effect through the early effects on depression observed at 6 months. Direct effects are attributable to factors that the intervention directly changed, such as increased treatment rates and satisfaction with care (19) . Direct effects might be expected at 12 and 18 months if the intervention led to longer-term change in patterns of treatment use by patients or treatment delivery providers or to persistent change in behaviors that were the direct focus of therapy. An indirect effect is an influence of the intervention on outcome through an intermediate factor. For example, indirect intervention effects on 18-month outcomes could occur if the relief of depression due to the intervention at 6 months reduced clinical risk factors for chronic or recurrent depression or stimulated other behavioral changes that were not the direct focus of therapy but nevertheless lowered the risk for later depression. Based on previous studies indicating that the benefits of depression treatment in youths are most evident early (16 – 18, 20), we hypothesized 1) that direct effects of the intervention on outcomes would be strongest at the 6-month postintervention evaluation, and 2) that there would be an indirect intervention effect on 18-month outcomes through a continuing effect of the improvement in depression outcomes at 6 months. We also explored indirect quality improvement effects on quality-of-life outcomes.
Method
The Youth Partners in Care study is a multisite randomized effectiveness trial comparing the quality improvement intervention with an enhanced treatment-as-usual control group. The study protocol was approved by the institutional review boards from all participating organizations. After being given a complete description of the study, all participants, as well as legal guardians for youths under age 18, provided informed consent or assent. Because the study design is described elsewhere (19, 21), we provide only a brief overview below.
Sample and Design
Six study sites were selected from five health care organizations to include public sector (two sites), managed care (two sites from one organization), and academic health programs (two sites). Participants were recruited and enrollment eligibility determined through in-clinic screenings of a consecutive sample of patients using brief self-administered questionnaires. Eligibility criteria were either a score ≥24 on the Center for Epidemiological Studies Depression Scale (CES-D; 22) or endorsement of “stem items” for major depression or dysthymia from the 12-month Composite International Diagnostic Interview (CIDI), modified slightly to conform to diagnostic criteria for adolescents, 1 week or more of past-month depressive symptoms, plus a CES-D score ≥16. Following common adolescent medicine practices (23), we defined adolescence broadly to include youths up to age 21. Patients were eligible for inclusion if they were 13–21 years of age and presented at one of the clinic sites for a primary care visit. Patients were excluded if they had previously completed the screening instrument, if they did not speak English, if their provider was not in the study, or if they had a sibling in the study.
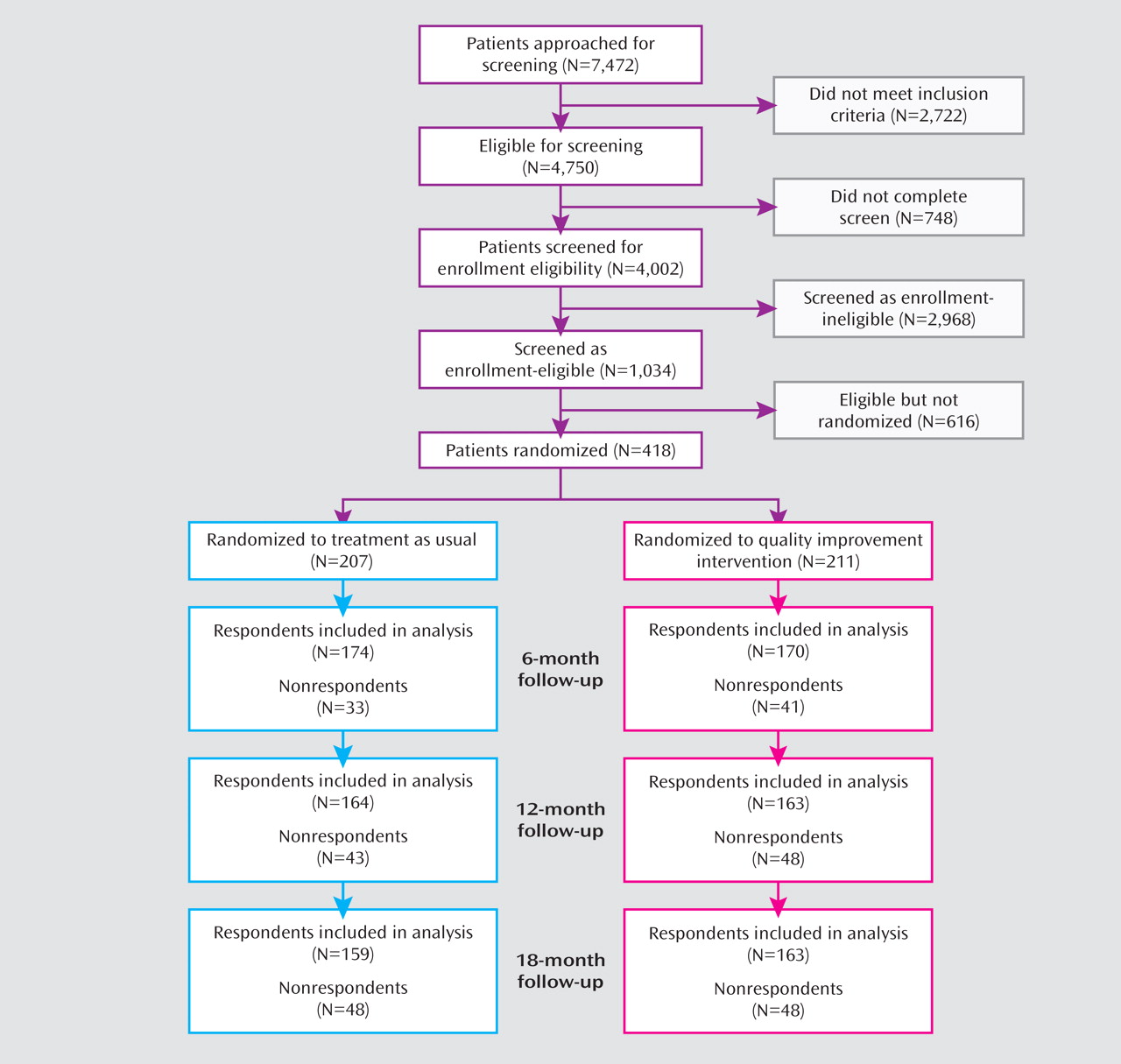
Of 4,750 youths eligible for screening, 4,149 began and 4,002 completed the screening instrument ( Figure 1 ). Of the 1,034 youths who met eligibility criteria, 418 completed baseline assessments and were randomly assigned to the intervention or treatment-as-usual condition. To improve balance across conditions in terms of provider mix and patient sequence, we stratified participants by site and provider. Screening and enrollment staff and assessment staff were blind to randomization status and sequence.
Figure 1. Flowchart of Patients’ Progress Through Study ProtocolOpen in viewer
Among the 418 youths enrolled, 380 (90.9%) participated in more than one follow-up evaluation, 344 (82%) participated in the 6-month assessment, 327 (78.2%) participated in the 12-month assessment, and 322 (77.0%) participated in the 18-month assessment ( Figure 1 ). At baseline 178 participants (42.6% of the sample) met CIDI criteria for depressive disorders; the remaining participants reported elevated depressive symptoms but did not meet the threshold for major depression or dysthymic disorder. Rates of baseline depressive disorders were similar for the intervention and treatment-as-usual groups (44% of the intervention group and 41% of the treatment-as-usual group).
Intervention Conditions
Treatment as Usual
Youths in the treatment-as-usual group had access to usual treatment at the site, but not to the specific mental health providers trained in the study CBT and care management services. Treatment as usual was enhanced by providing primary care physicians with 1–2 hours of training (24) and educational materials (manuals, pocket cards). The training emphasized evaluation strategies, depressive symptoms, common comorbid disorders and complicating conditions, and treatment strategies, particularly medication.
Quality Improvement Intervention
The intervention included 1) expert leader teams at each site to adapt and implement the intervention; 2) clinical care managers who supported providers with patient evaluation, education, pharmacological and psychosocial treatment, and linkage with specialty mental health services; 3) training for care managers in manualized CBT for depression; and 4) patient and provider choice of treatment modalities (CBT, medication, referral, and follow-up). The study informed providers about patient participation only in the intervention condition.
Care managers were psychotherapists with master’s or doctoral degrees in a mental health field or nursing. Spanish-speaking staff were available at two sites, and all other staff were non-Hispanic Caucasians. The study provided a 1-day training session on the study CBT and evaluation-and-treatment model, emphasizing culturally competent care and tailoring the intervention to the cultural context of each patient and family (25) . It also provided detailed manuals and consultation to support fidelity to the treatment model and provide case-specific training.
Patients in the intervention group—and their parents when appropriate—were offered an in-clinic care manager visit emphasizing evaluation, education about treatment options, and clarification of treatment preferences. A treatment plan was developed, finalized with the primary care provider, and modified when needed. Care managers followed patients for 6 months, supported the primary care provider, and delivered the CBT. The study CBT was based on the Coping With Depression Course (26, 27), which was developed for individual or group sessions and adapted to enhance feasibility within primary care. This manualized CBT (26) included an introductory session, three 4-session modules emphasizing different CBT components (activities/social skills, cognitions, communication/problem solving), and a final session emphasizing relapse prevention and follow-up care. The mean number of CBT sessions for patients receiving CBT was 3.85 (SD=3.69; range=1–16), based on case record review (21) . The Texas Medication Algorithms (28) guided medication treatment and emphasized selective serotonin reuptake inhibitors (SSRIs) as the first-stage medication choice. Further details about the intervention can be found elsewhere (19, 21) .
Assessment
Assessments were conducted by Battelle Survey Research Institute using computer-assisted telephone interviews and interviewers who were blind to intervention assignment. Continued attempts to contact participants were made until the participant declined to be interviewed or it became clear that he or she could not be reached. Interviewer training and supervision was by staff with official CIDI training. Ratings of interview quality (accuracy in presenting questions, probing, coding) conducted for 10% of interviews indicated good quality (on a 3-point scale with 1 as the highest rating, mean=1.02 [SD=0.06]).
Measures
The primary outcome variable was severe depression, defined on the basis of CES-D score: a score <24 was classified as response, and a score ≥24 (indicating severe depressive symptoms) was classified as nonresponse (19, 22) .
As a context for understanding the depression outcomes, we also had three secondary outcome variables. We examined mental health-related quality of life using the mental health summary score of the Medical Outcomes Study Short Form–12 health survey (29) ; satisfaction with care; and process of care (i.e., rates of mental health treatment) (19) .
Statistical Analyses
For analyses of main intervention effects on outcomes, we followed the intent-to-treat principle. Data for all randomly assigned participants were analyzed according to the experimental arm they were assigned to, regardless of whether patients in the intervention group received treatment or used study resources (such as care management and CBT) or those in the treatment-as-usual group received treatment through usual resources. Repeated-measures analyses were conducted to evaluate intervention effects over time. We fit regression models for continuous outcomes using SAS, version 9.1.3 (SAS Institute, Cary, N.C.) PROC MIXED, and logistic regression models for dichotomous outcomes using SAS GLIMMIX macro, using follow-up data at 6, 12, and 18 months. In the REPEATED statement, we specified autoregressive (AR[1]) covariance structure within subjects to account for the within-subject correlation over time. We treated time as a categorical variable and examined the fixed effects for time, intervention condition, and their interactions with regression adjustment for age, gender, ethnicity, the baseline measure for the same outcome, and study site. To show effect sizes, we present both unadjusted means and proportions by intervention groups and adjusted group differences and odds ratios calculated from the mixed effects models. These analyses were supplemented by a survival analysis examining the impact of the intervention on speed of recovery over the 18-month follow-up period, defined as the first assessment without severe depression (CES-D score <24), while controlling for censoring effects due to differential length of follow-up or recovery in a prior interval. These analyses used an extension of the life table method by the Kaplan-Meier method, as operationalized in SAS PROC LIFETEST. Because intervention effects were predicted to be more likely to occur in the early postintervention period, we tested for between-group differences in survival curves using the Wilcoxon statistic, a nonparametric rank test that more heavily weights earlier events in the survival distribution.
To explore the hypothesis that the intervention might have indirect effects on long-term outcomes, we used path analysis. The path model included a direct path from intervention to severe depression status at 18 months and a direct path from intervention to severe depression status at 6 months, and then to 12 and 18 months, reflecting indirect benefits of the early intervention. The model also included baseline depression, age, gender, ethnicity, and study site as covariates. The path model was estimated using a weighted least squares estimator and the probit link function with Mplus (30), using procedures recommended by Shrout and Bolger (31) . Because the path analysis combines analysis of randomized (intervention to 6- or 18-month outcomes) and nonrandomized (depression effects on subsequent depression) effects, it is considered an observational and exploratory analysis.
The criterion we set for statistical significance was a two-sided p value £0.05. We conducted sensitivity analyses by weighting nonresponse (32) to address missing data for 9% of patients with no follow-up assessments. Nonresponse weights were constructed by fitting logistic regression models to predict follow-up status from baseline clinical and sociodemographic characteristics. Separate models were fitted for each intervention group. The reciprocal of the predicted follow-up probability is used as the nonresponse weight for each participant. For analysis of repeated measures and path analysis, two parallel analyses were conducted with and without nonresponse weighting. Weighted and unweighted analyses yielded similar results. We report results from unweighted analyses.
Results
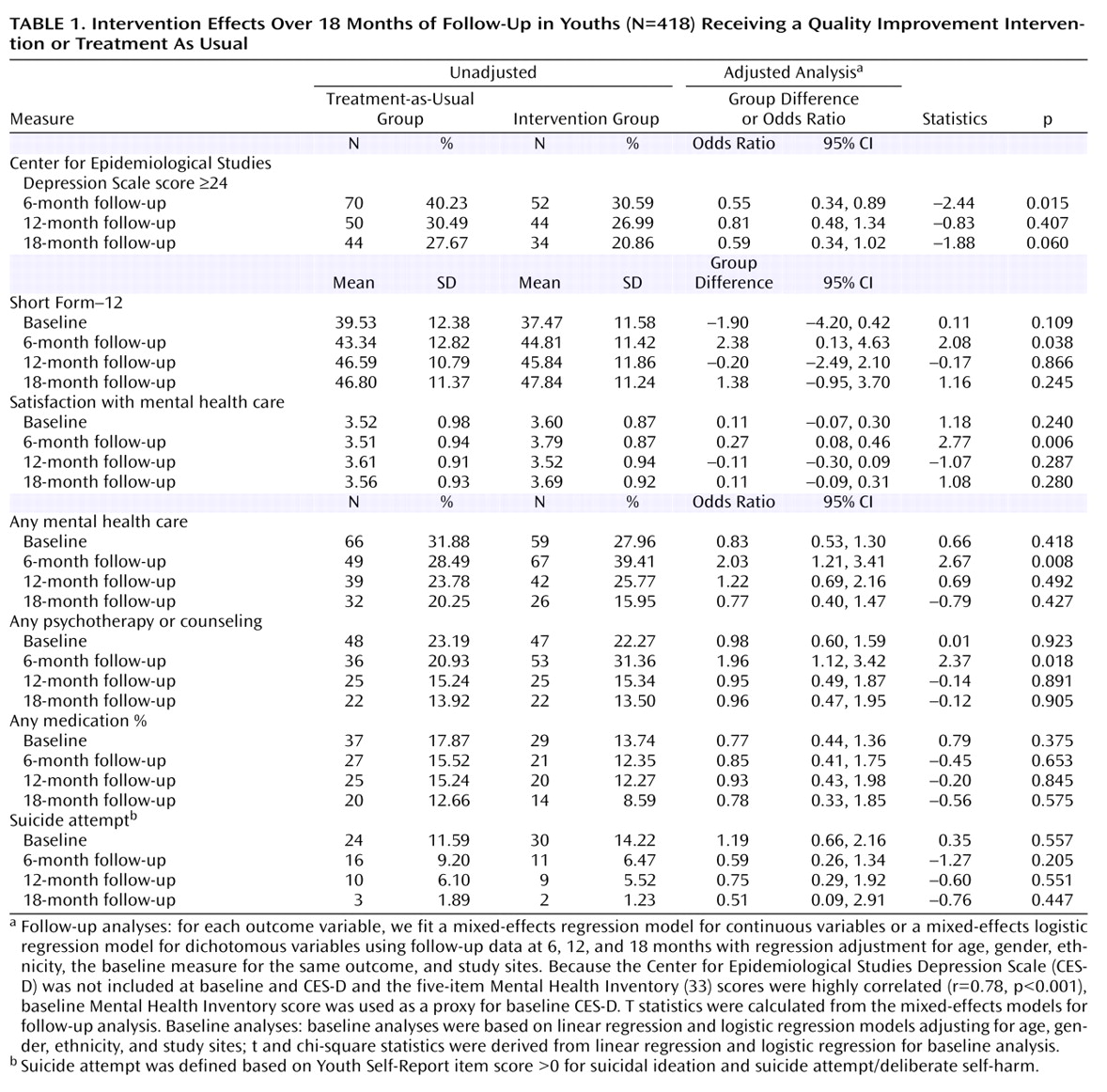
The sample was clinically and sociodemographically diverse. Most patients were female (78%) ethnic minorities (56% Hispanic or Latino; 13% African-American; 1% Asian; 17% other or mixed ethnicity). The sample included patients with depressive disorders (43%), primarily major depression (42%), and patients with subsyndromal depression (57%). There were no significant differences between the quality improvement and treatment-as-usual groups at baseline (see Table 1 ). The statistical analysis strategy differed in this paper from that used in the 6-month outcome paper (19) ; the results are similar but differ slightly in numerical value.
Results of mixed-model analyses ( Table 1 ) confirmed significant intervention effects on rates of severe depression at 6 months. The trend toward decreased rates of severe depression in the intervention compared with the treatment-as-usual group at 18 months did not reach statistical significance (p=0.06). Intervention effects on secondary outcomes (Short Form–12 mental health summary, satisfaction with care, rates of mental health treatment) were statistically significant only at the 6-month outcome point. Sensitivity analyses using the continuous CES-D score revealed statistically significant intervention effects only at 6 months. The study did not have sufficient statistical power to assess suicide attempt outcomes, and there were no statistically significant intervention effects on rates of suicidal ideation or suicide attempt. Attempt rates declined >50% in the intervention group at 6 months, but also declined in the treatment-as-usual group ( Table 1 ).
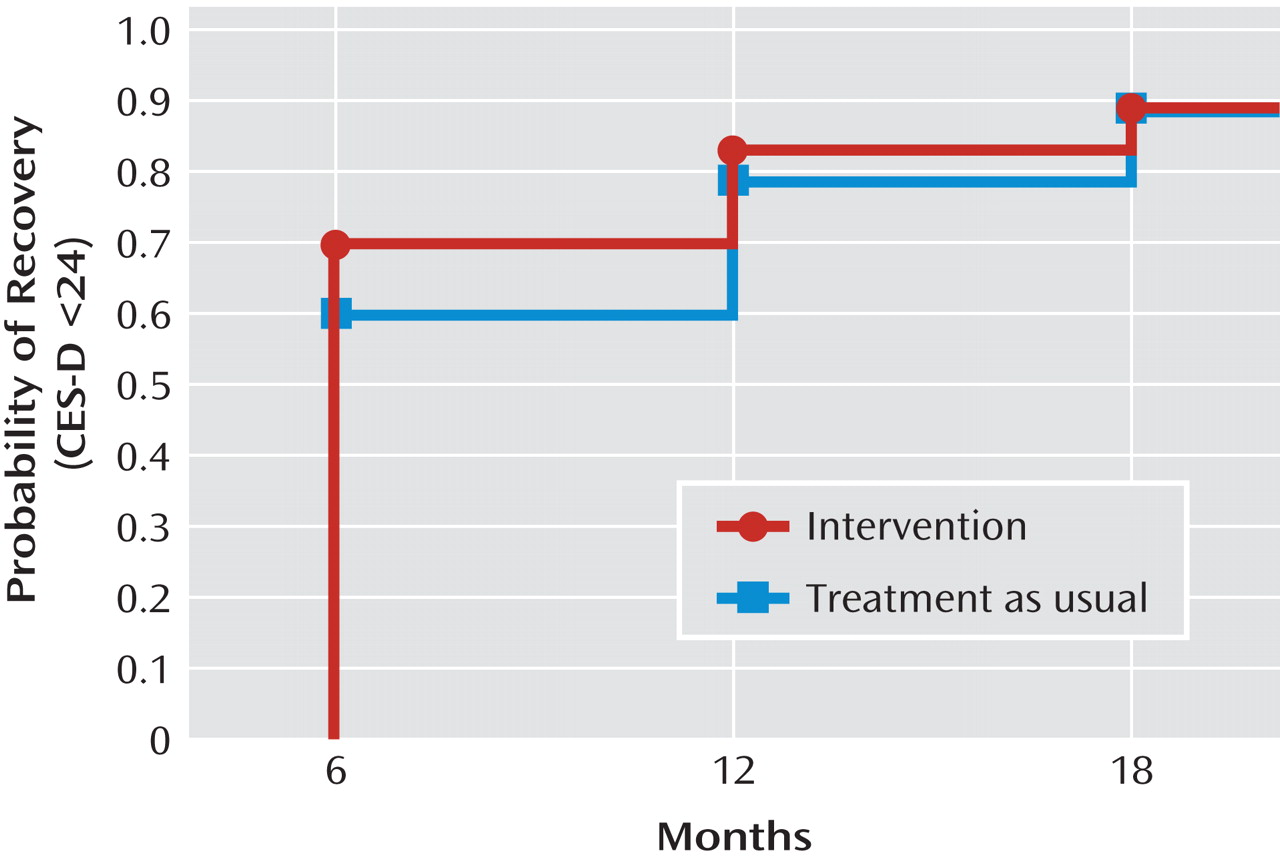
Figure 2 shows time to first recovery (CES-D score <24) over 18 months. The Kaplan-Meier survival analysis showed that the between-group difference in the estimated probability of initial recovery was roughly 10 percentage points at 6 months, 5 percentage points at 12 months, and zero at 18 months, with a 90% cumulative probability of recovery in each group over the 18-month follow-up period. Mean times to recovery were 8.76 months (SD=0.35) for the intervention group and 9.65 months (SD=0.37) for the treatment-as-usual group, suggesting a first recovery almost 1 month (27 days) earlier in the intervention group. Statistically significant between-group differences were seen only at 6 months (z=2.03, p=0.042). The overall trend toward faster recovery for the intervention group compared with the treatment-as-usual group over 18 months did not reach statistical significance (Wilcoxon χ 2 =3.60, p=0.058).
Figure 2. Kaplan-Meier Survival Analysis Time to First Recovery During 18 Months of Follow-Up a
a Recovery was defined as a score <24 on the Center for Epidemiological Studies Depression Scale (CES-D).
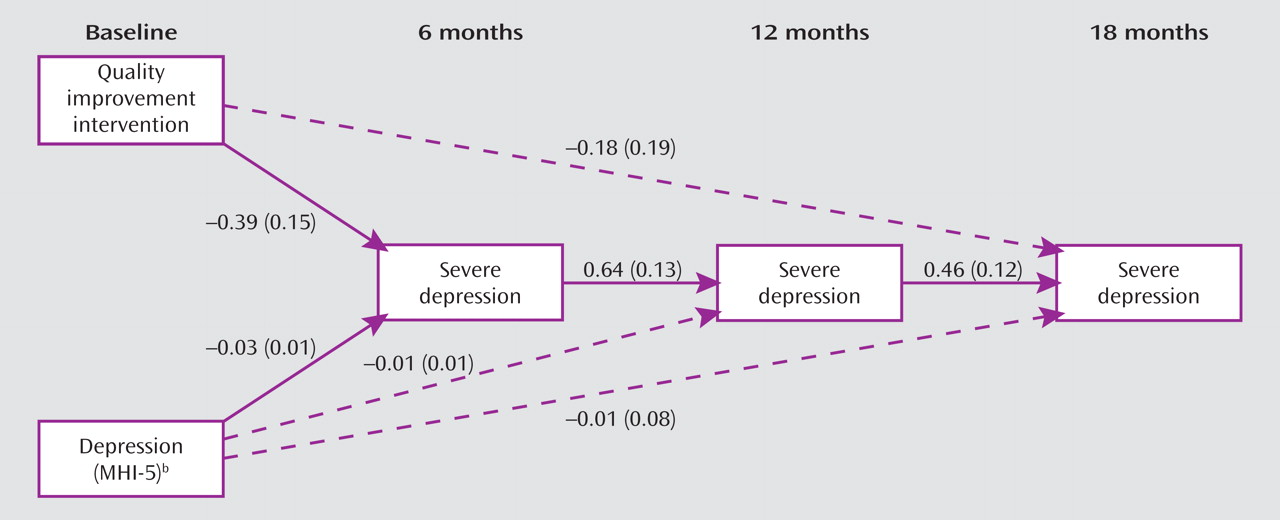
Figure 3 presents the path analysis model graphically, with probit models specified for the dichotomous outcome variable (severe depression) at three outcome time points (months 6, 12, and 18). Estimated coefficients and standard errors of the probit model are displayed for each significant path, depicted by a solid line; dashed lines show nonsignificant paths that were included in the model specification. For parsimony, the baseline covariates included in the model are not depicted. The direct effect of the intervention on 18-month outcome was not significant, although the indirect path specified was (t=–2.21, p=0.027), as were all of the paths within that indirect path: the effect of the intervention on 6-month depression (t=–2.57, p=0.011); the effect of 6-month depression on 12-month depression (t=4.91, p<0.001); and the effect of 12-month depression on 18-month depression (t=3.83, p<0.001). Sensitivity analyses replicated the path model using CES-D score (indirect effect: t=–2.29, p=0.023) and the secondary outcome of mental health-related quality of life (Short Form–12 mental health summary) (indirect effect: t=2.29, p=0.023), showing replication of findings across different outcome variables.
Figure 3. Path Model for Predicting Probability of Severe Depression Status After Receiving a Quality Improvement Intervention a
a Severe depression status was defined as a score ≥24 on the Center for Epidemiological Studies Depression Scale (CES-D). Path coefficients represent estimated coefficients (and standard errors) of the probit model. Solid lines depict significant paths, and dashed lines show nonsignificant paths included in the model specification.
b MHI-5=five-item Mental Health Inventory. Because the CES-D was not administered at baseline, baseline MHI-5 was used as an indicator of baseline depression. Lower scores on the MHI-5 indicate higher depression levels. At follow-up, CES-D and MHI-5 scores were highly correlated (r=0.78, p<0.001).
To our knowledge, this is the first study to evaluate a quality improvement intervention for depressed youths in primary care settings. We found that the intervention, relative to treatment as usual enhanced by provider training, led to more rapid recovery—specifically, to a reduced likelihood of severe depression 6 months after the intervention. Over an 18-month follow-up period, we observed a significant indirect intervention effect on rates of severe depression, depressive symptoms, and mental health-related quality of life. This finding suggests a continuing advantage for youths in the intervention group resulting from the initial clinical benefit of the intervention at 6 months, which then shifted youths toward a healthier path through 12 and 18 months. This may have occurred, for example, through a lowering of the risk for chronic or recurrent depression conferred by the initial clinical improvement. We found no support for a purely direct intervention effect on long-term outcomes, such as might have resulted from continuing differences in use of treatments or continuing application of strategies learned in CBT.
These results must be viewed in the context of the study limitations. Our sample size (N=418) was considerably smaller than the adult (N=1,356) and late-life depression (N=1,801) studies (11, 34), resulting in less statistical power to detect intervention effects. Given the high rates of recovery in youth depression and low levels of treatment received (particularly medication) relative to efficacy studies, a larger study is needed to replicate and further explain the indirect pathway findings or to observe small main effects. We also do not have data on longer-term outcomes allowing us to identify differences in relapse rates over several years. Other important limitations include selection of particular sites, moderate response rates, reliance on self-report measures, and the more exploratory nature of the causal modeling for indirect effects.
To our knowledge, only two prior studies have reported on the impact of depression treatment among adolescent primary care samples. Mufson et al. (35) demonstrated short-term (12-week) effects of a controlled trial of interpersonal psychotherapy delivered in school-based health clinics. Clarke et al. (36) found a marginal advantage for a 9-month collaborative care CBT program delivered in combination with “usual” SSRI medication compared with SSRI treatment alone; in an assessment of the program impact over 12 months, the strongest impact appeared to be between 6 and 9 months. Our findings are consistent with results of these studies in emphasizing the salience of early intervention effects as the main effects. We would expect weaker effects in Youth Partners in Care because of our emphasis on effectiveness with treatment delivered under “usual” treatment conditions, in which patients chose their preferred treatments (including no treatment), and treatment rates were lower relative to these other studies. In a study such as ours, even small main effects are of interest because they would suggest that strategies to further increase treatment utilization might further improve outcomes.
In the adult Partners in Care study and a study of similar quality improvement interventions for depressed elderly patients, outcome improvements were observed through 2 years, and for some groups, such as ethnic minorities and those with subthreshold depression, through 5 years and beyond (8, 34, 37 – 40) . The Partners in Care study reported indirect intervention effects that continued through 5 years and led to both improved health and life event outcomes (39) . The intervention effect sizes at 6 months looked similar for Partners in Care and Youth Partners in Care. Because of methodological differences, including in the measures used and in sample size, we cannot be confident that the youth intervention has smaller effect sizes at 18 months, but effect sizes do appear to be smaller at 12 months. Future research should focus on developing strategies to strengthen longer-term outcomes, such as finding ways to reinforce key information and access to resources for depression care as youths transition through different life roles and health care service delivery pathways. Because of relatively high natural recovery rates for youth depression, considerably larger samples (two to three times larger than in this study) will probably be needed to confidently determine the magnitude of any long-term outcome effects.
The results of this study reinforce the finding that quality improvement programs for youth depression improve clinical outcomes at 6 months, or by the end of the active intervention period, and shorten time to recovery within the first 6 months. They also suggest that such programs constitute an investment in the future health of youths by exerting a favorable effect on their course over the longer term through initial intervention effects. Although this finding must be replicated, it suggests an important direction for new research on improving outcomes for youth depression. It also may be encouraging to providers and families that their efforts to deliver and receive evidence-based depression care for youths may have longer-term, indirect benefits. The finding also supports the value of a more proactive effort to identify and support access to treatment for depressed youths in primary care and is generally consistent with the recent recommendations from the U.S. Preventive Services Task Force to screen adolescents for major depression when resources are adequate for evaluation, treatment, and follow-up (41) .
Footnotes
Received Nov. 20, 2008; revision received April 2, 2009; accepted April 23, 2009 (doi: 10.1176/appi.ajp.2009.08121909). From the David Geffen School of Medicine, UCLA, Los Angeles; Kaiser Permanente Los Angeles Medical Center; Venice Family Clinic, Venice, Calif.; Children’s Hospital, University of Pittsburgh, Pittsburgh; and Ventura County Medical Center, Ventura, Calif. Address correspondence and reprint requests to Dr. Asarnow, Neuropsychiatric Institute, UCLA School of Medicine, 760 Westwood Plaza, Los Angeles, CA 90024-1759; jasarnow@mednet.ucla.edu (e-mail).
Dr. Asarnow has received funding from the American Foundation for Suicide Prevention and unrestricted research funding from Philip Morris, has consulted on cognitive-behavioral therapy and quality improvement for depression, and has consulted on an unrestricted research grant from Pfizer. Dr. Jaycox has received unrestricted research funding from Pfizer. Dr. Murray has served on Merck’s speakers bureau and has been a member of the behavioral health committee of Highmark. Dr. Rea has consulted on cognitive-behavioral therapy and quality improvement for depression. The other authors report no competing interests.
Supported by grant HS09908 from the Agency for Healthcare Research and Quality. Additional support for data management and analysis was provided by NIMH grant P30 MH068639.
References
1.
Murray C, Lopez AD: The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability From Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020. Cambridge, Mass, Harvard University Press, 1996
Birmaher B, Brent D, AACAP Work Group on Quality Issues, Bernet W, Bukstein O, Walter H, Benson RS, Chrisman A, Farchione T, Greenhill L, Hamilton J, Keable H, Kinlan J, Schoettle U, Stock S, Ptakowski KK, Medicus J: Practice parameter for the assessment and treatment of children and adolescents with depressive disorders. J Am Acad Child Adolesc Psychiatry 2007; 46:1503–1526
Weisz JR, Jensen P, McLeod BD: Development and dissemination of child and adolescent psychotherapies: milestones, methods, and a new deployment-focused model, in Psychosocial Treatments for Child and Adolescent Disorders: Empirically Based Approaches, 2nd ed. Edited by Hibbs ED, Jensen PS. Washington, DC, American Psychological Association, 2003
Cheung AH, Zuckerbrot RA, Jensen PS, Stein RE, Laraque D: Expert survey for the management of adolescent depression in primary care. Pediatrics 2008; 121:e101–e107
Bower P, Garralda E, Kramer T, Harrington R, Sibbald B: The treatment of child and adolescent mental health problems in primary care: a systematic review. Fam Pract 2001; 18:373–382
Wells K, Sherbourne C, Schoenbaum M, Ettner S, Duan N, Miranda J, Unützer J, Rubenstein L: Five-year impact of quality improvement for depression: results of a group-level randomized controlled trial. Arch Gen Psychiatry 2004; 61:378–386
Katon W, Von Korff M, Lin E, Walker E, Simon GE, Bush T, Robinson P, Russo J: Collaborative management to achieve treatment guidelines: impact on depression in primary care. JAMA 1995; 273:1026–1031
Brent D, Emslie G, Clarke G, Wagner KD, Asarnow JR, Keller M, Vitiello B, Ritz L, Iyengar S, Abebe K, Birmaher B, Ryan N, Kennard B, Hughes C, DeBar L, McCracken J, Strober M, Suddath R, Spirito A, Leonard H, Melhem N, Porta G, Onorato M, Zelazny J: Switching to another SSRI or to venlafaxine with or without cognitive behavioral therapy for adolescents with SSRI-resistant depression: the TORDIA randomized controlled trial. JAMA 2008; 299:901–913
Bridge JA, Iyengar S, Salary CB, Barbe RP, Birmaher B, Pincus HA, Ren L, Brent DA: Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA 2007; 297:1683–1696
March J, Silva S, Petrycki S, Curry J, Wells K, Fairbank J, Burns B, Domino M, McNulty S, Vitiello B, Severe J; Treatment for Adolescents With Depression Study (TADS) Team: Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents With Depression Study (TADS) randomized controlled trial. JAMA 2004; 292:807–820
Birmaher B, Brent DA, Kolko D, Baugher M, Bridge J, Holder D, Iyengar S, Ulloa RE: Clinical outcome after short-term psychotherapy for adolescents with major depressive disorder. Arch Gen Psychiatry 2000; 57:29–36
Vostanis P, Feehan C, Grattan E, Bickerton WL: A randomised controlled out-patient trial of cognitive-behavioural treatment for children and adolescents with depression: 9-month follow-up. J Affect Disord 1996; 40:105–116
Asarnow JR, Jaycox LH, Duan N, LaBorde AP, Rea MM, Murray P, Anderson M, Landon C, Tang L, Wells KB: Effectiveness of a quality improvement intervention for adolescent depression in primary care clinics: a randomized controlled trial. JAMA 2005; 293:311–319
Rohde P, Clarke GN, Mace DE, Jorgensen JS, Seeley JR: An efficacy/effectiveness study of cognitive-behavioral treatment for adolescents with comorbid major depression and conduct disorder. J Am Acad Child Adolesc Psychiatry 2004; 43:660–668
Asarnow J, McKowen J, Jaycox L: Improving care for depression: integrating evidence-based depression treatment within primary care services, in Treatment of Adolescent Depression. Edited by Essau CA. London, Oxford University Press, 2009, pp 159–174
Asarnow JR, Carlson G, Schuster M, Miranda J, Jackson-Triche M, Wells KB: Youth Partners in Care: Clinician Guide to Depression Assessment and Management Among Youth in Primary Care Settings. Los Angeles, UCLA School of Medicine, 1999
Miranda J, Bernal G, Lau A, Kohn L, Hwang WC, LaFromboise T: State of the science on psychosocial interventions for ethnic minorities. Annu Rev Clin Psychol 2005; 1:113–142
Ware JE Jr, Kosinski M, Keller SD: A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996; 34:220–233
Berwick DM, Murphy JM, Goldman PA, Ware JE Jr, Barsky AJ, Weinstein MC: Performance of a five-item mental health screening test. Med Care 1991; 29:169–176
Unützer J, Katon W, Callahan CM, Williams JW Jr, Hunkeler E, Harpole L, Hoffing M, Della Penna RD, Noël PH, Lin EH, Areán PA, Hegel MT, Tang L, Belin TR, Oishi S, Langston C; IMPACT Investigators: Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA 2002; 288:2836–2845
Mufson L, Dorta KP, Wickramaratne P, Nomura Y, Olfson M, Weissman MM: A randomized effectiveness trial of interpersonal pychotherapy for depressed adolescents. Arch Gen Psychiatry 2004; 61:577–584
Clarke G, Debar L, Lynch F, Powell J, Gale J, O"Connor E, Ludman E, Bush T, Lin EH, Von Korff M, Hertert S: A randomized effectiveness trial of brief cognitive-behavioral therapy for depressed adolescents receiving antidepressant medication. J Am Acad Child Adolesc Psychiatry 2005; 44:888–898
Wells KB, Tang L, Miranda J, Benjamin B, Duan N, Sherbourne CD: The effects of quality improvement for depression in primary care at nine years: results from a randomized, controlled group-level trial. Health Serv Res 2008; 43:1952–1974
Sherbourne CD, Edelen MO, Zhou A, Bird C, Duan N, Wells KB: How a therapy-based quality improvement intervention for depression affected life events and psychological well-being over time: a 9-year longitudinal analysis. Med Care 2008; 46:78–84
Wells KB, Sherbourne CD, Miranda J, Tang L, Benjamin B, Duan N: The cumulative effects of quality improvement for depression on outcome disparities over 9 years: results from a randomized, controlled group-level trial. Med Care 2007; 45:1052–1059
US Preventive Services Task Force: Screening and treatment for major depressive disorder in children and adolescents: US Preventive Services Task Force Recommendation Statement. Pediatrics 2009; 123:1223–1228
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
Figure 3. Path Model for Predicting Probability of Severe Depression Status After Receiving a Quality Improvement Intervention a
a Severe depression status was defined as a score ≥24 on the Center for Epidemiological Studies Depression Scale (CES-D). Path coefficients represent estimated coefficients (and standard errors) of the probit model. Solid lines depict significant paths, and dashed lines show nonsignificant paths included in the model specification.
b MHI-5=five-item Mental Health Inventory. Because the CES-D was not administered at baseline, baseline MHI-5 was used as an indicator of baseline depression. Lower scores on the MHI-5 indicate higher depression levels. At follow-up, CES-D and MHI-5 scores were highly correlated (r=0.78, p<0.001).
Murray C, Lopez AD: The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability From Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020. Cambridge, Mass, Harvard University Press, 1996
Birmaher B, Brent D, AACAP Work Group on Quality Issues, Bernet W, Bukstein O, Walter H, Benson RS, Chrisman A, Farchione T, Greenhill L, Hamilton J, Keable H, Kinlan J, Schoettle U, Stock S, Ptakowski KK, Medicus J: Practice parameter for the assessment and treatment of children and adolescents with depressive disorders. J Am Acad Child Adolesc Psychiatry 2007; 46:1503–1526
Weisz JR, Jensen P, McLeod BD: Development and dissemination of child and adolescent psychotherapies: milestones, methods, and a new deployment-focused model, in Psychosocial Treatments for Child and Adolescent Disorders: Empirically Based Approaches, 2nd ed. Edited by Hibbs ED, Jensen PS. Washington, DC, American Psychological Association, 2003
Cheung AH, Zuckerbrot RA, Jensen PS, Stein RE, Laraque D: Expert survey for the management of adolescent depression in primary care. Pediatrics 2008; 121:e101–e107
Bower P, Garralda E, Kramer T, Harrington R, Sibbald B: The treatment of child and adolescent mental health problems in primary care: a systematic review. Fam Pract 2001; 18:373–382
Wells K, Sherbourne C, Schoenbaum M, Ettner S, Duan N, Miranda J, Unützer J, Rubenstein L: Five-year impact of quality improvement for depression: results of a group-level randomized controlled trial. Arch Gen Psychiatry 2004; 61:378–386
Katon W, Von Korff M, Lin E, Walker E, Simon GE, Bush T, Robinson P, Russo J: Collaborative management to achieve treatment guidelines: impact on depression in primary care. JAMA 1995; 273:1026–1031
Brent D, Emslie G, Clarke G, Wagner KD, Asarnow JR, Keller M, Vitiello B, Ritz L, Iyengar S, Abebe K, Birmaher B, Ryan N, Kennard B, Hughes C, DeBar L, McCracken J, Strober M, Suddath R, Spirito A, Leonard H, Melhem N, Porta G, Onorato M, Zelazny J: Switching to another SSRI or to venlafaxine with or without cognitive behavioral therapy for adolescents with SSRI-resistant depression: the TORDIA randomized controlled trial. JAMA 2008; 299:901–913
Bridge JA, Iyengar S, Salary CB, Barbe RP, Birmaher B, Pincus HA, Ren L, Brent DA: Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA 2007; 297:1683–1696
March J, Silva S, Petrycki S, Curry J, Wells K, Fairbank J, Burns B, Domino M, McNulty S, Vitiello B, Severe J; Treatment for Adolescents With Depression Study (TADS) Team: Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents With Depression Study (TADS) randomized controlled trial. JAMA 2004; 292:807–820
Birmaher B, Brent DA, Kolko D, Baugher M, Bridge J, Holder D, Iyengar S, Ulloa RE: Clinical outcome after short-term psychotherapy for adolescents with major depressive disorder. Arch Gen Psychiatry 2000; 57:29–36
Vostanis P, Feehan C, Grattan E, Bickerton WL: A randomised controlled out-patient trial of cognitive-behavioural treatment for children and adolescents with depression: 9-month follow-up. J Affect Disord 1996; 40:105–116
Asarnow JR, Jaycox LH, Duan N, LaBorde AP, Rea MM, Murray P, Anderson M, Landon C, Tang L, Wells KB: Effectiveness of a quality improvement intervention for adolescent depression in primary care clinics: a randomized controlled trial. JAMA 2005; 293:311–319
Rohde P, Clarke GN, Mace DE, Jorgensen JS, Seeley JR: An efficacy/effectiveness study of cognitive-behavioral treatment for adolescents with comorbid major depression and conduct disorder. J Am Acad Child Adolesc Psychiatry 2004; 43:660–668
Asarnow J, McKowen J, Jaycox L: Improving care for depression: integrating evidence-based depression treatment within primary care services, in Treatment of Adolescent Depression. Edited by Essau CA. London, Oxford University Press, 2009, pp 159–174
Asarnow JR, Carlson G, Schuster M, Miranda J, Jackson-Triche M, Wells KB: Youth Partners in Care: Clinician Guide to Depression Assessment and Management Among Youth in Primary Care Settings. Los Angeles, UCLA School of Medicine, 1999
Miranda J, Bernal G, Lau A, Kohn L, Hwang WC, LaFromboise T: State of the science on psychosocial interventions for ethnic minorities. Annu Rev Clin Psychol 2005; 1:113–142
Ware JE Jr, Kosinski M, Keller SD: A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996; 34:220–233
Berwick DM, Murphy JM, Goldman PA, Ware JE Jr, Barsky AJ, Weinstein MC: Performance of a five-item mental health screening test. Med Care 1991; 29:169–176
Unützer J, Katon W, Callahan CM, Williams JW Jr, Hunkeler E, Harpole L, Hoffing M, Della Penna RD, Noël PH, Lin EH, Areán PA, Hegel MT, Tang L, Belin TR, Oishi S, Langston C; IMPACT Investigators: Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA 2002; 288:2836–2845
Mufson L, Dorta KP, Wickramaratne P, Nomura Y, Olfson M, Weissman MM: A randomized effectiveness trial of interpersonal pychotherapy for depressed adolescents. Arch Gen Psychiatry 2004; 61:577–584
Clarke G, Debar L, Lynch F, Powell J, Gale J, O"Connor E, Ludman E, Bush T, Lin EH, Von Korff M, Hertert S: A randomized effectiveness trial of brief cognitive-behavioral therapy for depressed adolescents receiving antidepressant medication. J Am Acad Child Adolesc Psychiatry 2005; 44:888–898
Wells KB, Tang L, Miranda J, Benjamin B, Duan N, Sherbourne CD: The effects of quality improvement for depression in primary care at nine years: results from a randomized, controlled group-level trial. Health Serv Res 2008; 43:1952–1974
Sherbourne CD, Edelen MO, Zhou A, Bird C, Duan N, Wells KB: How a therapy-based quality improvement intervention for depression affected life events and psychological well-being over time: a 9-year longitudinal analysis. Med Care 2008; 46:78–84
Wells KB, Sherbourne CD, Miranda J, Tang L, Benjamin B, Duan N: The cumulative effects of quality improvement for depression on outcome disparities over 9 years: results from a randomized, controlled group-level trial. Med Care 2007; 45:1052–1059
US Preventive Services Task Force: Screening and treatment for major depressive disorder in children and adolescents: US Preventive Services Task Force Recommendation Statement. Pediatrics 2009; 123:1223–1228
Figure 3. Path Model for Predicting Probability of Severe Depression Status After Receiving a Quality Improvement Intervention a
a Severe depression status was defined as a score ≥24 on the Center for Epidemiological Studies Depression Scale (CES-D). Path coefficients represent estimated coefficients (and standard errors) of the probit model. Solid lines depict significant paths, and dashed lines show nonsignificant paths included in the model specification.
b MHI-5=five-item Mental Health Inventory. Because the CES-D was not administered at baseline, baseline MHI-5 was used as an indicator of baseline depression. Lower scores on the MHI-5 indicate higher depression levels. At follow-up, CES-D and MHI-5 scores were highly correlated (r=0.78, p<0.001).
Table 1
No caption available.
Reference #1
Request Username
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.