1. Introduction
Between 14% and 23% of pregnant women will experience a depressive disorder while pregnant (
1). In 2003, approximately 13% of women took an antidepressant at some point in pregnancy, a rate that has doubled since 1999 (
2). Thus, clinicians and patients need up-to-date information to assist with decisions about depression treatment during pregnancy. To meet this need, the American Psychiatric Association and the American College of Obstetricians and Gynecologists convened a work group to critically evaluate and summarize information about the risks associated with depression and antidepressant treatment during pregnancy. The group was comprised of clinical research experts within these two medical specialties and a developmental pediatrician. By consensus, the authors selected studies that were methodologically sound as evidenced by clearly stated variables and sample sizes that were appropriate to test stated hypotheses. This report is published jointly in a psychiatric and an obstetrical journal to ensure that clinicians have easy access to the information.
Readers should consider several limitations when interpreting the literature. Only a minority of reports that assessed associations between antidepressant treatment and birth outcomes included information on maternal psychiatric illness. When available, such information was typically in the form of clinicians' reports from administrative databases or self-report screening measures. The studies with detailed information regarding diagnoses and antidepressant use were usually smaller and had limited power to find important associations. Finally, confounding factors that influence birth outcomes, such as poor prenatal care and drug, alcohol and nicotine use were variably controlled. These potential confounders occur at a higher rate in depressed compared to nondepressed women (
3) Similarly, pregnancy complications such as nausea, vomiting, hyperemesis gravidarum, and pre-eclampsia occur at a higher rate in depressed compared to non-depressed women (
4).
The convergence of results from studies with different designs was a factor used in this report to evaluate the validity of associations between antidepressant exposures and adverse reproductive outcomes. We review findings that refer to associations between maternal depression and use of antidepressants with regard to specific perinatal outcomes. At the end of the report, we present strategies for the management of women with depression who are either pregnant or planning a pregnancy.
6. Treating a pregnant woman who is depressed
6.1. Behavioral treatments for mood disorders
Many patients with mild-to-moderate depression can be treated by psychosocial approaches including individual and group psychotherapy in lieu of medication. Patients with residual symptoms, those at high risk of relapse, those with comorbid conditions such as panic disorder and those who prefer to avoid medication may benefit from psychotherapy. This is an especially critical option for women preparing for conception or currently pregnant since a large percentage of women may plan to avoid medication.
Cognitive behavioral therapy (CBT) or interpersonal psychotherapy (IPT) have been shown to be effective for depression in pregnant women (
57). Web and computer-based cognitive behavioral therapy are options if there are few behavioral therapists in a patient's area or she has monetary limitations. While evidence for supportive and psychodynamic psychotherapy is limited, these approaches are also reasonable if IPT and CBT are unavailable.
6.2. Antidepressant treatment during pregnancy
There are no antidepressant drug efficacy trials in depressed pregnant women. However, there is little reason to think that response would differ between pregnant and nonpregnant women. Guidelines for treatment of depression and mania in pregnancy have been published (
58–
60).
It is ideal, but not always possible, to evaluate a woman with a past or current depressive illness prior to conception. In 2001, more than 6 million women conceived in the United States and nearly half of these were unintended (
61). Accordingly, this document presents algorithms for the management of a depressed woman who is contemplating pregnancy and is taking antidepressant medication (
Fig. 1), pregnant and not receiving treatment for depression (
Fig. 2) and pregnant but already undergoing pharmacological treatment for depression (
Fig. 3). For all, healthy lifestyles, such as nutritional adequacy and weight management, regular prenatal care and childbirth education should be emphasized and supported. Treatment of addictions such as cigarettes, alcohol and other exposures is appropriate to reduce maternal-fetal risk.
Before prescribing any medication, document all drug and environmental exposures dating back to conception in the record. Careful documentation of a risk benefit discussion regarding medication or other treatment is imperative (
59).
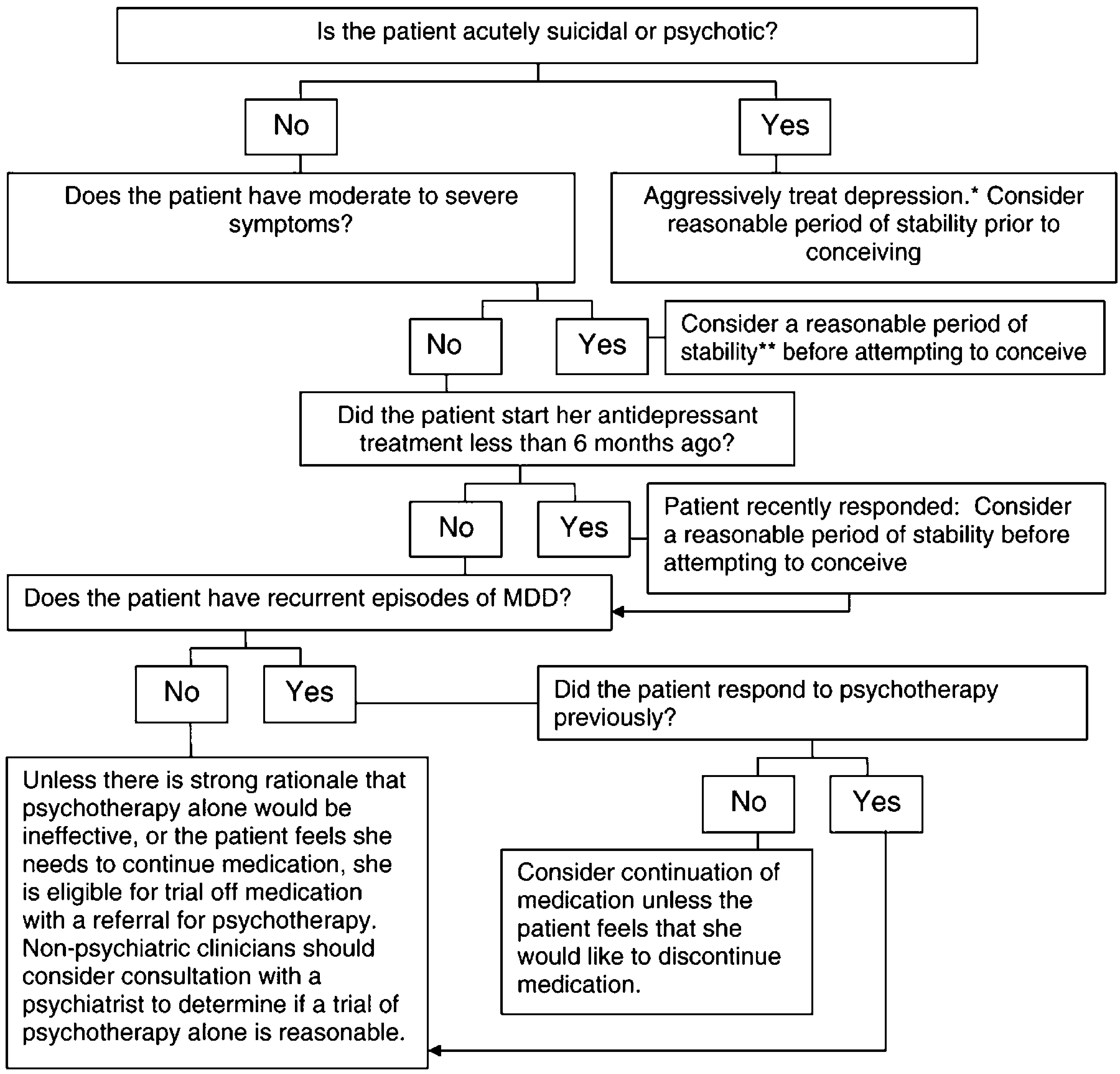
6.3. Pre-conceptional patients
When depressed patients present prior to conception for evaluation, her provider should determine whether the patient has moderate to severe symptoms (see algorithm in
Fig. 1). If the evaluation is conducted by an obstetrical provider and the patient has suicidal or acute psychotic symptoms, she should be promptly referred to a psychiatrist for aggressive treatment. In such instances, it is judicious for the patient to wait a period of time after she has achieved euthymia before she attempts to conceive. Whether the patient has an evaluation with an obstetrician or a psychiatrist, if she has moderate to severe symptoms, her clinician should strongly consider continuation and optimization of her antidepressant medication. It is prudent to counsel the patient to wait for a period of time prior to conceiving in this instance as well. While it is difficult to specify an exact or optimal length of time for all patients, guidelines such as those from the Agency for Healthcare Quality and Research, suggest that antidepressant treatment for a first, acute episode of depression should endure at least 6–12 months (
62).
Patients with mild or no symptoms for 6 months or longer may be candidates for medication taper and discontinuation prior to conception. The patient's psychiatrist and obstetrician can collaborate with the patient to make the decision regarding a hiatus from pharmacotherapy. Generally, if a woman is a candidate for stopping pharmacological treatment, slow taper such as 25% reduction in dose every 1–2 weeks with close monitoring for relapse or discontinuation symptoms is preferable.
Patients with a history of severe, recurrent major depressive disorders (MDD), psychosis, bipolar illness, psychiatric comorbidity that requires pharmacotherapy, or history of a serious suicide attempt may not be candidates for medication discontinuation. These individuals should continue psychotropic medication and her obstetrician and psychiatrist, if available, should coordinate her care so that she has optimal prophylaxis from psychiatric illness relapse but also appropriate obstetrical care. Some women may also benefit from referral to a therapist who can provide psychotherapy. While CBT or IPT are preferable, other types of counseling may be helpful if empiric-based therapies are not available.
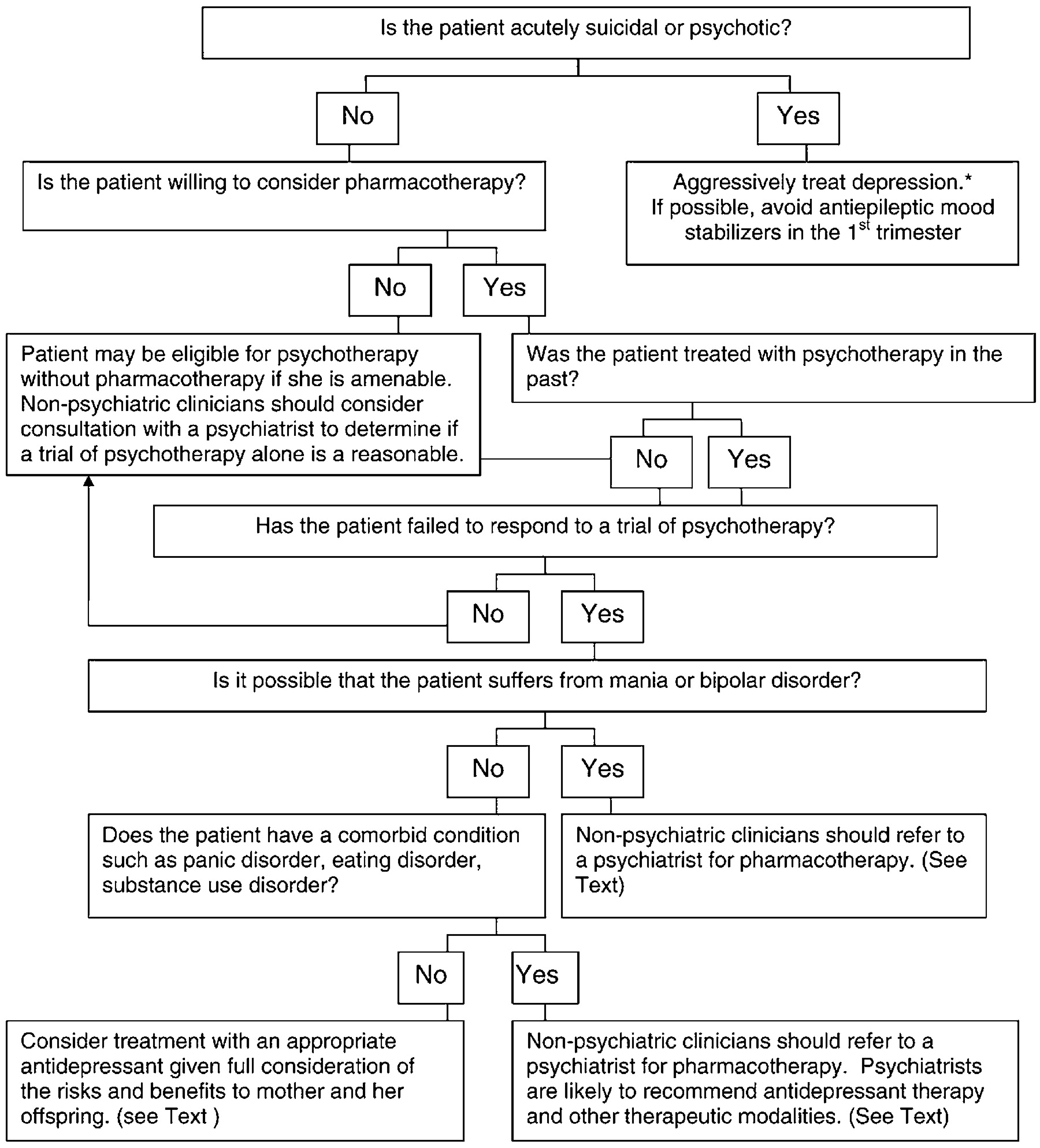
6.4. Pregnant patient who is not receiving pharmacotherapy
It is common to diagnose untreated depression during pregnancy and to encounter patients who have discontinued their medications but are symptomatic. The algorithm presented in
Fig. 2 summarizes recommendations for management of a depressed woman who is pregnant but not receiving treatment for her illness. Again, if an obstetrical provider encounters a patient with suicidal or psychotic symptoms, a psychiatrist who can optimize her pharmacotherapy should see the patient emergently. If possible, the psychiatrist should avoid first trimester use of antiepileptic agents, newer antipsychotic agents and antidepressants. The former are teratogens and are appropriate if alternatives are ineffective; there is less reproductive safety information about new (atypical) antipsychotics and antidepressants than agents that have been on the market for a decade or longer. An additional step is to assess whether the patient would consider pharmacotherapy. If a woman prefers not to take antidepressant medication and she is not gravely disabled or at high risk of relapse, she may benefit from psychotherapy. Psychiatrists should manage women who suffer from bipolar affective disorder since monotherapy with an antidepressant may trigger mania and psychosis. If the patient lives in a rural or other area where a psychiatrist is not available, the obstetrical provider may decide to seek expert consultation with regard to the management of the patient.
The treatment choice for other patients will depend upon the safety profile of the medications, the stage of gestation, the patient's symptoms, history and therapeutic preferences. The dose of agents metabolized primarily by cytochrome P 450 2D6 or P450 3A4 may require an increase in the second half of pregnancy (
63). If a patient has an agitated depression, a more sedating antidepressant such as a TCA may be preferable. Mirtazepine is also sedating but there are few data on its use in pregnancy. TCAs and some SSRIs will also augment a patient's appetite if she has difficulty gaining weight. Women who are depressed and smoke cigarettes may benefit from treatment with bupropion, although a history of seizures or bulimia would preclude use of this agent.
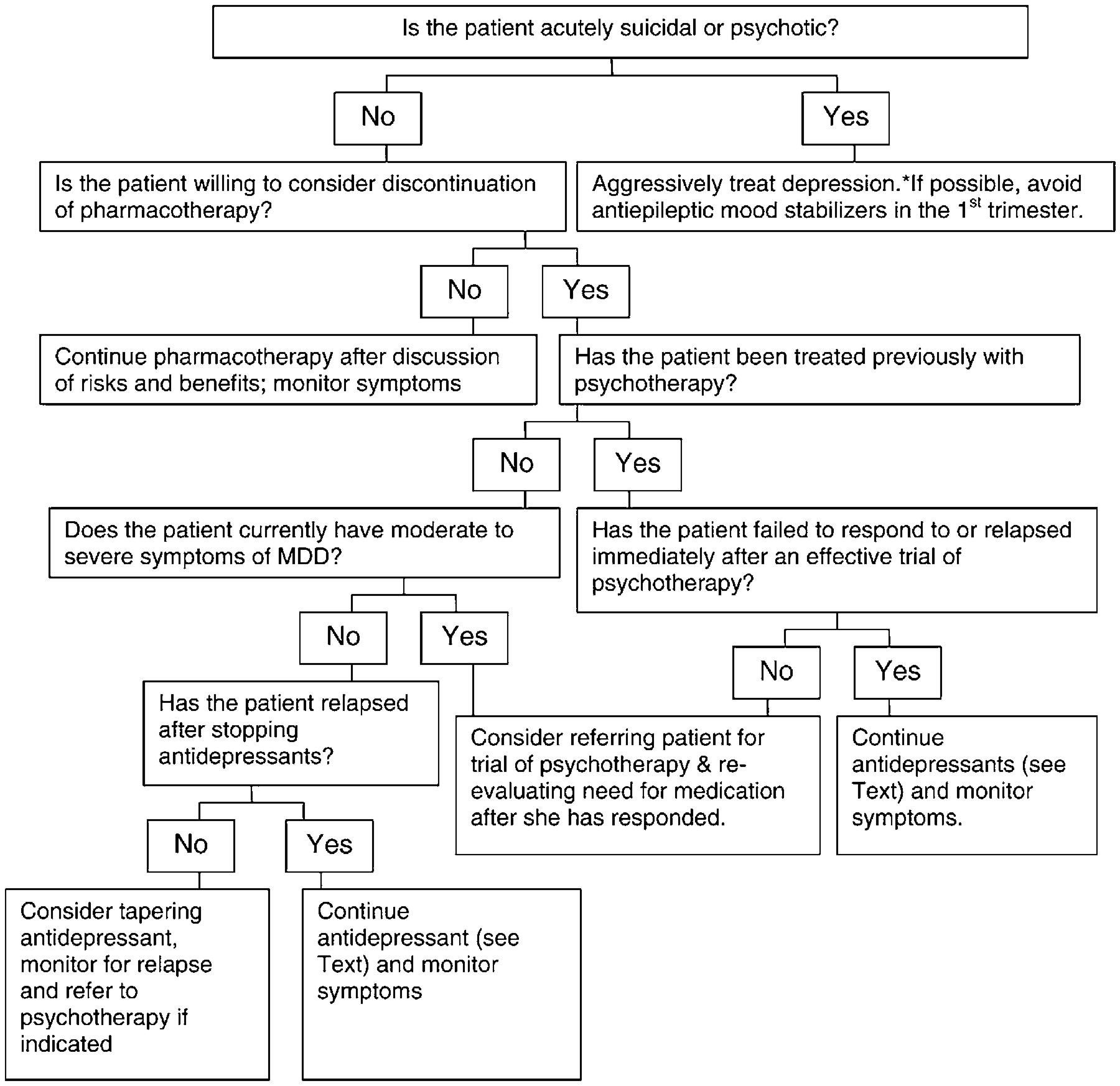
6.5. Patient with current or recent MDD who is taking antidepressants in pregnancy
A woman may seek assistance about whether to continue or taper her antidepressant medication. An algorithm to address this issue is illustrated in
Fig. 3. As above, a woman with evidence of current suicidal or psychotic thoughts will need to be managed aggressively by her psychiatrist. If the patient is psychiatrically stable and prefers continuation of medication, the psychiatric and obstetrical clinician should discuss risk/benefit issues and document this discussion and the patient's choice, in her medical record. Respect for the patient's preferences is paramount since she will likely have a sense of her ability to manage a pregnancy off medication. If the patient is willing to consider discontinuation of medication and she is not currently having symptoms, then, depending upon the individual's psychiatric history, a trial of medication taper may be appropriate. Women who have a history of severe, recurrent depression, even if currently asymptomatic or minimally symptomatic, are at high risk of relapse if medication is discontinued. In one prospective cohort study of women who suffered from recurrent depression, the risk of relapse was sixfold higher if women elected to discontinue antidepressant treatment in pregnancy compared to women who continued treatment at the same dose throughout pregnancy (
64).
Patients who have recurrent MDD or are symptomatic despite ongoing medication may benefit from psychotherapy that may either augment or replace pharmacotherapy. Patients who have not responded adequately to solo antidepressant treatment with a solid trial of psychotherapy, have severe illness with abrupt relapse after medication discontinuation or have a concurrent psychiatric condition that requires medication management, are candidates for continued antidepressant treatment.
Patients who are asymptomatic, have had a period of stability on treatment or have responded well in the past to psychotherapy may be candidates for medication taper and discontinuation with additional psychotherapy as needed. Their clinicians should monitor them for signs and symptoms of relapse.
7. Frequently Asked Questions
(1) Should women who are being treated with paroxetine prior to conception switch to an alternative SSRI?
The decision to continue or change medication is a collaborative one between the physician and the patient, and there is no universal “best answer” for all women. The data that would link paroxetine use during the first trimester with cardiac malformations are not strong but it prompted the US Food and Drug Administration to reclassify the agent as a category “D” drug. Nonetheless, some mothers may be concerned about media reports. If paroxetine is the only antidepressant that she has tried, substitution may be reasonable; however, substitution always carries the risk of relapse. If she has responded to paroxetine only after several other failed drug trials, substitution becomes difficult to justify. The clinician should review data regarding paroxetine as outlined in the preceding sections, document the discussion and the woman's questions carefully in the medical record.
(2) Given the recently reported six-fold relative risk for persistent pulmonary hypertension of the newborn associated with SSRI exposures after 20 weeks gestation, how should pregnant women receiving SSRI therapy be counseled?
The six-fold risk is a relative risk; the absolute risk increases from 1 to 2 per 1000 (0.1–0.2%) to 3–12 per 1000 (0.3–1.2%) with exposure to SSRI (
44,
49). The risk for PPHN was increased for exposures to SSRI after 20 weeks of gestation and did not occur for non-SSRI antidepressants (
44). However, the risk of PPHN could be related to the duration of antidepressant use or other maternal illness severity characteristics (
33). Factors of illness history, risk of relapse with a change of agent and patient preference must be considered here as in Question 1 above.
(3) In view of reports regarding neonatal SSRI effects, how should women who receive SSRI therapy in the third trimester be counseled?
Third trimester use of TCAs and SSRIs have been associated with neonatal signs which are either due to the presence of antidepressants in the infant at birth (akin to side effects) or discontinuation effects. The majority of infants have signs that are mild and transient (most have disappeared by two weeks). Clinicians should consider preparing mothers for the possibility of infant effects such as restlessness and irritability. Such behaviors are not limited to SSRI exposed infants but are found in neonates exposed to TCAs as well as non-psychotropic exposure, including nicotine, as well as neonates with no exposures. Discontinuing medication to avoid symptoms in the neonate may lead to relapse in the mother.
(4) What are the absolute contraindications to stopping SSRI therapy in pregnancy?
Women with severe depression characterized by suicide attempts, functional incapacitation or weight loss should be continued on their medication. The risk of recurrence or escalating symptoms is high after treatment discontinuation and can result in deterioration of the woman's physical health and possibly suicide. In the event that a patient refuses pharmacologic treatment, it is imperative for a psychiatrist to be part of the treatment team to reinstitute treatment if clinical deterioration occurs. Ideally, a plan for alternative treatment and monitoring of the patient's well being should be developed before medication discontinuation.
(5) Are there pregnant patients for whom a TCA or bupropion would be a superior therapeutic option?
The antidepressant bupropion is also a therapy for nicotine addiction and may have added benefit for women who smoke and are depressed. However, not all patients respond to buproprion and clinicians should recognize that a change of medication may lead to relapse. This medication is contra-indicated for individuals who have an eating disorder or seizure disorder. Tricyclic antidepressants are reasonable for use during pregnancy and an advantage is the ability of the clinician to monitor serum levels alongside response. However, anticholinergic side effects (e.g., dry mouth, constipation and sedation) and toxicity in overdose are disadvantages. As with bupropion, a patient who has responded to an SSRI may not respond to a TCA if she is switched to this medication.
(6) Which pregnant patients are candidates for electroconvulsive therapy?
Patients who have not responded to antidepressant therapy or who are psychotic, suicidal or severely disabled are candidates for electroconvulsive therapy. Other patients with severe depression may prefer electroconvulsive therapy because of the rapidity of response to this modality.