Reports of sudden death among children and adolescents receiving stimulant medications for treatment of attention deficit hyperactivity disorder (ADHD) have raised concerns about the safety of these agents. There have been reports of pediatric stroke after long-term use of methylphenidate within therapeutic ranges
(1) . Acute myocardial infarction has been reported in one adolescent taking methylphenidate for an unknown period of time
(2) and in another adolescent 1 week after restarting a daily 20-mg prescription of mixed amphetamine salts
(3) . Cardiac arrest occurred in another adolescent who was taking methylphenidate for ADHD and who had previously had a normal baseline echocardiogram
(4) . The Food and Drug Administration (FDA), using the Adverse Event Reporting System, reported 11 sudden deaths in pediatric patients taking methylphenidate from January 1992 to February 2005
(5) . While the FDA’s reporting rate of sudden death in stimulant-treated children was the same as the base rate in the general population, spontaneous reports of sudden deaths may underestimate their true incidence, and limited available information on total number of prescriptions precludes reliable estimates of stimulant exposure
(5) . Less serious cardiovascular effects have also been reported in association with stimulant medications. An average increase in diastolic blood pressure of 4 mm Hg has been found among stimulant-treated youths in placebo-controlled trials
(5,
6) . A 10-year analysis of Florida Medicaid claims data revealed that stimulant use among youths diagnosed with ADHD was associated with increases of 20% and 21% in risk of emergency department visits and physician office visits for cardiac symptoms, respectively
(7) . No cardiac sudden deaths occurred during the 42,612 person-years of current stimulant use; however, as the authors noted, the rarity of sudden death and cardiac mortality in this age group would have necessitated a sample size 16 times larger, i.e., approximately 2,000,000 person-years, to detect a significant difference between the stimulant use and nonuse groups.
There continues to be controversy surrounding whether there exists an association between stimulant use for the treatment of ADHD and serious cardiovascular events, including sudden death, with accompanying debate over clinical recommendations for physicians and families
(8,
9) . The FDA’s Pediatric Advisory Committee in March of 2006 voted unanimously against a black box warning, which had been proposed by an earlier FDA advisory committee, but recommended a warning targeted to specific high-risk children, such as those with structural heart defects, cardiomyopathy, or heart-rhythm disturbances
(10) . In 2008, the American Heart Association recommended considering routine ECGs prior to starting children with ADHD on stimulant and other psychotropic therapy regimens
(11) but underscored the need for future studies to assess the risk of sudden death associated with stimulant medication use in children and adolescents. The American Academy of Pediatrics
(12) has also highlighted the “absence of scientific data to establish an increased risk of sudden death in individuals receiving stimulant medications.”
Method
This study was initiated in 1996, with support from the National Institute of Mental Health (NIMH), to examine the association between sudden death in children and adolescents and the use of tricyclic antidepressants or concomitant methylphenidate and clonidine therapy
(15,
16) . During the course of the study, there was a marked decrease in the use of tricyclic antidepressants in youths
(17) and an associated significant increase in the use of selective serotonin reuptake inhibitors (SSRIs), which led to an attenuation of the clinical relevance of our examination of the association of tricyclic antidepressants and sudden death. Thus, these analyses were not pursued further. In light of concerns over the safety of stimulant medications, the FDA in 2006 requested an expansion of the inquiry of stimulants to include amphetamine, dextroamphetamine, and methamphetamine. The current report focuses on stimulant use among children and adolescents.
Definition of Sudden Unexplained Death
A case of sudden unexplained death was defined as any cause of death listed as ICD-9 codes E798 (sudden death, cause unknown), E799.9 (other unknown and unspecified causes), or E427 (cardiac dysrhythmia). These codes reflected causes of death in case reports of sudden death in children using tricyclic medications
(15), consistent with the original goal of the study. We targeted cases 7 through 19 years of age, identified from mortality data from 1985 –1996 state vital statistics across the United States.
Exclusion criteria were 1) deaths with known causes—such as accidental deaths, suicides, overdoses, homicides, and natural causes (e.g., asthma)—initially misclassified on death certificate as unknown and subsequently amended; 2) deaths in which there were medical intervention complications or among individuals hospitalized for more than 48 hours at the time of death; or 3) coexisting physical disorders known or suspected to be associated with sudden death but not listed as the cause of death on the death certificate or autopsy report, such as Marfan’s syndrome
(14), Wolff-Parkinson-White syndrome
(18), severe cerebral palsy
(19), profound developmental delays
(20), seizure disorders
(21), sickle cell anemia
(22), morbid obesity
(23), asthma
(24), anorexia nervosa
(25), prolonged QT interval in the deceased or in any first-degree relative, history of sudden death among first-degree relatives, conduction disorders in the deceased, and evidence of cardiac disease or abnormal anatomical finding on autopsy, such as cardiomegaly, cardiac hypertrophy, and cardiomyopathy
(14) .
Comparison Group
Individuals who died as passengers in motor vehicle traffic accidents with another motor vehicle (ICD-9 code E812.1) were also examined. A comparison group of
deceased youngsters was necessary to avoid differential recall biases. Parents of both sudden unexplained death and motor vehicle accident victims had experienced a
sudden, traumatic loss of their children. Unlike other victims of injuries
(28), motor vehicle passenger victims were selected because they have been found
not to be at greater risk for hyperactivity and other deficits in vigilance, attention, and impulse control. Thus, we avoided inappropriately increasing the likelihood of stimulant use among the comparison group. In this way, subjects were likely to be representative of the general population of youths 7 through 19 years of age. The same exclusion criteria noted for sudden unexplained death subjects were applied to the motor vehicle accident victims.
Comparison subjects were individually matched to sudden unexplained death cases by year of death (within 3 years), age (within 3 years), gender, and data source available. Each matched pair was unique; an individual motor vehicle accident victim was matched to one and only one case of sudden unexplained death. Limitations in the pool of comparison subjects precluded matching on race and census geographic region of death, factors that may affect rate of stimulant medication use
(7,
26) .
Definition of Exposure
The primary exposure variable was evidence of stimulant use immediately prior to death, indicated by presence of amphetamine, dextroamphetamine, methamphetamine, methylphenidate, or their derivatives, as noted by informants or in medical examiner records, toxicology findings, or death certificates. Information was also obtained about use of clonidine, tricyclic antidepressants, and SSRI antidepressants.
Sources of Data
Mortality data and death certificates were obtained from state vital statistics offices across the United States (including New York City and the District of Columbia) for 1985 through 1996. Indiana, Kansas, Maryland, Wisconsin, and Wyoming were excluded because their state statutes did not allow direct interviewing of families of deceased individuals or had restrictive contact requirements.
For informant reports, the names of the deceased child and his or her parents and the address at time of death were identified from the death certificate, on public record, from the state vital statistics offices. Parents were approached by letter describing the purpose of the study and were asked to complete a survey. The survey included items assessing medical history, medications taken at time of death, a list of medical problems, and the use of over-the-counter and prescription medications. A history of sudden death among relatives was also assessed. To locate informants, various Internet search engine white pages, a credit bureau database (without access to credit information), ChoicePoint (CDB Infotek), and PrivateEye were used.
Medical examiner records and toxicology findings were used to identify medication use and assist in the identification of exclusion criteria. Medical examiner reports could include informant- or toxicology-based findings, as well as autopsy reports. The applied postmortem detection threshold for a blood or urine stimulant level to be deemed positive varied considerably across jurisdictions. Thus, our reports of a positive finding reflect a value above the stated threshold for each individual laboratory.
Procedures
Data collection, from March 1997 to January 2008, involved the following phases. Cases of sudden unexplained death were identified through state mortality data, and death certificates were obtained from state vital statistics offices. Death certificates were reviewed for eligibility by the research team. Parents were approached for surveys and consent for records, if required by state law. Autopsy and toxicology records obtained from medical examiners were reviewed and abstracted. The same procedures were applied to motor vehicle accident victims matched to sudden unexplained death cases with surveys or toxicology results.
A two-stage determination of eligibility for all subjects was conducted by the two principal investigators (M.S.G. and B.T.W.) and research staff, blind to medication status. The first stage involved the examination of death certificates, and the second involved review of informant reports and medical examiner, autopsy, toxicology, and medical records.
The Institutional Review Board of the New York State Psychiatric Institute/Columbia University Department of Psychiatry approved study procedures, and a Certificate of Confidentiality was issued by NIMH.
Analytic Strategy
The basic unit of analysis is the matched dyad, rather than the individual subject. We estimated the association between sudden unexplained death and stimulant exposure using a logistic regression model that predicted sudden unexplained death from stimulant exposure. Race and region of death were included as covariates in all logistic regression models. In light of matching on sources of information (e.g., medical examiner records, toxicology, and informant reports), only sources available for both members of the matched pair were used to define exposure status. In the primary analysis, using the total sample, exposure was defined as any stimulant indication. A series of sensitivity analyses varied the exposure definition, including the presence of any stimulant as noted by informants; any stimulant reported in medical examiner records or toxicology reports; methylphenidate reported by any source; methylphenidate noted by informants; and methylphenidate disclosed in medical examiner records or toxicology reports. Each sensitivity analysis used the subsample of dyads with observed data for the specific information source.
In light of the original study’s intent to examine the association of sudden death with tricyclic antidepressants and with concomitant methylphenidate and clonidine use, we conducted another series of analyses to assess whether these associations might be significant in our sample in order to determine whether the concomitant use of these medications needed to be taken into account in our current sensitivity analyses of stimulant exposure.
Pairing of subjects
(27) was incorporated into the conditional logistic regression model through exact conditional logistic regression using the EXACT statement in the LOGISTIC procedure in SAS statistical software, release 8.1.
Results
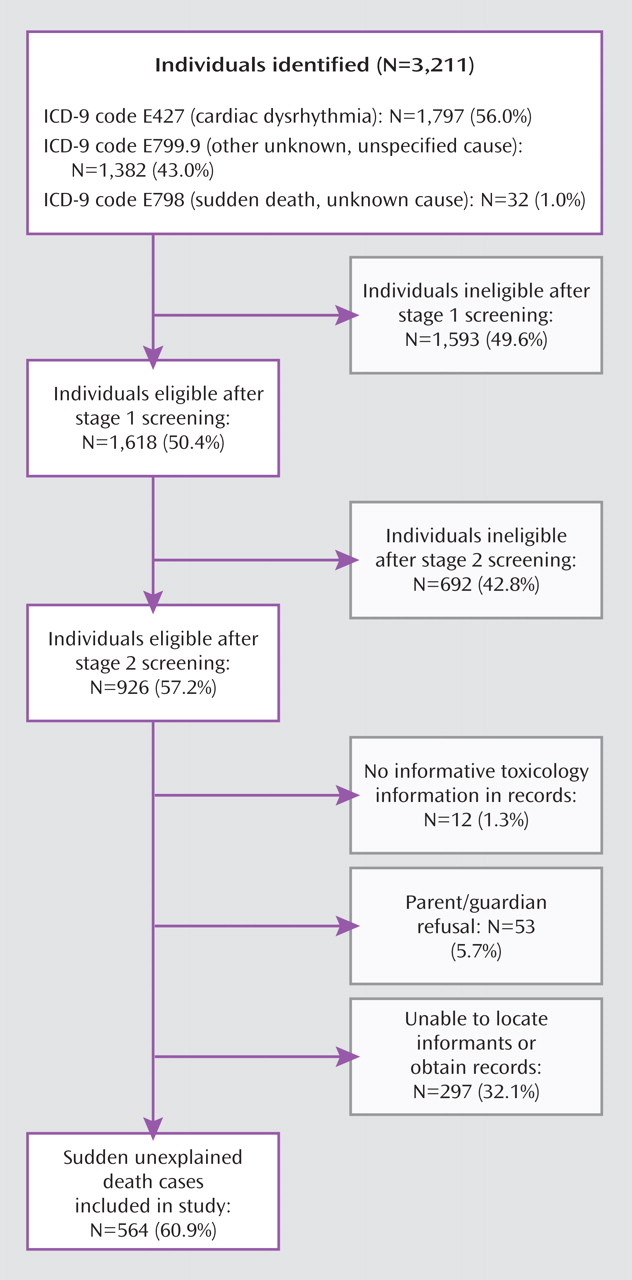
Eligible individuals (N=926) were identified from a pool of 3,211 youths with deaths listed as ICD-9 codes E798, E799.9, or E427 (
Figure 1 ).
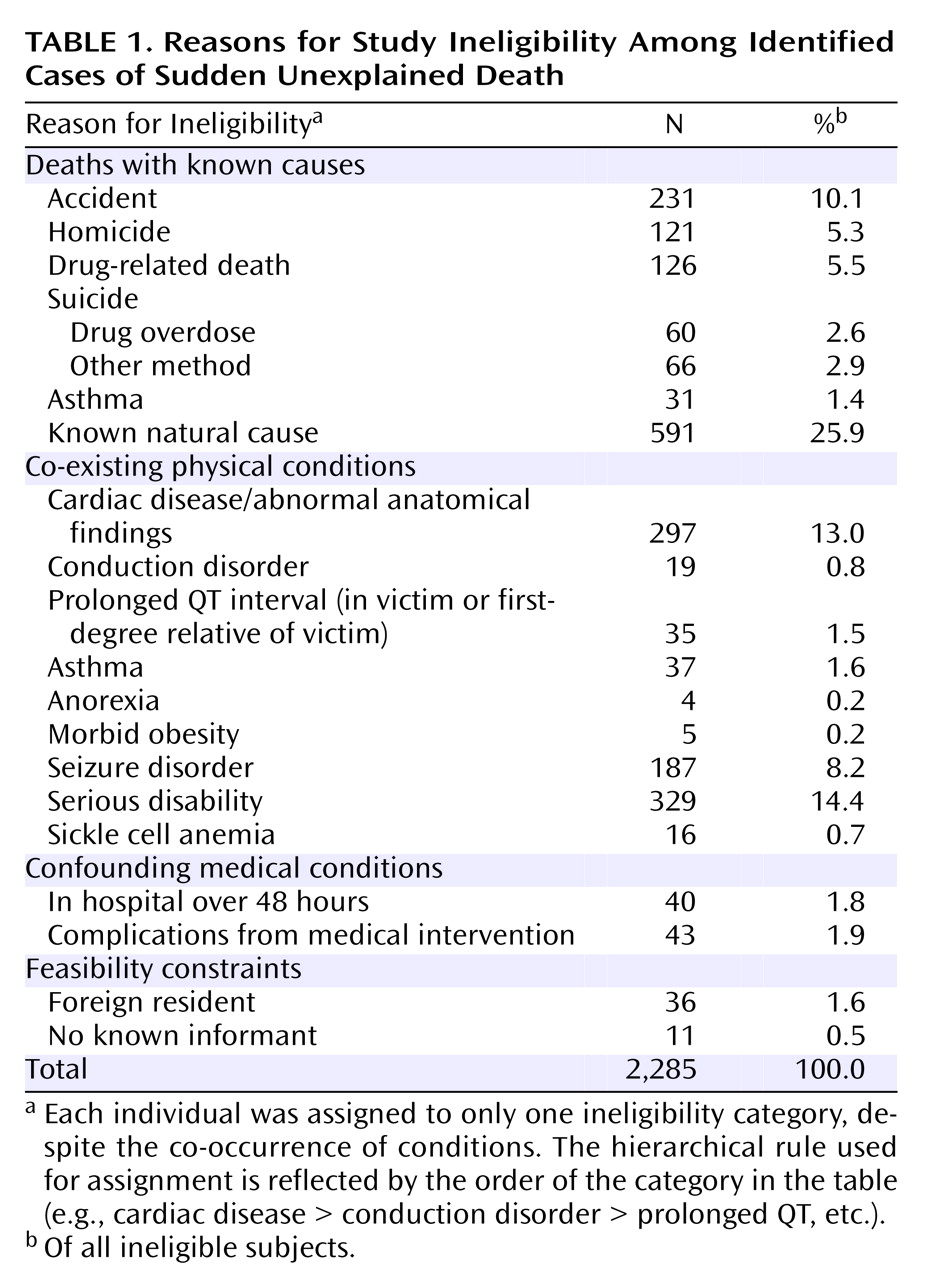
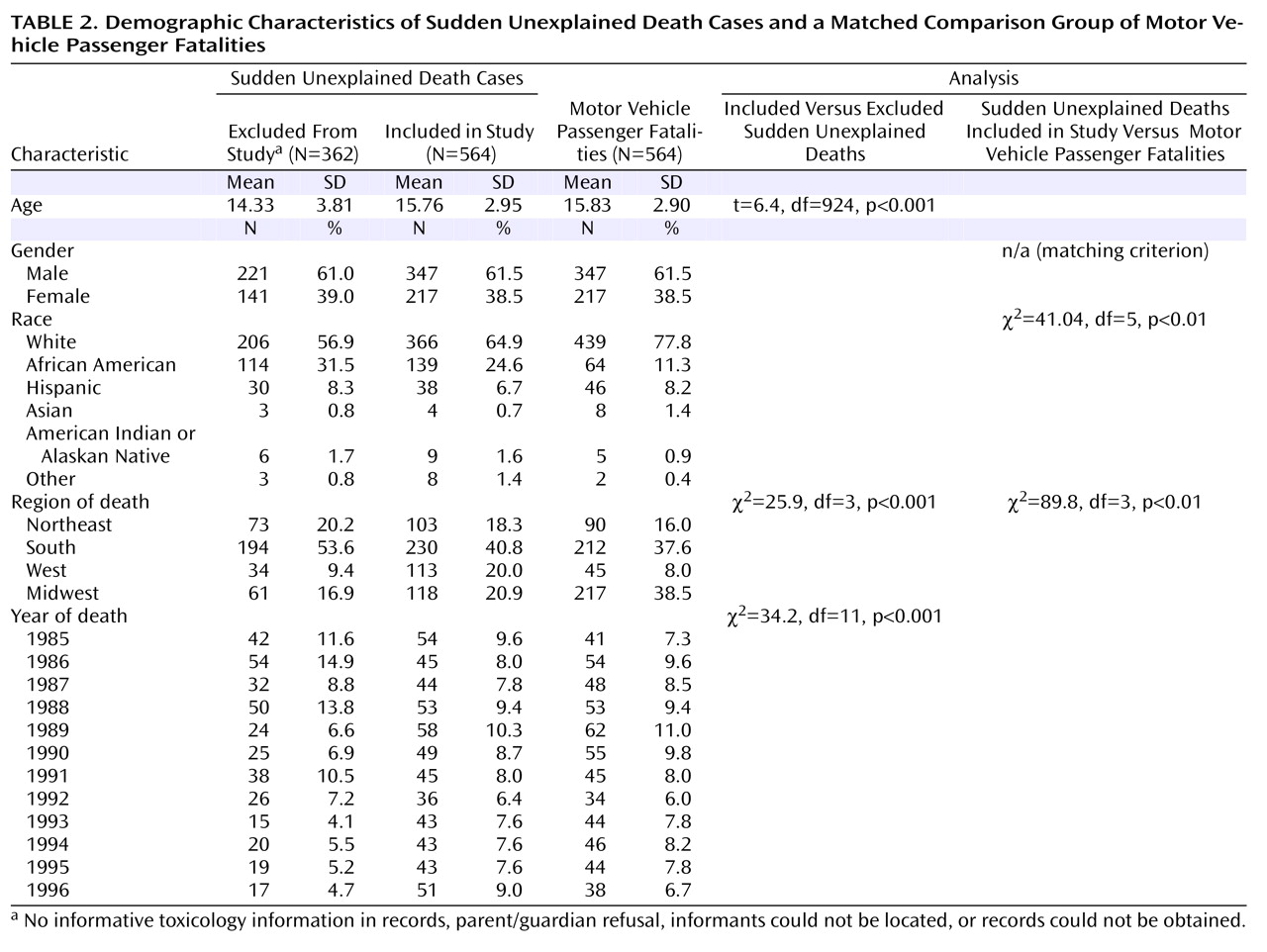
Table 1 provides the reasons for ineligibility. The overall study inclusion rate was 60.9% (N=564 of 926). Study exclusion was due largely to our inability to locate informants listed on the death certificates and obtain medical examiner or toxicology records. There were no significant differences in gender or race between the sudden unexplained death cases included and excluded from the study. However, there were significant differences in age, region of death, and year of death (
Table 2 ).
The group of 564 comparison subjects was obtained from a potential pool of 1,014 motor vehicle passenger fatalities, identified from jurisdictions that conducted informative toxicology screens. Thus, 55.6% of the total pool of motor vehicle passenger fatalities were matched to a sudden unexplained death case.
Table 2 displays the demographic characteristics of the sudden unexplained death cases included in the study and the motor vehicle accident comparison group; race and region of death significantly differed between the two groups. The distribution of the information sources available for the 564 matched pairs was as follows: informant reports only (29.6%); medical examiner records or toxicology reports only (55.5%); informant reports and medical examiner records but no toxicology report (5.3%); and all three sources (9.6%).
Matched Pair Analyses
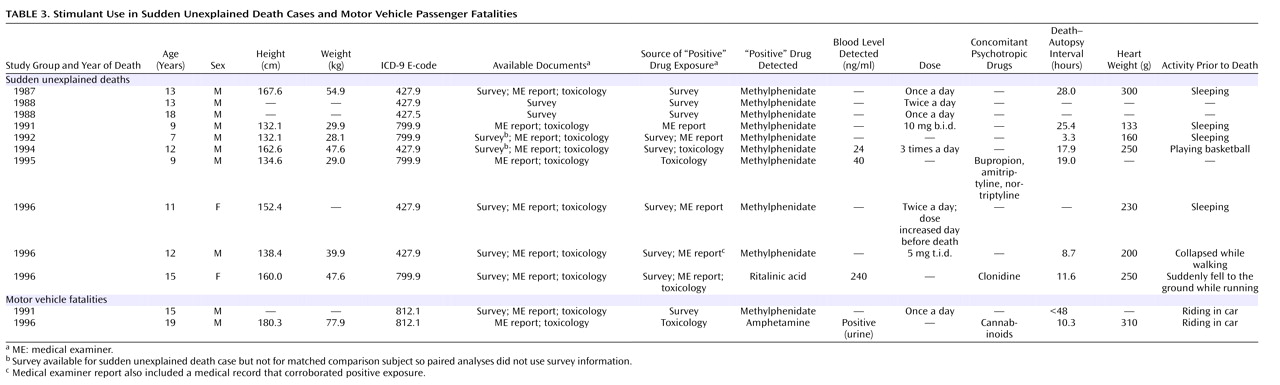
Ten of the 564 sudden unexplained death cases (1.8%) were identified as having used stimulants at the time of their deaths (
Table 3 ). In each of these cases, the stimulant detected was methylphenidate. Stimulants were identified in two of the 564 motor vehicle accident comparison subjects (0.4%). Detailed information on the dose or duration of stimulant use was not available. Rates of stimulant use among subjects fell within the range reported for the years of study
(26,
28,
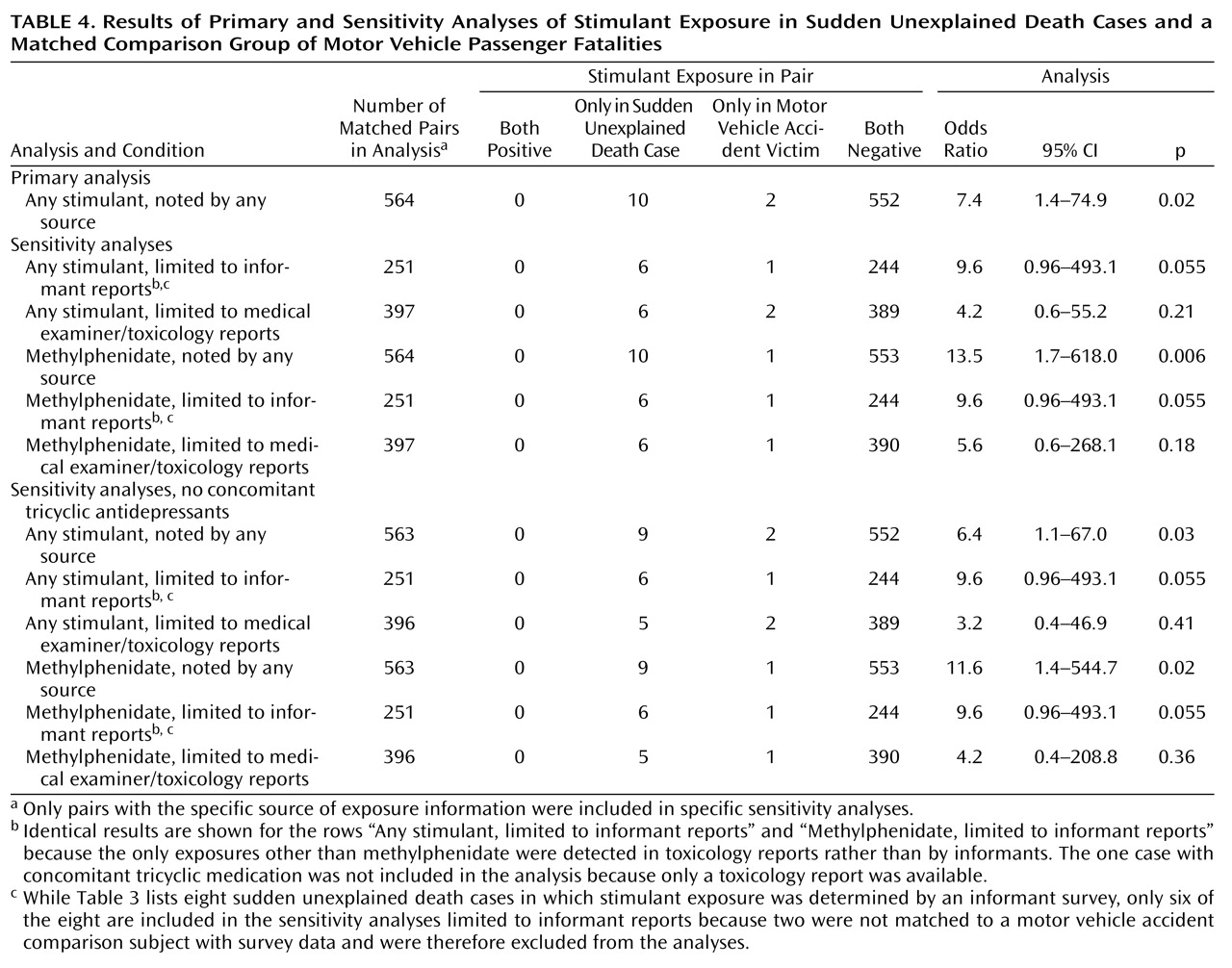
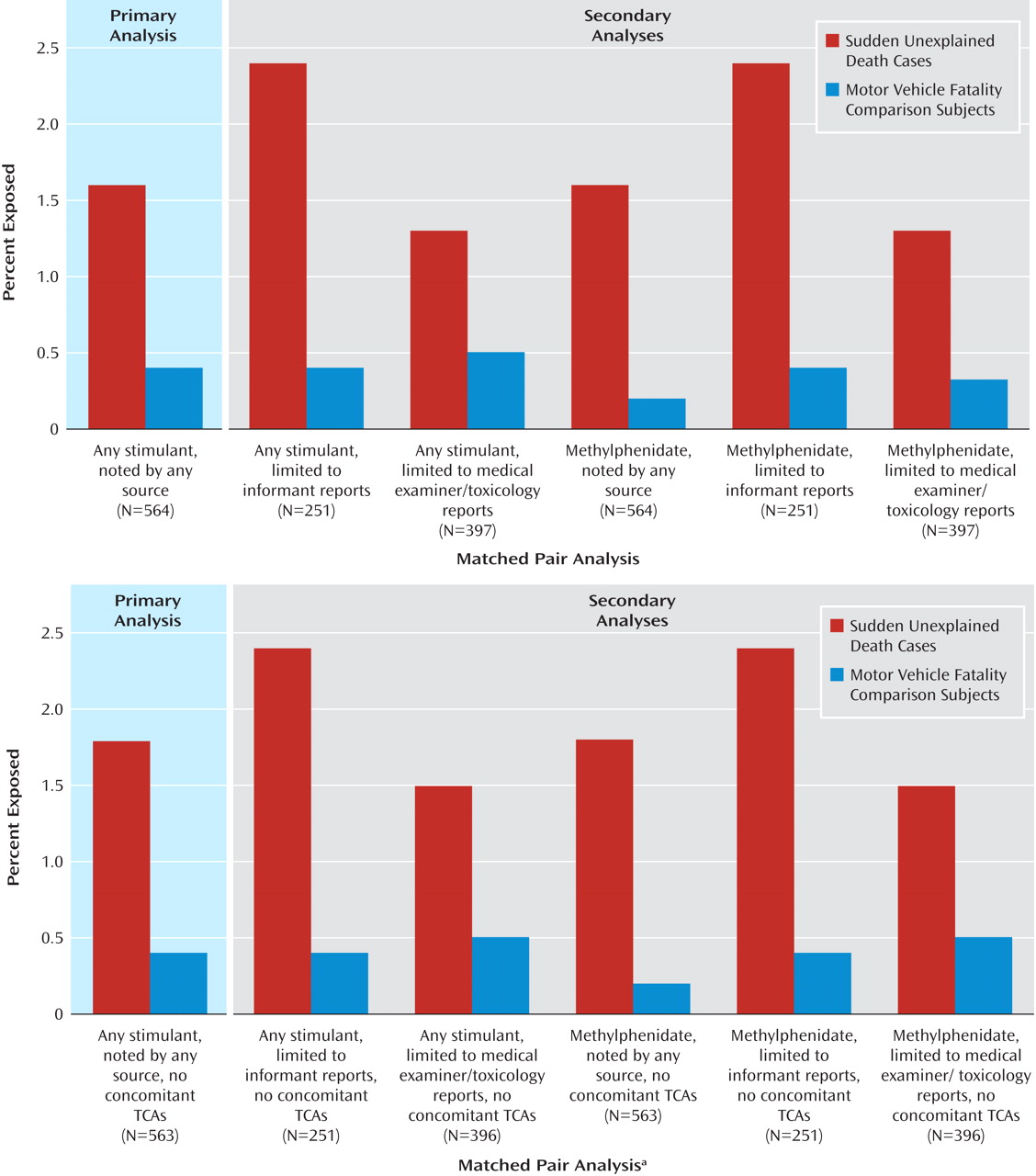
29) . Results of the primary analysis and sensitivity analyses are presented in
Table 4, and the rates of exposure in the groups for each of these analyses are presented in
Figure 2 . The odds ratio derived from the primary exact logistic regression was 7.4 (95% CI=1.4–74.9; p=0.02). Sensitivity analyses using alternative measures of stimulant exposure revealed qualitatively similar findings, indicating that qualitatively our finding is insensitive to the stimulant exposure algorithm. In particular, all odds ratios observed were clinically significant
(30), with the smallest one being 4.2 for the scenario “any stimulant, limited to medical examiner/toxicology reports.”
Preliminary analysis of the association of tricyclic antidepressants with sudden death indicated that they might be associated in our sample (six exposures among our sudden death cases and none among our motor vehicle accident comparison subjects). Thus, another series of sensitivity analyses, paralleling those described previously, was conducted deleting any individuals with concomitant tricyclic antidepressant and stimulant use (
Table 4 and bottom half of
Figure 2 ). The sensitivity analyses, excluding the stimulant-exposed sudden death case with concomitant tricyclic antidepressants, yielded essentially the same results, with the smallest odds ratio being 3.2, again for the scenario “any stimulant, limited to medical examiner/toxicology reports.” The use of clonidine appeared not to be associated with sudden death, providing no justification to delete the case with concomitant clonidine and stimulants. In analyses with reduced numbers of total observations or exposures, some of the p values fell below statistical significance. However, the focus of sensitivity analysis is on the effect sizes (the odds ratios), which reflect the strength of the association, rather than the p values, which are a function of sample size
(31) .
Examination of Potential Biases
Threshold postmortem blood levels of detection of the targeted stimulant exposure varied by jurisdiction, raising the possibility that the thresholds for sudden unexplained death cases might be more sensitive than for the comparison group of motor vehicle accident victims. Mean threshold detection levels available for 83 cases of sudden unexplained death and 66 motor vehicle accident deaths indicated that their thresholds for methylphenidate were not significantly different (mean=127.7 ng/ml versus 108.8 ng/ml, respectively; t=1.2, df=147, p=0.23).
Since a matched comparison subject was only sought after the identification of a case with appropriate documents, the interval between date of death and informant survey was significantly longer for the comparison subjects (mean=12.8 years, SD=4.5) than the sudden unexplained death cases (mean=9.8 years, SD=5.2) (t=9.5, df=252, p<0.01), suggesting a possible recall bias. However, deleting all three motor vehicle accident victims whose death-to-survey interval was greater than two standard deviations above the mean of the sudden unexplained death cases did not change the results of the matched-pair analysis (odds ratio=7.3, 95% CI=1.4–74.0; p=0.02). Moreover, the death-to-survey interval was not significantly related to reports of stimulant exposure among sudden unexplained death cases (odds ratio=0.99, 95% CI=0.98–1.01; p=0.46). An informant survey was available for only one stimulant-exposed motor vehicle accident victim, precluding the inclusion of motor vehicle accident victims in a similar analysis. The distribution of informants did not significantly differ by group (χ 2 =8.1, df=6, p=0.23). A great majority of informants for sudden unexplained death cases (91.2%) and motor vehicle accident victims (93.2%) were parents/legal guardians, suggesting that differential recall bias is unlikely to be an important source of bias.
Discussion
In recent years, concerns have arisen that stimulants may be associated with an increased risk of death. Results of the current study are consistent with these concerns. The odds of using stimulant medications were approximately six to seven times greater for the cases of sudden unexplained death than for the matched motor vehicle accident victims. Such an association is biologically plausible given the central and peripheral catecholaminergic effects of stimulants and significant increases in heart rate and blood pressure that accompany their use
(32) .
The present study has several strengths. First, it employed a matched case-control design, which yielded substantial power to detect rare outcomes. Second, multiple sources of information were used to increase the sensitivity of detecting stimulant use. Third, the availability of parent reports lessened the possibility that the findings reflect illicit stimulant use, since it is unlikely that parents would have known of or reported illicit stimulant use. The single youth who appeared likely to have used stimulants illicitly was a motor vehicle accident victim, whose “positive” exposure was detected by toxicology alone. Fourth, several potential confounding factors, such as asthma, that are associated with both ADHD
(33) and sudden death
(24), were excluded. Furthermore, because ADHD
(34) and impaired attention
(35) are common among youths with some congenital structural cardiac diseases, we excluded individuals with evidence of cardiomegaly, cardiac hypertrophy, and cardiomyopathy. Three individuals receiving stimulants were excluded from our group of sudden unexplained death cases because of notations of cardiac hypertrophy in their autopsies, even though the cardiac abnormalities were not cited as the cause of death. Moreover, we deleted a sudden death case with concomitant use of stimulants and tricyclic antidepressants, another possible confounding factor, in a second series of sensitivity analyses, and this had little effect on the results. Fifth, the study’s dates of inquiry (1985–1996) predated the use of Adderall, first approved by the FDA in 1996, which has been the stimulant medication most strongly implicated in sudden death
(36) .
The study also has important limitations. First, while case-control studies are a powerful method of detecting association, they cannot establish causality. It is conceivable that, despite our rigorous efforts to exclude or adjust for potential confounding factors, some unmeasured factors other than stimulant use were responsible for the observed association. For example, although gross structural cardiac disease was presumably excluded by autopsy, autopsy data were not available for two sudden unexplained death cases with stimulant exposure, and forensic pathology varies substantially in its ability to identify physiological as opposed to anatomic cardiovascular disease. Physiological abnormalities that confer risk (e.g., cardiac depolarization and repolarization abnormalities such as Brugada syndrome and long QT syndrome) could not be reliably excluded from the analysis. We attempted to exclude subjects with known prolonged QT interval, other conduction disorders, or a family history of long QT or sudden cardiac death, but clinically significant cardiac abnormalities may have passed undetected. However, a sensitivity analysis revealed that even if 40% of sudden unexplained death cases were excluded due to undetected cardiac disease, the primary analysis would still yield a significant association.
Second, we were unable to systematically obtain information on the psychiatric status of the decedents, including their clinical diagnoses. While this information was occasionally noted in a medical record or by an informant, it was not available for all subjects. Therefore, we are unable to estimate accurately the rates of ADHD in our sample, nor can we determine whether untreated ADHD was associated with sudden unexplained death. Although we excluded the known presence of structural cardiac diseases
(24), as well as asthma
(24,
33), there may be other unidentified mechanisms that were not controlled.
Third, we attempted to avoid differential recall biases, an important potential limitation of retrospective case-control studies, by employing a comparison group of deceased youths whose parents/legal guardians had also experienced a sudden, traumatic loss of their children. However, we cannot exclude the possibility that relative to a motor vehicle passenger fatality, an “unexplained” death may have prompted medical personnel to ask more questions about medications at the time of death. Yet the primary analysis remains significant (odds ratio=7.3, 95% CI=1.4–74.8, p=0.015) following exclusion of the one sudden unexplained death case whose methylphenidate exposure was detected solely from the medical examiner’s report. Although conceivable, we consider it unlikely that parents of sudden unexplained death cases remembered stimulant medications more vividly than parents of children who died in accidents. It is reassuring that medical records available for two sudden unexplained death cases whose “positive” exposures were based solely on the parental survey corroborated these informant reports. Because we were unable to obtain medical records on a majority of our subjects, we did not use them to identify “positive” exposures.
Fourth, toxicological assays were not conducted consistently across jurisdictions and may not have been sufficiently sensitive to detect therapeutic levels of methylphenidate, yielding an unreliable measure of exposure. The average detection threshold in toxicological assays (approximately 100 ng/ml) appeared to be higher than blood levels achieved during routine therapeutic use of immediate-release methylphenidate preparations (24 ng/ml)
(37), or the even lower peak plasma levels of 8–10 ng/ml achieved by the more recently marketed single daily dose, long-duration methylphenidate preparations, such as OROS methylphenidate
(38) . The short half-life of methylphenidate
(37,
39) and the interval between the last ingestion of medication and the acquisition of the blood samples is another potential source of insensitivity of the toxicology screens. Because sustained-release stimulants had not yet been widely marketed during the years of study (1985–1996), a therapeutic dose may not have remained in the blood for sufficient time to be detected by postmortem toxicology screens. This may explain why stimulants were not detected in the toxicology reports of five sudden unexplained death cases whose stimulant use was reported by the informant or noted in the medical examiner’s record (as reported by an informant at the time of death). Thus, while we are confident that the toxicology screens accurately ruled out overdoses, they may have been insensitive in some cases to therapeutic levels of methylphenidate. Nevertheless, since only sources of information available for
both sudden unexplained death cases and matched motor vehicle fatality victims were used in the analyses, limitations in a particular source of exposure, whether toxicology records or informant reports, were comparable across groups. Moreover, sensitivity analyses suggest that qualitatively our results were not sensitive to method of stimulant measurement.
Fifth, we were able to include in our analyses only 61% of the eligible cases of sudden unexplained death. Although there were no significant differences in gender or race between included and excluded subjects, these groups did significantly differ in age, region, and year of death. Sudden unexplained death cases included in the study were significantly older, less likely to have died in the South, more likely to have died in the West, and more likely to have died in the later years of the study. Nationally representative studies indicate that stimulant use rates vary by age, region, and year
(26,
28) . Differences in age would likely have yielded
lower rates of stimulant use among those included because age is inversely related to stimulant use
(26,
28) . Similarly, since the South has the highest rate of stimulant use and the West has the second lowest rate
(26), rates of stimulant use among sudden unexplained death cases included in the study would likely have been
lower than in those excluded. Conversely, the steep increase in the utilization of stimulants over time
(26,
28,
29) would bias toward
more stimulant use among the included than the excluded subjects. Although included subjects are not representative of all sudden unexplained death cases, pairs were either matched (age, gender, and date of death) or adjusted (race and region of death) for these sociodemographic and vital characteristics. Nevertheless, there may be unknown selection biases related to our inability to obtain information from all potential cases.
Last, because the project was originally funded to examine the association of sudden death and the use of tricyclic antidepressant medication, we did not include pediatric stroke and acute myocardial infarction, other causes of death linked to methylphenidate in case reports
(1 –
3,
40) . This may have yielded an underestimation of the association between sudden death and stimulant use.
This study reports a significant association or “signal” between sudden unexplained death and the use of stimulant medication, specifically methylphenidate. While the data have limitations that preclude a definitive conclusion, our findings draw attention to the potential risks of stimulant medications for children and adolescents, which warrant clinical attention and further study.