A Critical Appraisal of Neuroimaging Studies of Bipolar Disorder: Toward a New Conceptualization of Underlying Neural Circuitry and a Road Map for Future Research
Abstract
Objective
Method
Results
Conclusions
The Scope of Neuroimaging Studies in the Review
Major Themes That Emerge From Neuroimaging Studies
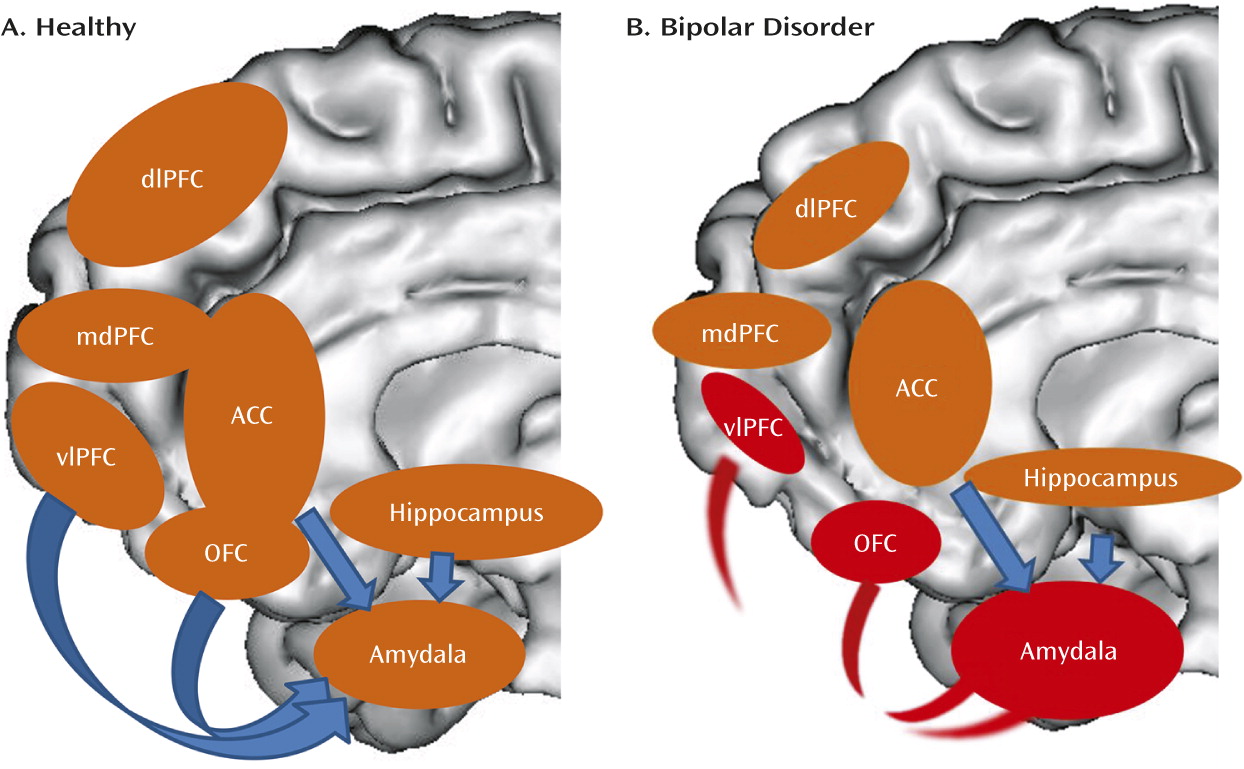
Theme 1: Abnormalities in Emotion-Processing and Emotion-Regulation Neural Circuitry
| Theme 1 | Abnormally decreased ventrolateral prefrontal cortex activity during emotion processing, emotion regulation, and response inhibition (9–19) |
|---|---|
| Theme 2 | Abnormally increased amygdala, striatal, and medial prefrontal cortical activity and decreased functional connectivity between amygdala and prefrontal cortex, to positive emotional stimuli (9, 10, 20–22) |
| Theme 3 | Abnormally increased amygdala, orbitofrontal cortex, and temporal cortical activity during nonemotional, cognitive task performance (23–28) |
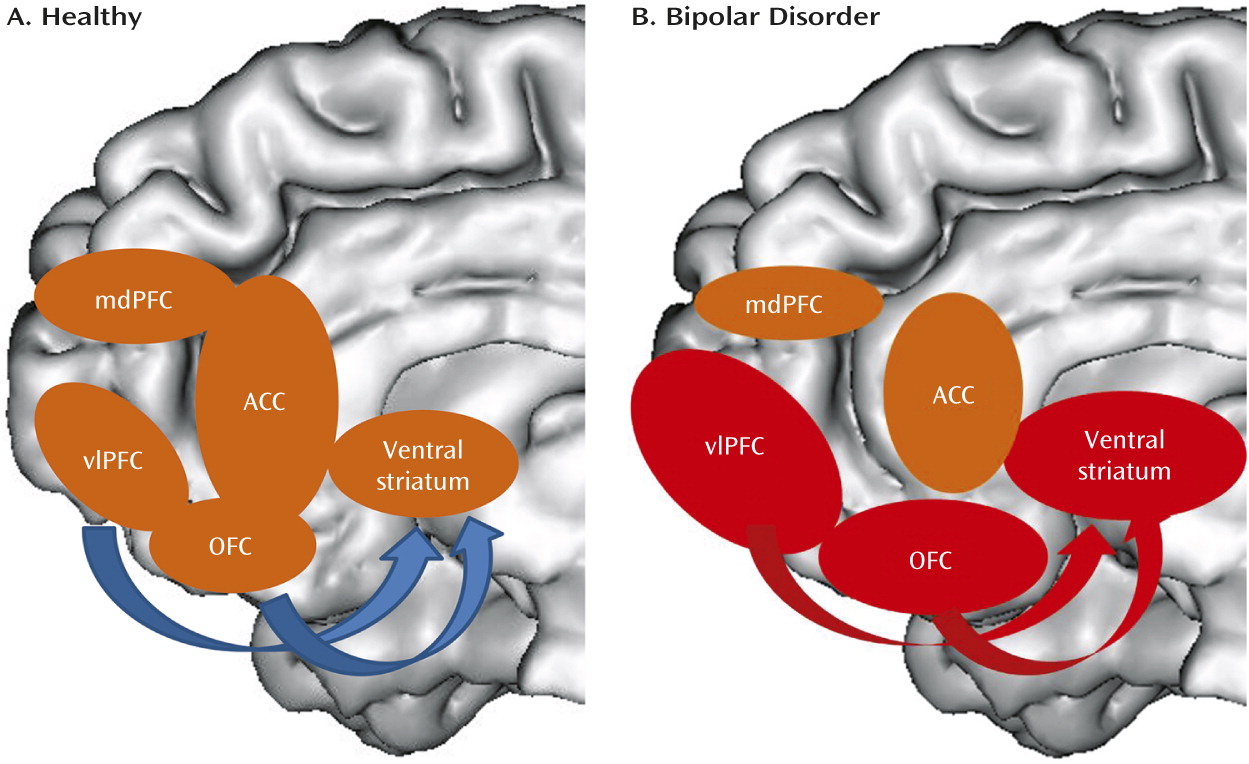
| Theme 4 | Abnormally increased left ventrolateral prefrontal cortex and orbitofrontal cortex, and ventral striatum activity during reward processing (40–45) |
Theme 2: Abnormal Activity in Emotion-Processing Circuitry to Positive Emotional Stimuli
Theme 3: Abnormal Activity in Emotion-Processing Neural Circuitry During Performance of Nonemotional Tasks
Theme 4: Abnormalities in Reward-Processing Neural Circuitry
Structural Neuroimaging Studies Providing Support for the Main Themes
| Main findings from structural neuroimaging studies supporting the main themes from functional neuroimaging studies |
|---|
| Cortical findings |
| Decreased gray matter volume, decreased white matter volume, and decreased cortical thickness in prefrontal, anterior temporal and insula cortices. Decreased gray matter volume in particular in right ventrolateral prefrontal cortex and orbitofrontal cortex (49–65) |
| Subcortical findings |
| Decreased volume of amygdala and hippocampus. Altered striatal volumes (55, 56, 60, 63, 65–74) |
| Main findings from diffusion imaging studies supporting the main themes from functional neuroimaging studies |
| White matter tract findings |
| Altered fractional anisotropy, and increased radial diffusivity, in frontally situated white matter (51, 56, 75–103) |
Diffusion Imaging Studies Providing Support for the Main Themes
Conceptualizing Bipolar Disorder in Terms of Abnormalities in Large-Scale Neural Circuits
Neuroimaging Research Needed to Support This Conceptualization of Bipolar Disorder Neural Circuitry
Mood State-Specific Functional Abnormalities in Circuits Supporting Emotion Processing, Emotion Regulation, and Reward Processing
Intrinsic (Resting-State) Connectivity Studies
Future Neuroimaging Research in Bipolar Disorder
Limitations of Extant Studies
Newer Research Areas
Neuroimaging studies of different bipolar disorder subtypes.
Neuroimaging studies comparing bipolar disorder with other major psychiatric disorders.
Multimodal neuroimaging studies.
Neuroimaging studies in youths with bipolar disorder and those at risk for bipolar disorder.
Neuroimaging studies adopting dimensional approaches.
Neuroimaging studies using pattern recognition approaches.
A Neuroimaging Research Road Map For Bipolar Disorder
| Strategy 1: Dimensional approaches | Dimensional approaches to identify emotion-processing, emotion-regulation, and reward-processing neural circuitry abnormalities associated with dimensions of pathological behaviors that cut across conventionally defined bipolar disorder and other mood disorder diagnostic categories. The inclusion of longitudinal designs will help identify the extent to which alterations in these circuitry abnormalities are associated with changes in affective state. |
|---|---|
| Strategy 2: Developmental studies | Longitudinal follow-up studies examining developmental trajectories of these neural circuits in individuals with bipolar disorder across the lifespan and in youths at risk for mood disorders |
| Strategy 3: Multimodal neuroimaging and systems-level approaches | Multimodal neuroimaging studies and studies adopting biological system-level approaches to examine the impact of genetic variation and molecular-level processes on neural circuitry development in at-risk individuals and individuals with bipolar disorder and other mood disorders |
| Strategy 4: Techniques to identify individualized patterns of neuroimaging measures | Studies using neuroimaging in combination with pattern recognition techniques to identify individual-level neural circuitry markers that help classify individuals into diagnostic groups and help predict individual-level future clinical course |
| Strategy 5: Combinations of the above strategies | These studies will a) help elucidate more complex neuropathophysiological processes underlying dimensions of abnormal behaviors associated with affective pathology across different diagnostic categories; and b) yield individual-level biological markers reflecting these processes with clinical utility for diagnosis, predicting future illness development, and guiding personalized treatment choice. |
Footnote
Supplementary Material
- View/Download
- 163.88 KB
References
Information & Authors
Information
Published In

History
Authors
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).