“Aaron,” a 17-year-old high school junior living with his father and younger brother, was referred for an evaluation in a university-based research program for individuals at clinical high risk for psychosis. He had undergone three brief inpatient stays, prompted by his father’s concern about his suspicion and unusual behaviors (e.g., flipping light switches to let others know he was home) and a sudden decline in academic performance. In 10th grade, he earned a 3.75 grade point average for the fall term but then failed most of his classes in the spring term. During his initial hospitalization, he was treated with ziprasidone (80 mg b.i.d.) for 4 days before it was discontinued.
Aaron was evaluated with the Structured Clinical Interview for DSM-5 and the Structured Interview for Psychosis-Risk Syndromes. He endorsed several items reflecting unusual thought content and subsyndromal delusional beliefs that had begun over the past 6 months. He reported that almost every day he wondered if what he’s watching on TV is a “message just for me.” He had also wondered whether people knew things about him even though they could not read his mind. For example, he had the feeling that people knew he had Alzheimer’s disease (which he worried he may have). At times he wondered if he might not exist, or he asked himself, “Is this real, or are we all in pods?” In the interview, he linked the notion of pods with the film Inception, in which the characters move through shared dream worlds. Notably, Aaron was able to spontaneously question his conviction in these thoughts, and he noted that he had always had an active imagination. When asked if he could think of other reasons for thinking people might be looking at him or thinking he had a disease, he was able to state that he had styled his hair into a Mohawk that day and they may have been looking at that.
Also within the past 6 months Aaron noted the onset of suspiciousness and paranoia. He started to feel as if his girlfriend was cheating on him, because of frequent calls to her cell phone. His suspiciousness, at least partially, caused the breakup of the relationship. After the breakup, he began to feel that his girlfriend might be trying to kill him or have him killed. He reported seeing a car drive by his school and thinking that the occupants had guns and were there to kill him (on his girlfriend’s orders). He also thought that she may have tried to poison him just before the break-up when she gave him some alcohol and marijuana. It was at this point that Aaron began to experience some perceptual changes, thus leading to the thought that he may have been poisoned. Because of his suspicions, Aaron began to isolate himself from others, rarely leaving home. He reported at the time of his interview that he did not feel as suspicious as he had previously, but he continued to be vigilant of his surroundings. Without prompting, Aaron remarked that he always questioned whether or not he was just imagining all this.
Aaron also showed signs of grandiose thinking, stating that he was “going to be big someday.” He stated that he had come up with a “time travel thing” and that he was going to be able to go back in time and help people (after getting clues from people in the present that others were in need of help). He also spoke about his writing abilities and his skills with virtual reality gaming. The grandiose thinking was determined to be part of hypomania (1- to 2-day periods when he needed less sleep than usual, felt more confident, and had more energy, ideas, and motivation) that he had experienced intermittently over the past 2 years.
During this same time frame, Aaron reported hearing random ringing sounds approximately once a month. He heard his girlfriend’s voice on two occasions when no one was there. He questioned the reality of these sounds. He also mentioned seeing dark areas out of the corner of his eye several times a week. He thought these might be spirits or just visual abnormalities. He reported having some experiences of tingling down the middle of his back and feeling cold for no reason. He was not sure how to explain this, had insight that it was likely a misperception, and was not distressed by these experiences.
During the evaluation, Aaron was noted to have linear thoughts and carry on a clear, coherent conversation with no evidence of disorganization of thoughts.
History
Aaron’s past psychiatric history was significant for a diagnosis of attention deficit hyperactivity disorder at age 7 and treatment with stimulants for an unknown period with unclear response. At age 15 he was treated with bupropion (up to 300 mg/day) for a major depressive episode in which he felt down and depressed, with periods of low energy, not wanting to get out of bed, low self-esteem, and suicidal thoughts. During treatment with bupropion, he developed what appears to have been a mixed mood state with grandiosity, irritable mood, decreased need for sleep, high energy, racing thoughts, and suicidal ideation. Aaron’s history was also significant for 1- to 2-day periods of hypomania since age 15 in which he would develop increased self-confidence, grandiose beliefs, risk taking, and decreased need for sleep. His medical history included no surgery, hospitalizations, major illness, or head injury. As for substance use, he reported daily use of cannabis for the past year.
Aaron’s developmental history was significant for parental divorce when he was 6 years old. He and his siblings lived with their mother after the divorce. Aaron endorsed a history of emotional neglect, psychological abuse, and physical abuse. His older brother died of a self-inflicted gunshot when Aaron was 9. His mother was addicted to intravenous drugs during Aaron’s early adolescence, and he witnessed her near death from overdose when he was 14. Aaron went to live with his father briefly at age 14 but had to be placed in foster care when he was ages 15–16 because his father could not care for the other children because of his sister’s chronic illness and subsequent death when Aaron was 16. Aaron suffered both psychosocial and physical bullying during adolescence. After his sister’s death, he went back to live with his father, where he was living at the time of initial evaluation.
As for family psychiatric history, Aaron’s mother was diagnosed with bipolar disorder (with possible psychosis) and has an extensive substance use history. His maternal aunt was diagnosed with schizophrenia, and his older brother died by suicide at age 18.
Aaron comes from a lower-middle-class family and attends school in a neighborhood known for gang activity. He had been a good student up until the previous semester, when his functioning declined. He had friends and had dated, but he had become more isolated. He enjoyed video games and watching movies. He admitted to having an active imagination.
Diagnosis
Aaron’s DSM-5 diagnoses were bipolar II disorder; attention deficit hyperactivity disorder, combined presentation; and other specified schizophrenia spectrum and other psychotic disorder: attenuated psychosis syndrome. His Global Assessment of Functioning Scale (GAF) score was 44 (in the past year, his highest GAF score was 80 and his lowest was 20).
Neuropsychological Assessment
Aaron underwent a comprehensive neuropsychological assessment shortly after his initial clinical assessment (Table 1). Tests administered included the MATRICS (Measurement and Treatment Research to Improve Cognition in Schizophrenia) Consensus Cognitive Battery, subtests of the Wechsler Abbreviated Scale of Intelligence, and the reading subtest of the Wide Range Achievement Test, 4th edition. Aaron’s performance on most tests was within the low average to average range, except for verbal learning, which was within the borderline range.
Follow-Up Assessments
Aaron was seen again 1 month after the initial evaluation. He was still in high school and was looking for a job. He reported some mild depression and continued suspiciousness, perceptual changes, and idiosyncratic beliefs. He declined the recommended mood stabilizer (lithium was the first choice) but was in supportive psychotherapy with a therapist in the community once per week. His father had moved away, and Aaron was staying with friends.
After the initial 1-month follow-up, Aaron was lost to follow-up and did not return to the university-based program until 14 months later. He had dropped out of psychotherapy and had not received any psychiatric care until he was hospitalized 9 months after the initial evaluation for a full psychotic episode. The hospitalization was the result of extreme paranoia mixed with auditory hallucinations. He was brought to the attention of authorities by concerned friends who believed that he could not discern reality.
Aaron reported that during the hospitalization he was treated with injections of haloperidol (4 mg), lorazepam (1 mg), and benztropine (2 mg). Although he received prescriptions for these medications at discharge, he did not fill them and had not taken any medication since his discharge.
Aaron’s hygiene had dramatically deteriorated since the initial evaluation; he presented with stained clothing and severe body odor. He was living on the couch at a friend’s home. He assisted this friend working in a shop several hours a week in exchange for housing. He was not otherwise employed. He had had several temporary housing arrangements since his initial evaluation, including living with his father for a few months and with a girlfriend for 3 months. He denied any drug or alcohol use and smoked less than five cigarettes a day.
Aaron reported that before the hospitalization he had begun to believe that he was hearing the voice of God and that God was telling him to proselytize “his word” to others. He experienced this voice as being real and as coming from outside his head. He also felt a “hot sensation” on his chest area when he talked about God. He began to preach to others, but after a while he became frightened when he believed that he was changing others’ religious beliefs and that God and others would come to view him as the “anti-Christ.” Because of this fear and the anticipated punishment from God, he stopped talking to others about God’s views. Aaron also believed that he was able to communicate with others through “hugs” and that through a hug he could know the other person’s entire “mind and spirit.” He was convinced of his ability to do these things, and no insight could be induced. At the same time, Aaron became fixated on the idea that his girlfriend of 6 months was cheating on him. He acknowledged that he had no true evidence to suggest her infidelity, but reported spending up to 6 hours a day doing Internet searches trying to “find something” on her. He repeatedly followed her and confronted her about her infidelity, despite her denial. This led to her concern about his mental health, his hospitalization, and the demise of their relationship.
Aaron continued to be extremely suspicious. He believed that he was unsafe standing on his front porch and that he might get shot if he did so. He also believed that there was an “entity” that prevented him from feeling safe (which could be God). He believed that he had unique theories of the world that would change the way the human race lives, including ideas about time travel and religion, but did not want to share the exact nature of these theories for fear the interviewer would steal them. Aaron’s communication was very disjointed, displaying disorganization of thought. He was eventually able to respond to short questions but had to be redirected numerous times. (Q: “How much do you work each week?” A: “Oh, that’s what happened with Billy [his friend]! I work with the owner and she saw me one day and said, ‘You! You know Billy!’” Q: “Where are you living now?” A: “I was living with this girl, but she broke all my guitars and then I couldn’t play my music.”
Aaron’s GAF score was 33 (his past-year high and low scores were again 80 and 20, respectively). After conversion to psychosis, Aaron received repeat neuropsychological testing. His performance was stable in some domains, but he demonstrated a significant decline in verbal learning, working memory, and speed of information processing (Table 1). Moreover, his overall IQ, a relatively stable measure across time, declined from average to low average.
It was determined that Aaron had had his first psychotic break 9 months after the initial interview and had remained psychotic without treatment. He had received psychotherapy for a month after his initial assessment and then went 8 months with no treatment of any kind. At the time of his follow-up assessment, it was determined that he met the criteria for schizoaffective disorder, bipolar type, since he had ongoing psychotic symptoms that were independent of mood episodes.
TABLE 1. Neuropsychological Data for a Patient With Attenuated Psychosis Syndrome
Wechsler Abbreviated Scale of Intelligence, vocabulary subtest
54
10
48
8
Visuospatial functioning
Wechsler Abbreviated Scale of Intelligence, block design subtest
59
13
47
8
Wechsler Abbreviated Scale of Intelligence, IQ
109
89
Reading, spelling, math
Wide Range Achievement Test, 4th ed.
84
81
a
Borderline.
b
Impaired.
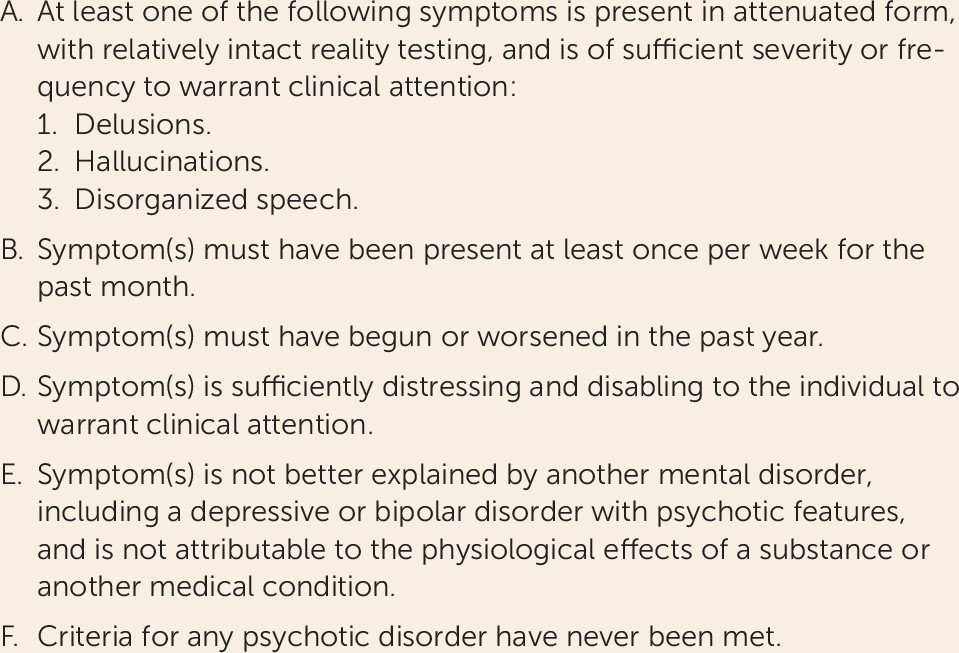
The vignette illustrates the case of an adolescent who initially presented with the recent onset and worsening of subsyndromal psychotic symptoms, suggestive of attenuated psychosis syndrome, the newly proposed psychosis risk syndrome included in DSM-5’s section “Conditions for Further Study” (Figure 1). Notably, he initially had some insight that these symptoms and thoughts may not be real, indicating that he had not crossed the threshold for a full-blown psychotic episode according to the Structured Interview for Psychosis-Risk Syndromes and other structured diagnostic instruments developed to identify and define the psychosis risk syndrome (sometimes referred to as clinical high risk, ultra high risk, attenuated psychotic symptoms). As part of the structured interview, the degree of insight is assessed in terms of whether the person spontaneously brings up doubt about his or her altered perceptions, for example, or whether insight needs to be elicited by the interviewer. It is also important to determine whether there has ever been a time when the individual lost insight and may have been fully psychotic. The diagnostic evaluation of a patient with suspected clinical high risk frequently requires extensive collateral information to tease out the often nuanced symptoms in the prodromal period and differentiating not only psychosis from prodrome but also prodrome from normal adolescent behavior. As is common with the onset of new psychotic-like symptoms in an adolescent, there is a gray zone between an active imagination and magical thinking, referential thoughts, and suspiciousness. Additionally, adolescents are novelty seeking (with developing dopamine receptors and not yet fully connected prefrontal cortices) and are likely to experiment with substances, find new peer groups, and explore their understanding of the world. A careful history that assesses family and social background along with cultural and spiritual history is important to put the newly emerging symptoms in context.
FIGURE 1. DSM-5 Proposed Criteria for Attenuated Psychosis Syndromea
a Reprinted from American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Washington, DC, American Psychiatric Association, 2013, p. 783. Copyright 2013, American Psychiatric Association. Used with permission.
Approximately one-third of individuals who meet the clinical high risk criteria will transition to full psychosis within 2 years. Those who do not make this transition are very likely to develop other mental disorders and remain functionally impaired (1). Aside from his symptoms, Aaron also presented with a number of risk factors for psychosis, including a family history of mental illness, childhood trauma, behavioral problems, verbal learning difficulties, substance use, and a decline in both role and social functioning. Overall, Aaron’s neuropsychological profile is consistent with the verbal learning and attentional problems described in youths at clinical high risk relative to healthy comparison subjects. Cognitive impairment in youths at clinical high risk is also associated with subsequent conversion to psychosis (2). Specifically, declines in verbal abilities (memory in particular), working memory, processing speed, and intellectual functioning have all been associated with later conversion to psychosis. Also, as commonly seen in individuals at clinical high risk, Aaron was help seeking, he had already received a variety of interventions, and the differential diagnosis was broad. Collectively, these risk factors for psychosis, along with moderately severe subsyndromal psychotic symptoms, put Aaron at high risk for a psychotic illness.
Risk Factors For Psychosis and Conversion To Psychosis In Youths at Clinical High Risk
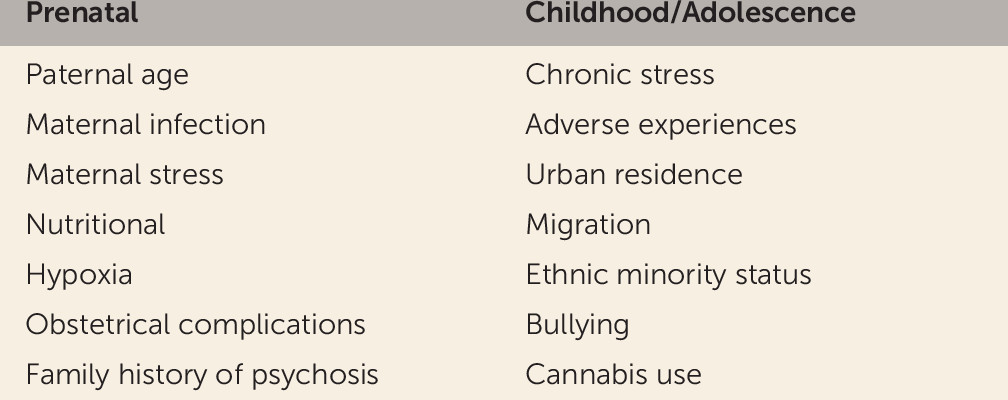
Along with family history of psychosis, a number of environmental risk factors have been shown in epidemiological studies to be associated with an elevated risk for psychosis (Figure 2). While many of the environmental risk factors may affect the developing fetus, others appear to be “second hits,” occurring in childhood or later adolescence. Theoretically, the second hits may act by epigenetic modulation of the genome in individuals who already have a genetic vulnerability, or they may potentiate biological pathways implicated in psychosis.
FIGURE 2. Risk Factors for Psychosis
Studies of risk factors for later conversion to psychosis in youths at clinical high risk have identified stressful life experiences (3), bullying (3), decline in social functioning (4), neurocognitive deficits (5), and drug use (4) as risk factors that, along with the clinical symptom criteria, may contribute to the development of an algorithm of psychosis risk. Much like diagnostic tools used to estimate risk for heart disease or cancer, a “psychosis risk predictor” could be used in the clinical setting to determine which individuals are at greatest risk and in greatest need of specific interventions.
Pathophysiology Of Early Psychosis
A number of interconnected neuropathological mechanisms, including increased hypothalamic-pituitary-adrenal axis (HPA) activity, neuroinflammation, N-methyl-d-aspartate (NMDA) receptor hypofunction, and reduced neuroplasticity, have been implicated in early psychotic illness and will be important domains of study as we move forward in the development of preemptive treatment in the prodromal phase of psychotic illness.
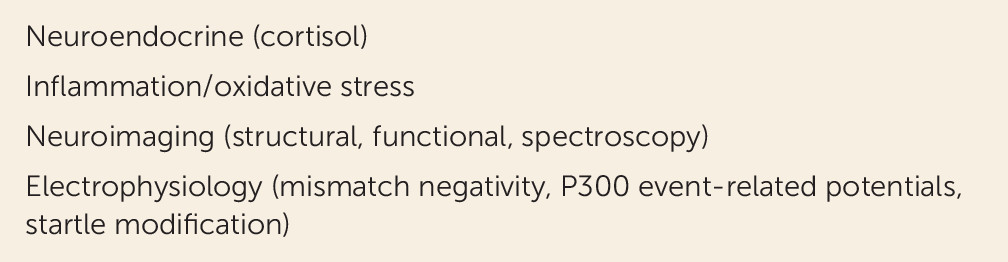
Ongoing research in youths at clinical high risk has also focused on identifying biomarkers that can be used for a variety of purposes, including 1) for understanding the neuropathological mechanism by which psychosis evolves, 2) as diagnostic markers to further identify those at highest risk, 3) for individualizing treatment, 4) for translational research, and 5) as surrogate endpoints in treatment studies. A number of promising biomarkers have been identified that predict risk for psychosis in youths at clinical high risk and provide insight into early neuropathological mechanisms (Figure 3), including elevated levels of salivary cortisol (6), elevated markers of inflammation and oxidative stress (7), accelerated loss of gray matter (8), thalamic dysconnectivity (9), brain glutamate measured with proton magnetic resonance spectroscopy (10), and reductions in event-related potentials (11).
FIGURE 3. Types of Biomarkers for Psychosis
Increased HPA activity is associated with psychotic disorders and exposure to stressful life events and may increase the activity of dopamine pathways (12). It has been postulated that early-life exposure to infection or inflammation has the potential to induce latent neuroinflammatory abnormalities that can be unmasked by exposure to stressful stimuli (13), activating microglia and enhancing the production of proinflammatory cytokines in the CNS (14). Animal models have demonstrated that the neurodevelopmental effects of prenatal infection or inflammation can lead to later brain and behavioral changes that can be attenuated by interventions targeting inflammation or associated physiological processes such as oxidative stress (15), suggesting possible directions for early intervention in individuals at clinical high risk with evidence of neuroinflammation.
Studies in individuals with schizophrenia and those at clinical high risk have shown gray matter volume reductions in multiple brain regions, including the prefrontal cortex and the superior and medial temporal lobes (16). In individuals at clinical high risk, Cannon et al. (8) found that those who converted to psychosis showed a steeper rate of gray matter loss in the right superior frontal, middle frontal, and medial orbitofrontal cortical regions, regardless of antipsychotic use. Importantly, gray matter loss was predicted by plasma levels of proinflammatory cytokines. The neuroanatomical changes in schizophrenia appear to be progressive changes beyond those associated with normal development (17). Cortical gray matter density declines normally during late adolescence, resulting in decreased neuropil in the same brain regions implicated in the pathophysiology of schizophrenia (18). It is likely that pre- or perinatal neurodevelopmental abnormalities can lead to a vulnerability to postpubertal insults that contribute to the accelerated loss of gray matter and aberrant connectivity in the prefrontal regions of vulnerable individuals. Factors such as substance abuse, stress, and HPA axis dysregulation may contribute to a later neurodegenerative process.
Recent studies using proton magnetic resonance spectroscopy (10) have identified neurometabolic changes, including dysregulation of glutamate prior to the onset of psychosis, in individuals at clinical high risk. While the dopamine hypothesis has been a useful model in our understanding of psychosis, it does not explain the accelerated gray matter loss and the deteriorating course in terms of cognition and function seen in the first few years of psychosis. Glutamate antagonists are well known to induce positive and negative psychotic symptoms more akin to schizophrenia than the positive symptoms induced by dopamine agonists alone (19), and it has been proposed that dopaminergic dysregulation is the final common pathway resulting from an altered glutamatergic neurotransmission early in the course of illness (20). According to glutamatergic theories, the abnormal developmental trajectory could result from reduced elaboration of inhibitory (GABA-ergic) pathways and excessive pruning of excitatory (glutamatergic) pathways leading to altered excitatory-inhibitory balance in the prefrontal cortex (21). Glutamatergic theories of schizophrenia suggest that an increase in cortical glutamatergic activity, due to genetically or environmentally mediated hypofunction of NMDA receptors, may lead to a time-limited neurotoxic process and dopaminergic dysregulation at the onset of psychosis (20).
Thus, while disturbances of neurodevelopment early in life may be necessary for the future emergence of psychosis, environmental influences during late adolescence may contribute to the emergence of psychosis via a range of possible mechanisms, including inflammation and glutamatergic or dopaminergic transmission, which are all potential targets for early intervention.
Early Intervention In The Psychosis Risk Syndrome
Differential Diagnosis
There is no “one size fits all” intervention for patients who meet the clinical high risk criteria. Clearly, remaining open to a broad differential diagnosis is critical at this point. Newly emerging symptoms could be part of a bipolar disorder with psychotic features, substance use disorder, posttraumatic stress disorder, an anxiety disorder, a schizophreniform disorder, or schizoaffective disorder. “Broad-spectrum” treatments that can target the presenting symptoms, safely modulate a potentially emerging illness, reduce stress, and enhance functioning are key.
Psychoeducation
Newly emerging subsyndromal psychotic symptoms in adolescence and early adulthood are often vague and nonspecific. Families and the affected individuals are typically help seeking and have identified a stressor or complaints that should be the focus of early education. Given that less than one-third of individuals who meet clinical high risk criteria will go on to develop a psychotic illness (22) but a far greater proportion will go on to be functionally impaired, the emphasis of initial education should not be on risk for psychosis but rather on the importance of health promotion and early treatment. It is important to use techniques such as motivational interviewing to address drug use (which can exacerbate attentional problems), and cognitive-behavioral therapies to address suspiciousness, altered perceptions, and mood dysregulation. An emphasis on sleep hygiene, healthy diet, and regular exercise is also important at all stages of psychosis. In our vignette, Aaron’s history is significant for multiple adverse childhood experiences, which are known to increase stress, inflammation, risk for mental illness, drug abuse, and lifelong health problems. In such cases, it is important to emphasize the importance of psychotherapy (individual, group, and/or family) and behavioral techniques such as mindfulness stress reduction, yoga, or exercise to target the effect of life stressors.
Aaron has a family history of both schizophrenia and bipolar disorder. In these circumstances, the family and the young person may already be concerned about whether the symptoms represent an emerging psychosis. It is important to acknowledge their concerns and to emphasize the importance of lifestyle, stress reduction, and support. Aaron also had a documented history of major depression, hypomanic episodes, and emergence of a mixed mood state with the addition of an antidepressant. Psychoeducation regarding mood disorders, depression versus bipolar spectrum, and the possible induction of rapid cycling or mixed mood states with antidepressant medications should be emphasized. Discussion of pharmaceutical interventions to target acute symptoms such as paranoia, anxiety, sleep disturbance, depression/suicidality, and mania/hypomania should also be discussed in the initial phase of treatment. Finally, an emergency plan should be in place for each family. They need to know whom to call and how to proceed if symptoms worsen.
Broad-Spectrum Interventions
Several controlled clinical trials in patients at clinical high risk have addressed the issue of whether symptoms, functioning, and the rate and timing of conversion can be influenced by potential course-altering therapy (23, 24). Studies have been conducted with cognitive-behavioral therapy (CBT), integrated cognitive-psychosocial therapy (25–27), omega-3 polyunsaturated fatty acids (28), antipsychotics (29, 30), and combinations of these interventions (31).
Cognitive-behavioral, psychosocial, and family-based therapies.
CBT has been shown to reduce symptoms, reduce transition to psychosis, and improve functioning in youths at clinical high risk across multiple centers and has the strongest evidence base of any treatment in individuals at clinical high risk (25–27). There is also a strong evidence base for the effectiveness of CBT for mood and anxiety disorders as well as schizophrenia. CBT and psychosocial therapy moderate negative, emotional, and social symptoms in individuals at clinical high risk. The positive overall outcomes with CBT and integrated psychosocial therapy support their first-line use in patients at clinical high risk.
While the aim of CBT for psychosis is to help patients gain insight into their psychotic symptoms, individuals at clinical high risk have insight and consider their thoughts and subsyndromal symptoms as unusual. Thus, the aim of CBT for patients at clinical high risk is to help foster their awareness. Furthermore, there is evidence that those at clinical high risk for psychosis demonstrate high levels of social defeat and negative evaluations of self and others (32), which in turn have an impact on global functioning. One aim of CBT is thus to help these patients correct inaccurate dysfunctional thoughts that interfere with goal-directed activities (e.g., “My friends are laughing at me and will do me harm, so I’d better stay home”), including defeatist expectancies (e.g., “It will be boring”), low self-efficacy beliefs (e.g., “I always fail”), and unusual beliefs (e.g., “My girlfriend’s phone ringing means she is cheating on me”). The goal of early intervention is to strengthen the focus on using corrective feedback from successful social interactions to challenge social disinterest and defeatist performance beliefs. An attempt should be made to challenge attenuated psychotic symptoms and also help to destigmatize the experience of attenuated psychotic symptoms.
CBT can be augmented with social skills training through activity scheduling. This may be especially important for individuals with negative symptoms. The objective of activity scheduling is to help the patient combat procrastination and gradually re-engage in daily activities and routines. At the same time, social skills training provides an opportunity to practice communications and other social skills in a safe and supportive environment, in which defeatist performance and cognitive beliefs can be challenged during observed social interactions (33).
Given the often significant functional difficulties in individuals meeting clinical high risk criteria, it is also important to introduce supported education or employment and case management. Ongoing family psychoeducation and therapy can help the family in dealing with the challenge of a transitional-age youth individuating and yet needing family support at this critical time. Carer and familial support promote the efficacy of CBT family-focused therapy (34).
Omega-3 fatty acids.
In an initial trial in patients at clinical high risk (28) and in a 7-year follow-up of the same sample (35), Amminger et al. found that omega-3 fatty acids with higher concentrations of eicosapentaenoic acid (EPA) reduced conversion to psychosis, although a subsequent trial (P. McGorry et al., unpublished 2015 data) did not support this finding. The positive outcome in the Amminger et al. study, in which patients at clinical high risk were treated with 700 mg/day of EPA plus 480 mg/day of docosahexaenoic acid (DHA) (28), was maintained for 7 years despite only 3 months of treatment, and tolerance was excellent. Functional outcome, together with both positive and negative symptoms, were improved in treated individuals. Interestingly, patients with borderline personality disorder, major depression, and bipolar disorder also benefit from treatment with omega-3 fatty acids, supporting its use as a broad-spectrum intervention in youths at clinical high risk. Multiple mechanisms of action may be implicated: anti-inflammatory and antioxidant properties; improved membrane fluidity, mitochondrial performance, and synaptic plasticity; inhibition of phospholipase A2; normalization of underactive or overactive mesocortical/mesolimbic dopaminergic pathways; promotion of white matter integrity; and restoration of adequate levels of nervonic acid, a major component of the myelin sheath (36).
Other Pharmacological Treatments
Atypical antipsychotics.
Three clinical trials (Table 2) have investigated the efficacy of atypical antipsychotics in youths at clinical high risk. None of these studies has demonstrated a benefit in terms of reducing conversion to psychosis, and significant side effects, such as weight gain and metabolic changes, have been reported. The lack of clear preventive effects of antipsychotics has led the European Psychiatric Association and its member National Societies (43) to recommend that antipsychotics not be used as first-line treatment until the clear emergence of psychosis and a probable diagnosis of schizophrenia.
TABLE 2. Antipsychotic Trials in Individuals at Clinical High Riska
Risperidone plus CBT, placebo plus CBT, and placebo plus supportive therapy (N=115, double-blind)
No difference in psychotic conversion rate (10.7%, 9.6%, and 21.8%) but improvement in symptoms and functioning
a
CBT=cognitive-behavioral therapy.
Mood stabilizers and antidepressants.
Individuals who meet the clinical high risk criteria have high rates of mood and anxiety disorders prior to the onset of subsyndromal psychotic symptoms and may also benefit from mood stabilizers or antidepressants in conjunction with psychosocial treatments, although no randomized controlled trials have been conducted with these agents in youths at clinical high risk. While these interventions may target presenting symptoms in help-seeking individuals, it is possible that they also provide disease-modifying benefits. Animal models have demonstrated increased neurogenesis, dendritic arborization, and synaptogenesis with selective serotonin reuptake inhibitors (37), supporting the notion that these agents may provide an element of neuroprotection. Preclinical and clinical studies have shown that lithium may exert neurotrophic effects that counteract pathological processes, suggesting protective and potentially regenerative brain effects, in patients with bipolar disorder (38). Well-powered clinical trials are clearly needed in youths at clinical high risk to determine the efficacy of these agents in an early phase of illness and to determine whether there are particular subgroups who are more likely to benefit.
Future Directions In Treatment
A long duration of untreated psychosis is associated with poor treatment response (39, 40), suggesting that earlier intervention may improve the outcome of the illness. Ultimately, the goal of treatment in individuals at clinical high risk for psychosis is to improve symptoms, modify active neuropathological changes, and promote functional recovery. With a greater understanding of aberrant neural systems in early psychosis, it will be possible to better specify treatment. A number of psychosocial and pharmacological interventions have great potential as neuroprotective, disease-modifying, or procognitive interventions in early psychosis. Given the heterogeneity of the prodromal period, the importance of treatment “precision” is evident. Ideally, with the use of risk-factor and biomarker assessments, it will be possible to develop a neurobiological profile to predict treatment response. In line with the Research Domain Criteria (41) proposed by the National Institute of Mental Health, it may be optimal to focus on neural systems to target treatment as opposed to DSM diagnosis.
Psychosocial and cognitive remediation techniques have emerged as some of the most effective interventions to target neurocognition, functional capacity, and functional outcome in schizophrenia. Cognitive remediation offers the potential to reinforce healthy circuits to compensate for areas of cognitive deficits and perhaps reduce gray matter loss and improve brain connectivity at the same time (42). Ongoing clinical trials in youths at clinical high risk will help to determine the efficacy of cognitive remediation in this vulnerable population.
Clinical and functional outcomes are important in clinical trials, but ongoing work that develops biomarkers linked to functional outcome, treatment response, and neural circuitry as surrogate endpoints is an innovative direction. Most importantly, if reliable neurobiological measures can be developed for the clinical setting that help to specify treatments for a particular patient, it would be possible to truly individualize care based on brain function, risk factors, and prediction of response.
Summary and Conclusions
Psychiatry, like the rest of medicine, has begun to focus on the early stages of illness as an opportunity to identify high-risk individuals early in the disease process, intervene, and perhaps prevent some of the devastating consequences of mental illness. In the vignette presented here, Aaron was identified as an individual at high risk for a psychotic illness. He had multiple risk factors, subsyndromal psychotic symptoms, and evidence of mood instability. It was clear that he needed intervention at the initial evaluation. Although he was help seeking and willing to be seen in psychotherapy, he had little family or social support to ensure that he had regular follow-up with mental health professionals. Ideally, he would have participated not only in CBT but also in group therapy and family psychoeducation. Perhaps with additional support and education, he would have agreed to try psychotropic medication to target his mood instability and, if necessary, his emerging psychotic symptoms before he required hospitalization. With a more stable living arrangement, avoidance of substances of abuse, and a stable mood, it is possible that his symptoms would not have progressed to full psychosis.
The case also illustrates the importance of mental health infrastructure for transitional-age youths. Transitioning from adolescence to adulthood, secondary school to work or college, and from a foster care environment to the relatively few resources available after foster care represents a window of opportunity for intervention at a population level. Models for youth mental health that make services accessible, friendly, and nonstigmatizing are an important direction in public health. Had there been more of a safety net in his environment, Aaron might have been able to follow through with treatment more effectively. Given the prospect of future innovative treatment that is precise and preemptive, it will only be effective if individuals in need have access to care.
References
1.
Addington J, Cornblatt BA, Cadenhead KS, et al: At clinical high risk for psychosis: outcome for nonconverters. Am J Psychiatry 2011; 168:800–805
Bora E, Lin A, Wood SJ, et al: Cognitive deficits in youth with familial and clinical high risk to psychosis: a systematic review and meta-analysis. Acta Psychiatr Scand 2014; 130:1–15
Addington J, Stowkowy J, Cadenhead KS, et al: Early traumatic experiences in those at clinical high risk for psychosis. Early Interv Psychiatry 2013; 7:300–305
Cannon TD, Cadenhead K, Cornblatt B, et al: Prediction of psychosis in youth at high clinical risk: a multisite longitudinal study in North America. Arch Gen Psychiatry 2008; 65:28–37
Walker EF, Trotman HD, Pearce BD, et al: Cortisol levels and risk for psychosis: initial findings from the North American Prodrome Longitudinal Study. Biol Psychiatry 2013; 74:410–417
Perkins DO, Jeffries CD, Addington J, et al: Towards a psychosis risk blood diagnostic for persons experiencing high-risk symptoms: preliminary results from the NAPLS project. Schizophr Bull 2015; 41:419–428
Cannon TD, Chung Y, He G, et al: Progressive reduction in cortical thickness as psychosis develops: a multisite longitudinal neuroimaging study of youth at elevated clinical risk. Biol Psychiatry 2015; 77:147–157
Anticevic A, Haut K, Murray JD, et al: Association of thalamic dysconnectivity and conversion to psychosis in youth and young adults at elevated clinical risk. JAMA Psychiatry 2015; 72:882–891
de la Fuente-Sandoval C, León-Ortiz P, Azcárraga M, et al: Striatal glutamate and the conversion to psychosis: a prospective 1H-MRS imaging study. Int J Neuropsychopharmacol 2013; 16:471–475
Bodatsch M, Brockhaus-Dumke A, Klosterkötter J, et al: Forecasting psychosis by event-related potentials: systematic review and specific meta-analysis. Biol Psychiatry 2015; 77:951–958
Van Craenenbroeck K, De Bosscher K, Vanden Berghe W, et al: Role of glucocorticoids in dopamine-related neuropsychiatric disorders. Mol Cell Endocrinol 2005; 245:10–22
Meyer U, Weiner I, McAlonan GM, et al: The neuropathological contribution of prenatal inflammation to schizophrenia. Expert Rev Neurother 2011; 11:29–32
Frank MG, Baratta MV, Sprunger DB, et al: Microglia serve as a neuroimmune substrate for stress-induced potentiation of CNS pro-inflammatory cytokine responses. Brain Behav Immun 2007; 21:47–59
Lanté F, Meunier J, Guiramand J, et al: Neurodevelopmental damage after prenatal infection: role of oxidative stress in the fetal brain. Free Radic Biol Med 2007; 42:1231–1245
Pantelis C, Velakoulis D, McGorry PD, et al: Neuroanatomical abnormalities before and after onset of psychosis: a cross-sectional and longitudinal MRI comparison. Lancet 2003; 361:281–288
Keshavan MS, Anderson S, Pettegrew JW: Is schizophrenia due to excessive synaptic pruning in the prefrontal cortex? The Feinberg hypothesis revisited. J Psychiatr Res 1994; 28:239–265
Moghaddam B, Javitt D: From revolution to evolution: the glutamate hypothesis of schizophrenia and its implication for treatment. Neuropsychopharmacology 2012; 37:4–15
Fusar-Poli P, Bonoldi I, Yung AR, et al: Predicting psychosis: meta-analysis of transition outcomes in individuals at high clinical risk. Arch Gen Psychiatry 2012; 69:220–229
Larson MK, Walker EF, Compton MT: Early signs, diagnosis, and therapeutics of the prodromal phase of schizophrenia and related psychotic disorders. Expert Rev Neurother 2010; 10:1347–1359
Addington J, Epstein I, Liu L, et al: A randomized controlled trial of cognitive behavioral therapy for individuals at clinical high risk of psychosis. Schizophr Res 2011; 125:54–61
Bechdolf A, Wagner M, Ruhrmann S, et al: Preventing progression to first-episode psychosis in early initial prodromal states. Br J Psychiatry 2012; 200:22–29
Morrison AP, French P, Stewart SL, et al: Early detection and intervention evaluation for people at risk of psychosis: multisite randomised controlled trial. BMJ 2012; 344:e2233
McGlashan TH, Zipursky RB, Perkins D, et al: Randomized, double-blind trial of olanzapine versus placebo in patients prodromally symptomatic for psychosis. Am J Psychiatry 2006; 163:790–799
McGorry PD, Yung AR, Phillips LJ, et al: Randomized controlled trial of interventions designed to reduce the risk of progression to first-episode psychosis in a clinical sample with subthreshold symptoms. Arch Gen Psychiatry 2002; 59:921–928
McGorry PD, Nelson B, Phillips LJ, et al: Randomized controlled trial of interventions for young people at ultra-high risk of psychosis: twelve-month outcome. J Clin Psychiatry 2013; 74:349–356
Stowkowy J, Addington J: Maladaptive schemas as a mediator between social defeat and positive symptoms in young people at clinical high risk for psychosis. Early Interv Psychiatry 2012; 6:87–90
Miklowitz DJ, O’Brien MP, Schlosser DA, et al: Family-focused treatment for adolescents and young adults at high risk for psychosis: results of a randomized trial. J Am Acad Child Adolesc Psychiatry 2014; 53:848–858
Amminger GP, Schäfer MR, Schlögelhofer M, et al: Longer-term outcome in the prevention of psychotic disorders by the Vienna omega-3 study. Nat Commun 2015; 6:7934
Manji HK, Moore GJ, Chen G: Clinical and preclinical evidence for the neurotrophic effects of mood stabilizers: implications for the pathophysiology and treatment of manic-depressive illness. Biol Psychiatry 2000; 48:740–754
Melle I, Larsen TK, Haahr U, et al: Reducing the duration of untreated first-episode psychosis: effects on clinical presentation. Arch Gen Psychiatry 2004; 61:143–150
Insel T, Cuthbert B, Garvey M, et al: Research Domain Criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry 2010; 167:748–751
Schmidt SJ, Schultze-Lutter F, Schimmelmann BG, et al: EPA guidance on the early intervention in clinical high risk states of psychoses. Eur Psychiatry 2015; 30:388–404
National Institute of Mental Health10.13039/100000025: MH102374, MH081944, MH105243, MH105247
Brain and Behavior Research Foundation10.13039/100000874: Young Investigator Award (HM)
Drs. Cadenhead and Mirzakhanian are supported by NIMH grants MH102374, MH081944, MH105243, and MH105247. Dr. Mirzakhanian is also supported by a NARSAD Young Investigator Award.The authors report no financial relationships with commercial interests.
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.