Depression during adulthood is one of the leading causes of the global burden of disease (
1), making research into prevention a priority. While it is rarely possible to prevent the occurrence of the adverse events and circumstances that are thought to increase the risk of depression, it may be possible to prevent development of depressogenic interpretations of adverse events, which may in turn reduce the risk of developing depression. Understanding the origins of depressogenic cognitive style is therefore important in strategies to prevent depression.
Beck’s cognitive theory of depression (
2) suggests that the presence of negative belief systems regarding the self, the world, and the future underlie the development of depression. Beck’s theory is consistent with research on attributional styles, which suggests that the application of such depressogenic beliefs to one’s interpretation of negative life events is associated with depression (
3). Recent research has extended Beck’s theory to more basic cognitive biases. For example, attentional bias toward negative stimuli is also associated with vulnerability to depression (
4). Such biases may represent a lower cognitive level of depressogenic beliefs: the beliefs we hold direct the information we bias and vice versa. In this article, however, we focus on depressogenic cognitive style defined as the tendency to attribute negative events to causes that are internal (caused by self), global (have an impact on a wide domain of activities), and stable (are difficult to change). Cognitive style is important because it represents the application of cognitive biases to the self and the interpretation of adverse events. Indeed, cognitive style is one of the therapeutic targets of cognitive behavioral therapy, and previous research has shown that this style is associated with both concurrent and future episodes of depression (
5).
Twin studies suggest that there may be both genetic and environmental influences on depressogenic cognitive style (
6). However, the reported genetic correlations for cognitive style are small, and smaller than those for depression or anxiety disorders themselves (
7). Therefore, cognitive style may develop largely through experience. One process by which negative cognitive style may develop is through the explanations of events provided by caregivers, particularly mothers. Several studies have suggested that negative and critical maternal feedback is associated with depressogenic offspring cognitive styles (
8–
10). Mothers’ own cognitive style may also provide a model for the child to imitate (
11,
12); based on observations of their mother’s inferences about herself and circumstances, children will develop their own cognitive style.
However, there are also theoretical reasons for questioning whether there is any direct association between maternal and offspring cognitive styles. First, it is possible that a mother’s negative beliefs about herself are not sufficiently expressed in her behavior to be modeled. Second, it is possible that the child may use the mother’s attributions to reach diametrically opposite conclusions. For example, if the mother makes an external attribution and blames the child for her misfortunes, the child may learn to blame him- or herself (
8).
Although some studies report correlations between maternal and offspring cognitive style (
8,
13,
14), at least as many studies fail to find evidence for any association (
10,
15,
16). This inconsistency may reflect a failure to detect real associations because the studies were limited to cross-sectional designs (
14,
16) or had small sample sizes (<400) (
8–
10,
13). Previous studies have also measured mother’s cognitive style after the index child was born, thus failing to eliminate the possibility of reverse causality.
In addition, previous studies have limited their investigations to within childhood and early adolescence (
9,
10,
13). It is, however, important to understand the antecedents of cognitive styles that are carried into adulthood, where the main public health burdens of depression are manifest. Cognitive styles may also be open to changing influences (
10), and as the child develops, the mother may become less influential in comparison to peers (
17).
Finally, it is unclear whether the association between maternal and offspring cognitive styles is independent of maternal depression. Maternal cognitive style and maternal depression are strongly related (
18), and maternal depression is also a risk factor for offspring depressogenic cognitive style (
10). Part of this association may be explained by the cognitive style of depressed mothers. However, the effect of maternal depression could also operate through mechanisms that are unrelated to cognitive style. For example, maternal depression may act as adversity for the child or have an impact on the child’s cognitive style through its association with less sensitive parenting (
19).
In this study, we sought to improve on previous investigations by using data from over 4,000 families from the Avon Longitudinal Study of Parents and Children (ALSPAC) cohort in the United Kingdom to investigate the association between maternal cognitive style measured during pregnancy and offspring cognitive style 18 years later and how any such association was related to the association between maternal and offspring depression.
Method
Participants
The sample comprised participants from ALSPAC. All pregnant women residing in the former Avon Health Authority in southwest England who had an estimated date of delivery between April 1, 1991, and December 31, 1992, were invited to take part. The children of 15,247 pregnancies were recruited (
20). The representative nature of the original ALSPAC sample has been investigated by comparison with the 1991 National Census data of residents in the county of Avon (
20). Ethical approval for the study was obtained from the ALSPAC Law and Ethics Committee and the Local Research Ethics Committees. Written consent was obtained from all participants after they received a description of the study. Detailed information has been collected on the cohort since early pregnancy (
20; see also
http://www.alspac.bris.ac.uk). In this study, we used data from the subsample of ALSPAC singleton offspring who attended the research clinic at age 18.
Measures
Offspring cognitive style.
The Cognitive Style Questionnaire–Short Form (CSQ-SF), which was developed from the original Cognitive Style Questionnaire (
21) and has been shown to be reliable and valid for use in adolescents (
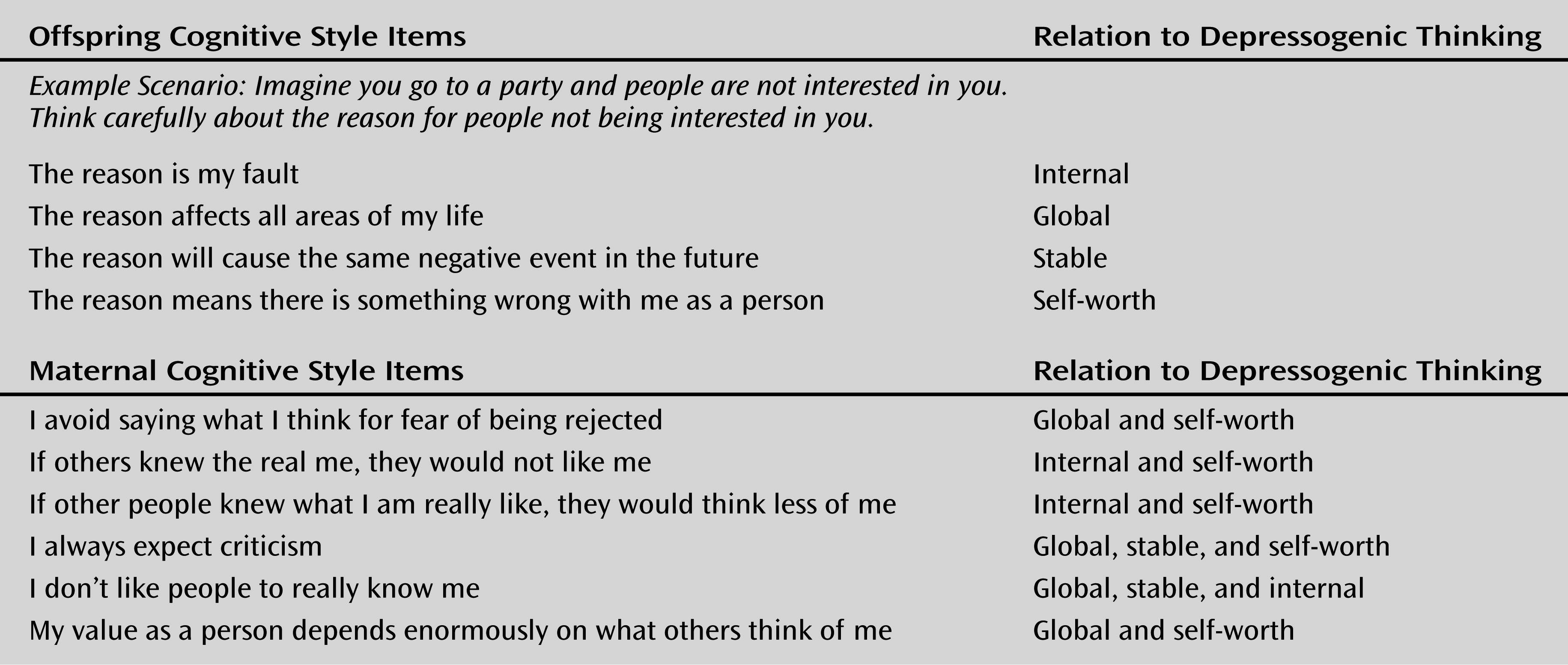
22), was administered to the ALSPAC children at the fourth Teen Focus Clinic (mean age: 17 years, 10 months). The CSQ-SF presents eight hypothetical events relating to failures in academic, employment, and interpersonal relationships. For each event, participants are instructed to vividly imagine themselves in that situation and think carefully about the reason for the event. Next, using a Likert scale of agreement from 1–5, participants rate the extent to which this reason was caused by internal versus external factors (themselves or others), specific versus global factors (has an impact on all areas or this specific situation), and stable versus unstable factors (will persist or not) and the extent to which it reflects their self-worth (means they are flawed) (
Figure 1). For each scenario, two items relate to each of the four dimensions, resulting in 64 items, with total scores ranging from 64 to 320. A fifth dimension relating to negative consequences was omitted from the CSQ-SF. Higher scores indicate a more negative style. Total scores showed a normal distribution, with a Cronbach’s alpha (measuring internal consistency) of 0.88, which is comparable to previous studies (
22). A principal-components analysis of the scores for the four dimensions indicated that a single factor with an eigenvalue of 3.25 explained 65% of the variance. All subscale scores loaded on this factor (loadings ranged from 0.37 to 0.85), which is comparable to previous studies (
22). We used CSQ-SF total score as the primary outcome variable.
A total of 4,693 adolescents completed at least one item on the questionnaire, and 3,387 completed all 64 items. For those who completed at least 75% of the items (equivalent to at least six of the eight scenarios), missing items were imputed from the individuals’ median scores across all other items in the subscale from which items were missing. Results are reported for the imputed scores. All analyses were repeated with complete item scores only, and the results were comparable (data available on request).
Maternal cognitive style during pregnancy.
A broader measure of intrapersonal sensitivity (
23) given to mothers as part of a questionnaire mailed out at 18 weeks of pregnancy was used to derive a measure of maternal cognitive style (
18). Six items relating to negative cognitions outlined in Beck’s cognitive theory of depression were selected on a theoretical basis in a previous study (
18). These items originated from the Dysfunctional Attitudes Scale, which has been validated against a reviewer-led measure of cognitive distortions using hypothetical stories (
24). Selected items were judged to measure negative cognitions according to Beck’s theory; two authors (G.L. and J.E.) selected these items independently. Items were excluded if they included words that were likely to be confounded by current mood, such as “worry” or “feel.” The internal consistency of the items was high (Cronbach’s alpha=0.77). Each item was rated for agreement on a 4-point Likert scale, with possible scores ranging from 0 to 3. Summed scores could range from 0 to 18, with higher scores reflecting more negative cognitions. A total of 12,175 mothers completed the six items, with a mean score of 4.6 (SD=3.4). Higher scores for mothers who were not currently depressed were predictive of future episodes of depression years after birth (
18). The negative cognitions endorsed by the mothers relate to the dimensions on the CSQ-SF. For example, to agree with the statement “I always expect criticism” reflects low self-worth, which, as indicated by the endorsement of “always,” is both a global and a stable attribution. As this measure was taken as an index of maternal cognitive style, it is referred to as such hereafter (see
Figure 1).
Confounding variables.
Variables previously shown to be associated with maternal and offspring cognitive styles were controlled for (
10). Maternal characteristics were derived from questionnaires given during pregnancy. These included age, education level, social class, (ranked from 1 to 5, with lower scores indicating higher status), parity, smoking during pregnancy, and depression measured using the Edinburgh Postnatal Depression Scale (
25) at 18 weeks of pregnancy on the same questionnaire from which the measure of maternal cognitive style was derived. The Edinburgh Postnatal Depression Scale is a 10-item self-report questionnaire specifically designed to screen for perinatal depression; scores >12 have been shown to have a high sensitivity (81.1%) and specificity (95.7%) in predicting major depressive disorder (
26). We also included offspring gender and offspring depression, which was measured with the Clinical Interview Schedule–Revised (
27) at the same research clinic as the CSQ-SF.
Offspring depression.
The Clinical Interview Schedule–Revised is a self-administered, computerized interview that establishes the severity of symptoms that constitute anxiety and depression disorders using algorithms based on ICD-10 criteria (
27). The version we used derives an ICD-10 diagnosis as well as symptom severity scores for depression, depressive thoughts, anxiety, panic, phobia, sleep, concentration, and fatigue, on a scale of 0–4. We used a binary variable (depressed, not depressed); cases were those with a primary diagnosis of mild, moderate, or severe depression using ICD-10 criteria. We also used a depressive symptom score derived by summing scores for depression, depressive ideas, poor concentration, sleep problems, and fatigue to account for subthreshold symptoms.
Statistical Analysis
We first examined the relationship between maternal cognitive style and offspring cognitive style in a series of linear regression models. The exposure variable was maternal negative cognitive style, treated as a continuous score. The outcome variable was offspring total CSQ-SF score. We examined a univariate model, then introduced potential confounding variables (maternal and offspring depression) separately into the model to investigate their impact on the main association. Although later maternal depression measures were available, they were not included in our models because of the strong correlation among timings of maternal depression. However, we repeated all analyses reported here with antenatal replaced by postnatal timing of depression and obtained comparable results (data available on request). There were no later measures of maternal cognitive style.
We examined a final multivariate model that included all confounding variables, and then we repeated the final multivariate analysis excluding mothers who exceeded thresholds for depression at the time they completed the cognitive style measure. Analyses were conducted using Stata, version 12 (StataCorp, College Station, Tex.).
Mediation analyses.
To investigate whether the association between maternal and offspring cognitive style mediated any association between maternal and offspring depression, we investigated the association between maternal and offspring depression before and after including cognitive styles and performed a mediation analysis using Mplus.
Missing data.
In a sensitivity analysis, we used multiple imputations to account for missing data. Given the availability of information on sociodemographic variables, we assumed that missingness is dependent on observed data and used multiple chained equations using all study variables and sociodemographic indicators to impute 30 data sets. We then repeated analyses across the imputed data sets combining estimates using Rubin’s rules (
28). Given the difficulty in imputing missing outcomes (
28), we initially imputed only up to the sample for which complete cognitive style (CSQ-SF) outcome data were available (N=3,845). However, given the association between CSQ-SF and mood, we used five earlier measures of mood to predict CSQ-SF and repeated the imputation model up to a starting sample with at least one measure of mood or temperament as well as exposure (N=10,322). This model should be interpreted with caution, however, as our ability to predict CSQ-SF scores was limited.
Results
A total of 3,845 offspring provided useable data on the CSQ-SF at age 18. From this sample, 3,320 of their mothers had provided maternal cognitive style data during pregnancy. This sample was further reduced to 2,528 mothers and children for whom complete data for all confounding variables were available. Demographic characteristics for the sample with complete data as compared with the rest of ALSPAC are summarized in
Table 1.
Associations With Offspring Cognitive Style
Mean offspring cognitive style (CSQ-SF) scores, by level of maternal cognitive style, are presented in
Table 2. Linear regression analyses provided evidence for a positive association between maternal and offspring cognitive style. This association held in the sample for whom complete data were available for confounding variables after we included adjustments for maternal and offspring depression and additional confounding variables, excluding mothers who were depressed at baseline, and imputing missing data (
Table 3). There was also evidence for a univariate association between maternal depression and offspring cognitive style. For a one-standard-deviation increase in maternal depression score, offspring cognitive style score increased by 1.28 points (95% CI=0.40–2.17; p=0.005). However, the increase fell to 0.17 (95% CI=–0.002 to 0.36; p=0.09) after adjustment for maternal cognitive style.
Associations With Offspring Depression and Mediating Role of Cognitive Styles
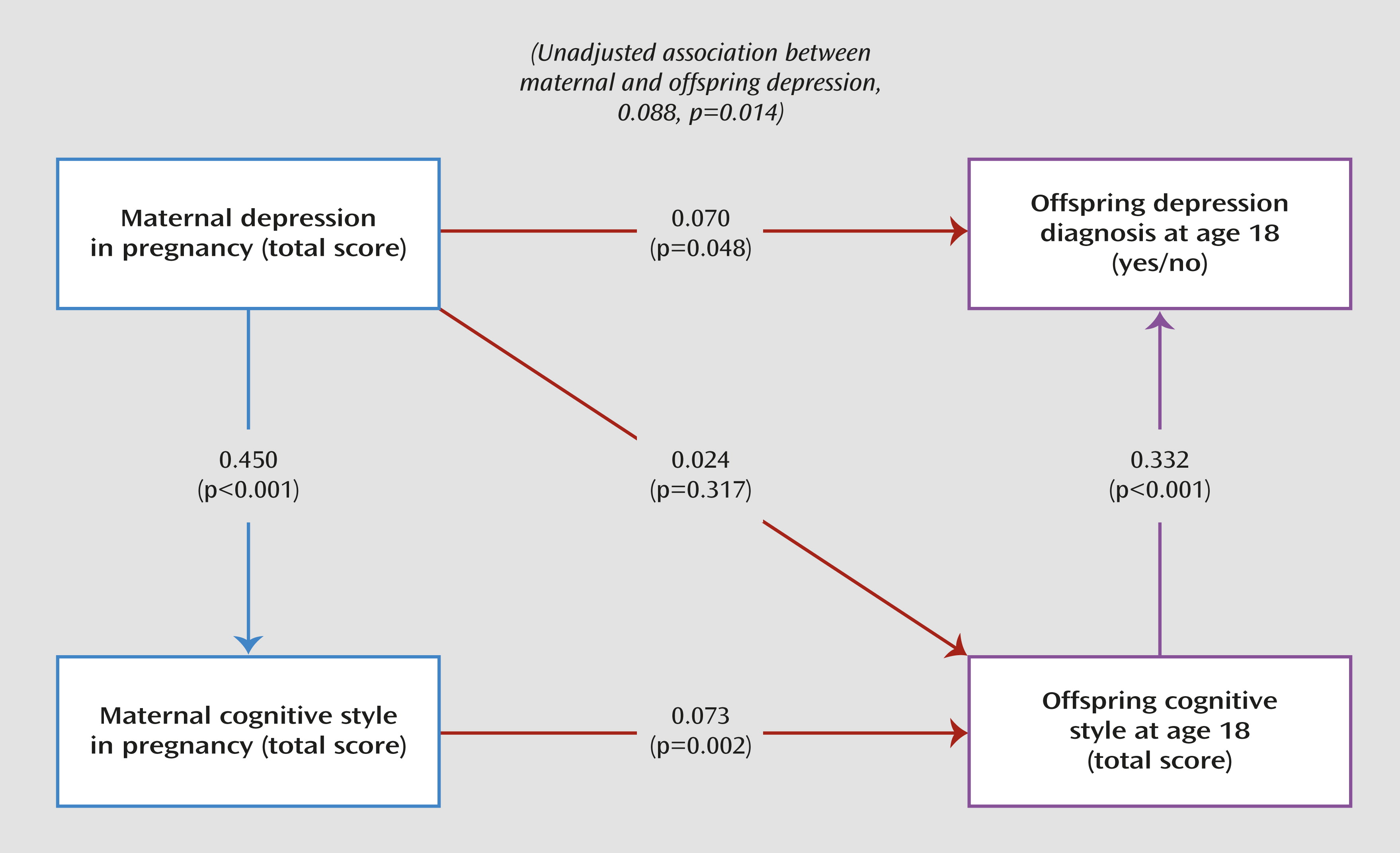
Cognitive style scores for depressed offspring were 14 points (0.8 standard deviations) higher (95% CI=12–18; p<0.001) than those for their nondepressed peers. There was also an association between maternal cognitive style and offspring depression (odds ratio=1.18, 95% CI=1.01–1.40; p=0.049), which was reduced after adjustment for offspring cognitive style (odds ratio=1.10, 95% CI=0.93–1.31; p=0.248). Finally, there was an association between maternal depression and offspring depression. For a one-standard-deviation increase in maternal depression score, the odds of offspring depression were increased by 23% (odds ratio=1.23, 95% CI=1.04–1.44; p=0.013). This association was reduced after maternal and offspring cognitive styles were included in the model (odds ratio=1.15, 95% CI=0.96–1.39; p=0.138). As shown in
Figure 2, mediation analysis provides evidence that 21% of the association between maternal and offspring depression was mediated by maternal and offspring cognitive styles.
Discussion
An increase of approximately one standard deviation in maternal cognitive style score during pregnancy was associated with an increase of approximately 0.1 standard deviations in offspring cognitive style score at age 18. The small effect size may explain previous inconsistent findings because it suggests that this association may have been missed in smaller studies lacking sufficient statistical power. Our analyses provide evidence that maternal and offspring cognitive styles explained 21% of the association between maternal and offspring depression. It is striking that the association between maternal and offspring cognitive styles should remain despite the possible reduction in maternal influence as the child ages and the potential for the mother’s cognitive style to change through the child’s life.
Strengths and Limitations
Strengths of the study include the large sample size, the long-term follow-up spanning the life of offspring from before birth into adulthood, and the availability of confounding variables, particularly concurrent measures of both maternal and offspring depression.
A limitation of the study is the loss to follow-up from the original sample. Young adults who attended the clinic at age 18 were less likely to come from poorer families. However, sensitivity analyses accounting for missing data provided no evidence that missing data introduced bias. Another limitation is that the measurement of maternal and offspring cognitive style differed. The maternal measure related to negative cognitive style in general, whereas the offspring measure involved attribution of cognitive styles to hypothetical events. According to cognitive theories, the two measures should reflect the same underlying constructs. For example, if a mother always expects criticism, it seems reasonable to infer that this outlook would be applied to the attributions of negative events. Nonetheless, there was likely to have been considerable measurement error in measuring cognitive styles, for the maternal measure in particular; some subjects with negative cognitive styles may not have reported this in the few questions available, in which case their score on the measure would not accurately reflect their cognitive style. This will have added noise to the data, likely leading to an underestimate of any association.
There are also several questions that our findings cannot answer. For example, the stability of maternal cognitive style throughout the child’s life was unclear, which limits our understanding as to
when it influences the child. Furthermore, the lack of a parenting measure limits our understanding as to
how maternal cognitive style influences the child. Finally, although previous studies have reported limited heritability of depressogenic cognitive styles (
6,
29), unmeasured shared genetic factors may also explain part of the association.
Mechanisms
One explanation for the association between mother and offspring cognitive styles is that negative cognitive style is a marker for depression and therefore the results reflect the established association between maternal and offspring depression (
12,
30). However, the association remained after adjustments for maternal and offspring depression, indicating that this is not a likely explanation. In contrast, maternal and child cognitive styles mediated a significant part of the association between maternal and offspring depression. Because maternal depression and maternal cognitive style were measured on the same occasion, we cannot determine the direction of causality. Previous evidence suggests that cognitive style leads to depression (
18); however, depressed states could also lead to negative cognitive style. Whichever way the association is initially brought about, the important point is that maternal depression and cognitive style were strongly correlated in pregnancy and that the association with cognitive styles partially explained the effects of maternal depression. Transmission of cognitive styles is therefore one potential pathway from maternal to offspring depression that is modifiable and would provide a target for prevention. Furthermore, maternal cognitive style was associated with offspring cognitive style irrespective of maternal depression. Thus, maternal cognitive style is a potential target for prevention of offspring depression even if the mother is not depressed at that point.
Interventions
There are two possible strategies that might prevent the transmission of cognitive styles. First, maternal cognitive style could be modified. For example, cognitive therapy is designed to modify cognitive styles, and evidence suggests that it has a lasting positive influence on cognitive style (
31). As described above, it is also possible that maternal depression leads to negative cognitive styles, and thus in depressed mothers antidepressant treatment could prevent development of a negative cognitive style. Second, rather than focusing on changing the mother’s cognitive style, interventions could focus on preventing transmission by changing what a mother says and how she behaves. To prevent the imitation of cognitive styles, interventions could work on preventing mothers from providing examples of negative cognitive style. For example, commenting that the child’s
act was bad rather than that the
child is bad would be modifying a global and personal attribution that is specific and external. Negative maternal cognitive style may also result in less specific forms of negative parenting, which may also need to be targeted (
32). For example, mother-child interventions such as video feedback have been shown to modify mothers’ expression of negative language and behavior and increase responsiveness (
33). Finally, a mother may apply her negative beliefs to her interpretation of child behavior: a mother who always feels criticized may perceive that—and act as though—her child is critical of her (see the second patient perspective). Children who are told that they hold negative and critical thoughts may come to believe that they are negative people. In this case, interventions could work on improving the mother’s awareness of the child’s mental processes, or mind-mindedness (
34). For example, changing a mother’s focus to her child’s rather than her own mental states may help her act appropriately to the child’s needs.
Conclusions
To our knowledge, this is the first study to provide evidence for an influence, persisting into early adulthood, of a mother’s cognitive style on her offspring’s cognitive style. The effect size is relatively small, but given the dose-response relationship, the 18-year longitudinal time frame, the low-risk sample, and potential measurement error resulting in underestimation of any associations, such an effect is likely to be meaningful. The mechanisms underlying this effect remain to be established, although the findings suggest that modifying maternal cognitive style irrespective of the current presence of maternal depression could help prevent the development of a depressogenic cognitive style in offspring. Given the association between cognitive style and clinical levels of depression in this and other studies (
35), these findings provide another possible route to preventing depression.
Acknowledgments
The authors are grateful to the families who took part in the study, the midwives for help in recruiting them, and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists, and nurses. Patient Perspectives were provided in collaboration with J. Cassidy and E. Meins.