Living in poverty exposes families to chronic stressors that can increase family instability and conflict, compromising effective parenting as well as limiting access to high-quality early care and education (
1). Children growing up in these adverse circumstances often exhibit deficits in social-emotional competencies and language skills when they enter formal schooling (
2). These initial gaps in school readiness do not diminish over time, but forecast ever-widening disparities in school adjustment, behavioral risks, and emotional distress, with elevated rates of psychopathology apparent by adolescence (
2,
3). Enriching preschools serving low-income families with evidence-based social-emotional learning (SEL) programs and enhanced support for language development may foster resilience by improving child self-regulation skills and promoting child capacities to initiate and sustain positive interpersonal relationships (
4).
The negative impact of poverty-related adversities on mental health begins in early childhood and affects later adjustment in multiple ways. Early experiences play a particularly important role in shaping neurodevelopmental reactivity to stress and capacity for effective emotional and behavioral regulation (
5). Exposure to chronic or unpredictable negative circumstances and unreliable interpersonal support can overwhelm immature stress response systems, increasing impulsive responding and impeding the development of the prefrontal cortex and associated executive functions that support self-regulation and problem-solving skills (
6). In addition, stressed and under-resourced living conditions can increase parental irritability and family conflict and diminish the early socialization supports that foster growth in child emotional understanding and empathy, interpersonal trust, communication skills, and behavioral control (
1).
Underdeveloped social-emotional and self-regulation skills leave children unprepared for the behavioral demands of school (
2). In a bidirectional negative cascade, contextual adversity increases emotional reactivity and decreases adaptive interpersonal and coping skills, which in turn expose children to more adversity in the form of distressing social experiences at school (
1) and coercive, conflictual transactions at home (
7). As a result, almost 20% of children growing up in poverty show clinically significant rates of conduct problems at school entry (
2,
8).
By adolescence, growing up in poverty adds to the convergence of factors that exacerbate externalizing and internalizing psychopathology (
7,
9). Likely as a result of both past and current adversity in family, school, and community settings, adolescents from low-income families often show heightened emotional reactivity and elevated rates of antisocial behavior and emotional symptoms, compared with their more advantaged peers (
9,
10).
Longitudinal studies suggest that stronger social-emotional and self-regulation skills developed early in life serve as protective factors for low-income youths, enabling them to more effectively manage their feelings and inhibit impulsive behaviors as they navigate the social opportunities and stressors of adolescence (
9,
11,
12). Landmark preschool studies initiated over 50 years ago, such as the Perry Preschool and Abecedarian programs, first demonstrated that high-quality preschool (relative to home care) could promote improved well-being in adulthood (
2). Recent reanalyses suggest that growth in social-emotional and self-regulation skills rather than academic skills account for the long-term benefits these programs produced (
13,
14).
Leveraging these findings, more recent studies have enriched classrooms with SEL programming to enhance growth in early social-emotional skills and documented positive short-term effects on child skills and school adjustment (
15,
16). A recent meta-analysis of 31 studies demonstrated that, on average, preschool SEL programs significantly reduce child externalizing problems with effects of small to moderate magnitude (effect sizes, 0.26–0.50, representing between one-quarter and one-half standard deviation difference between intervention and control group children) (
4).
However, long-term follow-up studies are rarely conducted to determine the sustained benefits of such SEL programming. One recent meta-analysis of 82 SEL programs implemented in grades K–12 found small sustained effects on improved SEL skills (effect size=0.17) and reduced emotional distress (effect size=0.12); only six of these studies followed children more than 4 years (
17). Only one preschool SEL program has tracked study participants into high school. Ten years after receiving the Chicago School Readiness Project intervention—in which teachers were trained in positive behavior management strategies—youths reported significant improvements in their grades (effect size=0.19) and demonstrated improvements on an executive function task (effect size=0.18, nonsignificant at p=0.08) (
18). No sustained benefits were found on internalizing or externalizing problems.
The present study fills an important gap in the literature by examining the adolescent outcomes produced by the Head Start REDI (Research-Based, Developmentally Informed) program, which enriched preschool classrooms with social-emotional and language-literacy programming. REDI classroom teachers delivered an SEL curriculum that targeted emotional understanding, prosocial skills, intentional self-control, and social problem-solving skills (
19). In addition, based on research demonstrating that oral language skills enhance emotion regulation (
20) and reduce externalizing problems (
21), REDI also included a daily interactive reading program that used SEL-themed books to intensify child opportunities to consider and discuss social-emotional competencies and strengthen oral language skills (
23).
In a randomized controlled trial, REDI produced significant posttest gains at the end of preschool in targeted social-emotional competencies, learning engagement, and reduced aggression (d values, 0.21–0.35) along with enhanced vocabulary (d=0.15), compared with usual-practice Head Start (
23). Significant benefits remained evident through the end of elementary school in areas of enhanced social adjustment, learning engagement, and parent involvement (d values, 0.24–0.34), although effects on behavior problems had diminished by grade 5 (d=0.12) (
24).
In the present study, we tested the hypothesis that providing the REDI enrichments in preschool could promote improvement 8–10 years later at the transition from middle to secondary school, producing reduced levels of psychopathology symptoms in adolescence.
Methods
The study was conducted in compliance with the ethical standards of the American Psychological Association and with the approval of the institutional review board at Pennsylvania State University. All parents and teachers involved in the study provided signed informed consent for participation, and youths provided assent.
Participants
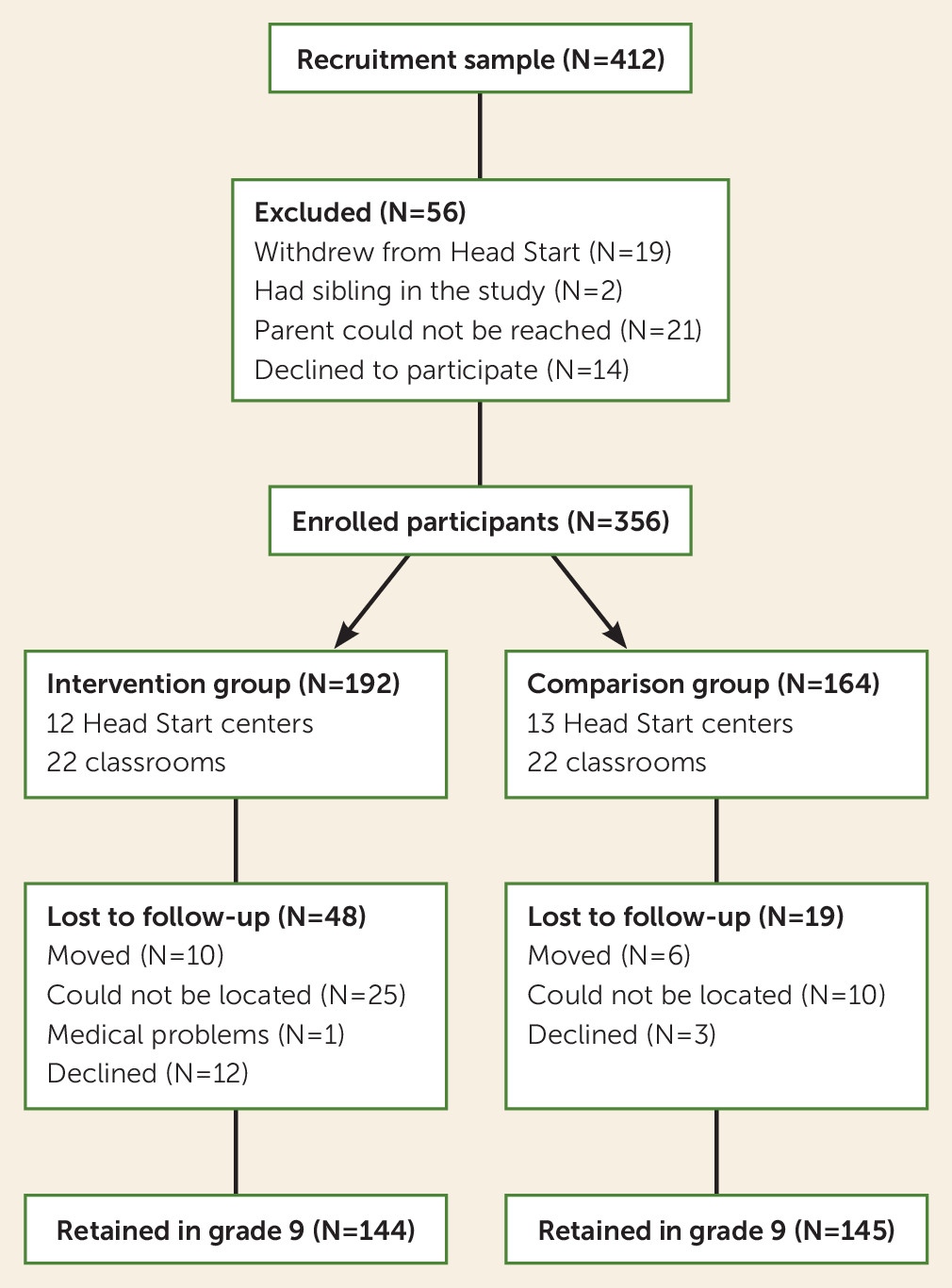
Participants were 356 children (58% White, 25% Black, 17% Latino; 54% female) recruited from Head Start programs serving three counties in Pennsylvania. Participating families were low income (median annual income, $15,000; average income-to-needs ratio, 0.88; 40% single-parent). Most parents had limited education (less than high school, 31%; high school, 60%; some post–high school education, 7%; and 4-year college degree, 2%).
Procedure
In 2003 and 2004, 25 Head Start centers were stratified by county, program features (e.g., full-day versus half-day), and population demographic characteristics (e.g., percent of children of color) and randomly assigned to the intervention (Head Start with REDI enrichments) or a control condition (usual-practice Head Start). Parents of all 4-year-old children in those centers were invited to participate in a study evaluating the impact of Head Start on child development, and 86% consented. Children with parental consent were assessed at the start and end of the preschool year and subsequently were followed longitudinally as they left Head Start and dispersed into 202 different kindergarten classrooms in 82 elementary schools in 33 school districts. By grade 9, the children had spread out further into 73 different high schools in 53 districts.
Attrition occurred at a rate of about 2% per year, mostly as a result of family moves, with 81% of the sample retained through grade 9 (
Figure 1). Retained and missing families were equivalent on most baseline characteristics; however, retention was significantly higher in the control group than the intervention group (88% compared with 78%) and among White non-Latino children than Latino children (87% compared with 72%) (see Table S1 in the
online supplement).
Head Start REDI Intervention
The REDI intervention used the Preschool PATHS (Promoting Alternative Thinking Strategies) curriculum (
19) to promote social skills, emotional understanding, self-regulation, and social problem solving. Teachers delivered 33 lessons, introducing skill concepts with stories, puppets, and discussions. Teachers also led extension activities (e.g., role play, games, art projects) to provide opportunities for guided skill practice. PATHS was integrated with a daily interactive reading program in which teachers utilized scripted questions to encourage child participation and promote advanced thinking and language skills (
22). The books were coordinated with the PATHS social-emotional themes, providing children with an “extra dose” of exposure to SEL concepts. Teachers also led sound games to develop phonological awareness and used alphabet centers to promote letter knowledge. To further promote skill use, teachers were encouraged to use supportive teaching strategies (e.g., positive classroom management, emotion coaching, induction strategies to promote self-control, and problem-solving dialogue) and enrich classroom language use (e.g., ask open-ended questions to extend conversations). Families were provided with weekly letters and three modeling videotapes to help them reinforce program themes at home.
The full Head Start REDI program was manualized. Teachers participated in 4 days of workshop training and received weekly mentoring from REDI trainers to support high-fidelity implementation. Teachers reported completing most of the planned PATHS and interactive reading lessons (mean=86%). On average, REDI trainers rated classroom implementation quality as “adequate” to “strong” (
23).
Measures
Teachers rated adolescent adjustment when participants were in grade 7 (middle school, ages 12–13) and grade 9 (high school, ages 14–15). Teachers provided independent ratings and were naive concerning the participants’ preschool intervention status.
Teachers completed the Strengths and Difficulties Questionnaire (SDQ) (
25), which has been used extensively and shows strong associations with clinical diagnoses of DSM-IV disorders (
26). SDQ subscales of five items each included conduct problems (e.g., fights, lies, or cheats; Cronbach’s alpha, 0.80 and 0.84 for grades 7 and 9 respectively), emotional symptoms (e.g., worried, unhappy, depressed; Cronbach’s alpha, 0.75 and 0.78), hyperactivity-inattention (e.g., restless, easily distracted, poor concentration; Cronbach’s alpha, 0.86 and 0.84), and peer problems (e.g., solitary, picked on or bullied by others; Cronbach’s alpha, 0.64 and 0.68). The clinical significance of the SDQ was interpreted by using the recommended four-category cutoffs for each scale, reflecting scores as follows: 1=close to average, 2=slightly raised, 3=high, and 4=very high (
27).
A set of covariates assessed at baseline was included to increase statistical power and the precision of estimates of intervention effects. Covariates included study design features (e.g., cohort, county site), demographic characteristics (e.g., child sex, ethnicity/race), vocabulary, baseline observer ratings of child self-regulation, and a cumulative measure of adverse childhood experiences (e.g., abuse history, parent separation, maternal depression, family mobility, parent need for special education, family use of corporal punishment). The covariates also included parent-rated measures of preschool behavior that corresponded to the SDQ outcomes. Covariate measures are described in more detail in Table S2 in the online supplement, and baseline scores for the intervention and control groups are provided in Table S3 in the online supplement.
Statistical Analysis
All analyses were conducted with 40 imputed data sets using a multiple imputation model that implemented fully conditional specification methods and included all outcomes and covariates (PROC MI in SAS, version 9.4). Three-level hierarchical linear models (
27) with random intercepts were estimated to evaluate intervention effects on SDQ scores. Level 1 included the effect of time from grade 7 to grade 9, centered at grade 9. Because the effects of time and the time-by-intervention status interactions were not significant for any outcome, these effects are not reported. Level 2 included the fixed effects of intervention status and the study covariates. Level 3 included the random effect of Head Start classroom. Effect sizes for each outcome were calculated by dividing the difference in adjusted means for children in the intervention and control conditions by the pooled standard deviation of the outcome across condition and grade. Such effect sizes are comparable to a Cohen’s d, adjusted for model covariates (
28).
To evaluate intervention effects on clinically significant levels of psychopathology symptoms, two a priori hypotheses were tested in grade 7 and again in grade 9. One logistic regression equation compared the intervention and control groups on SDQ scores that were “close to average” and those that were elevated (i.e., “slightly raised,” “high,” or “very high”). Another logistic regression equation compared the intervention and control groups on SDQ scores that were “very high” and those that were not clinically significant (i.e., “high,” “slightly raised,” or “close to average”).
Results
Preliminary Analyses
Baseline data revealed successful randomization with no significant differences between the intervention and control groups on any measure used in this study. School-level data revealed equivalence in the quality of schools subsequently attended by intervention and control group children based on rates of student poverty and academic achievement (see Table S3 in the online supplement).
Sample means and standard deviations, along with correlations among outcome measures, are presented in
Table 1. Within-grade correlations (r) among scales were 0.24–0.58 in grade 7 and 0.29–0.61 in grade 9, with the highest correlation in each grade between conduct problems and hyperactivity. Two-year stability correlations from grade 7 to grade 9 ranged from a low of 0.26 for emotional symptoms to a high of 0.51 for hyperactivity.
Evaluation of Intervention Effects
As presented in
Table 2, hierarchical linear model analyses of the SDQ continuous scores revealed a statistically significant intervention effect on conduct problems (β=−0.44, p=0.04, 95% CI=−0.90, −0.01; d=−0.20). The analyses also revealed a statistically significant intervention effect on emotional symptoms (β=−0.53, p=0.01, 95% CI=−0.92, −0.13; d=−0.25) (see Table S4 in the
online supplement).
Assessment of Clinical Significance
Logistic regression equation estimates at grade 7 revealed no statistically significant differences between the intervention and control groups in clinically significant levels of problems on any subscale of the SDQ (see Table S5 in the
online supplement). In contrast, as presented in
Table 3, logistic regression equation estimates at grade 9 revealed that significantly more youths from the REDI intervention group, compared with the usual-practice Head Start control group, displayed normative (e.g., “close to average”) as opposed to any level of elevated score on conduct problems (β=0.76, p=0.03, 95% CI=0.09, 1.44; odds ratio=2.15) and emotional symptoms (β=0.75, p=0.04, 95% CI=0.03, 1.47; odds ratio=2.12). Likewise, logistic regression equation estimates at grade 9 revealed that significantly fewer youths from the intervention group than the control group displayed clinically significant (e.g., “very high”) as opposed to any lower level score on conduct problems (β=−1.43, p=0.004, 95% CI=−2.40, −0.46; odds ratio=0.24), emotional symptoms (β=−1.90, p=0.003, 95% CI=−3.15, −0.66; odds ratio=0.15), and peer problems (β=−1.96, p=0.02, 95% CI=−3.58, −0.34; odds ratio=0.14).
Discussion
Growing up in poverty increases risk for exposure to chronic stressors and adverse experiences (
1,
5). Adverse early experiences and ongoing stress exposure leave many socioeconomically disadvantaged youths without the levels of impulse control, emotion regulation, and social supports they need to effectively navigate the social and behavioral demands of school and the challenges of adolescence, contributing to elevated levels of adolescent conduct problems and emotional distress (
12). This study documents the preventive benefits of enriching preschool programs, like Head Start, with evidence-based SEL interventions, which reduced rates of clinically significant adolescent conduct problems, emotional symptoms, and peer problems compared with usual-practice Head Start. In terms of clinical significance, these reductions by grade 9 were notable, with rates of very high conduct problems and emotional symptoms each reduced by 11 percentage points (6% and 3%, respectively, in the intervention group, compared with 17% and 15% in the control group) and rates of very high peer problems reduced by 6 percentage points (2% in the intervention group, compared with 8% in the control group.)
Extensive research documents the short-term benefits of contemporary preschool programs that utilize evidence-based curricula and provide professional development support for teachers, promoting gains in child academic and social-emotional skills at school entry (
29). However, only a few studies have examined the sustained effects of these programs in elementary school, and the findings are often disappointing, with academic benefits often fading fairly quickly (
29,
30). Researchers have suggested that the quality of subsequent instruction may undermine the academic advantages of children who experience enriched preschool (
30).
There are good reasons to believe that the benefits in the “noncognitive” domains of social-emotional well-being and mental health may be less influenced by subsequent academic instruction and hence more enduring (
13,
14). However, the Chicago School Readiness Project, which has followed children into high school, found that initial effects on internalizing and externalizing problems were not sustained (
18). Among the preschool programs of the past 50 years with a focus on social-emotional skills, REDI has demonstrated some of the longest-lasting effects.
Several factors may have increased REDI’s long-term impact on adolescent mental health. Like many SEL-focused preschool programs, including the Chicago School Readiness Project, REDI promoted more positive classroom management practices (
31). In addition, REDI provided children with explicit instruction in social-emotional skills during weekly PATHS lessons and extension activities. This developmentally sequenced SEL curriculum may have increased growth in children’s social-cognitive skills and provided classroom routines that helped teachers encourage daily conversations about feelings and regular use of social problem-solving dialogue (
4). REDI also used daily interactive reading sessions to promote growth in child oral language skills using books with social-emotional themes that provided a “double dose” of exposure to social-emotional themes and concepts. REDI enhanced the quality of teacher’s language use in the classroom (
31) and included additional intervention components to promote child emergent literacy skills, such as sound games and an alphabet center. It seems likely that REDI support for child language development in combination with the SEL programming contributed to the longer-term benefits of the program.
Conceptually, promoting social-emotional and language skills in preschool may support children in critical ways as they enter elementary school, altering the negative trajectories associated with skill deficits at school entry. The short-term benefits are that children who can connect in positive ways with teachers and peers and who are engaged adaptively in classroom activities are more likely to experience success (
15,
16). In the longer term, enhanced social-emotional competencies and self-regulatory skills may reduce adolescent susceptibility to emotional distress, deviant peer influences, and impulsive decision making, reducing the initiation or escalation of conduct problems and associated risky behaviors (
10,
32). In this way, preschool programs like REDI that foster emotional understanding, emotion regulation, language skills, and behavioral self-control may serve as protective factors reducing the negative developmental cascades after school entry that contribute to later increases in externalizing and internalizing symptoms (
10).
The present findings suggest that important public health benefits could be obtained by leveraging current public investments in preschool programs and enriching these programs with evidence-based curricula and teaching strategies that support SEL and language skill development. Public costs for Head Start are about $10,000 per student per year (
33); enriching classrooms with REDI costs an additional $831 per student (
34). This is a relatively small incremental cost, given the evidence of the reductions in costly adolescent conduct problems, emotional symptoms, and peer problems documented here.
The major limitation of this study was the use of SDQ teacher ratings as the only measure of adolescent psychopathology. Previous research suggests that, compared with self or parent ratings on the SDQ, teacher ratings are more accurate predictors of clinically diagnosed externalizing disorders, but that self ratings improve the sensitivity of teacher ratings in identifying internalizing disorders (
25). The precision of teacher ratings was likely increased in the present study by inclusion of ratings by different teachers in grades 7 and 9. Nonetheless, teachers rely on their observations and may be unaware of the internal feelings or covert delinquent acts of adolescents. In addition, the SDQ is a brief screening measure and not a diagnostic instrument. The inclusion of additional methods of measurement would have strengthened the study.
Conclusions
Enriching preschools with evidence-based programming that supports SEL and language skill development may be an important way to reduce the disparities in school readiness and mental health associated with growing up in poverty. Preschool SEL programs may address the origins of disparities in mental health early in life and thus reduce negative developmental cascades that can amplify pathology. As such, preschool SEL programs may be more effective at reducing rates of psychopathology than relying on treating symptoms after they emerge in adolescence (
5). SEL and language skill enrichment in preschool may be highly strategic for public health if early intervention can foster resilience and reduce additional exposure to adversity, thereby improving educational attainment, social support, and well-being, while reducing vulnerability to adolescent risky behavior and psychopathology.
Additional follow-up research is needed to determine whether these preschool enhancements will support significant improvements in life accomplishments such as high school graduation, employment status, and adult mental health. Additional research is also needed to determine how these effects might be amplified by coordinating preschool programs with parent-focused enrichment (
35,
36) or by embedding this kind of universal preschool program within a multitiered system of supports that offers additional, more intensive support services to children or parents who require them (
37).
Acknowledgments
The authors thank their partners in this project: the parents, students, teachers, and program personnel of the Head Start programs of Huntingdon, Blair, and York counties in Pennsylvania and the many school districts that supported follow-up assessments.