Posterior cortical atrophy (PCA) is the progressive and disproportionate loss of visual functions associated with neurodegeneration of posterior cortical regions.
1,2 Recent consensus criteria for PCA emphasize visuospatial and visuoperceptual deficits, relative sparing of memory and other cognitive functions, and posterior cortical abnormalities on neuroimaging.
2 The most common cause of PCA is an early-onset visual variant of Alzheimer’s disease.
3 Although there is no specific treatment for PCA or clear symptom response to Alzheimer’s medications, psychostimulants such as methylphenidate could potentially aid in improved shifting spatial attention and, hence, overall functioning among patients.
4 Additionally, methylphenidate might improve the ability of patients with PCA to overcome lack of motivation and withdrawal consequential to visuospatial limitations. Here, case reports of three patients with PCA whose symptoms improved with methylphenidate treatment are presented.
Patient 1
A 56-year-old woman presented with 2 years of progressive visual localization difficulty, particularly affecting her ability to dress herself and to drive. On dressing, she could not pick out her clothes or put her arms through the sleeves. On driving, she could not stay in her lane, appropriately stop at stop signs, or park her car. Her Mini-Mental State Examination (MMSE) score was 21/30.
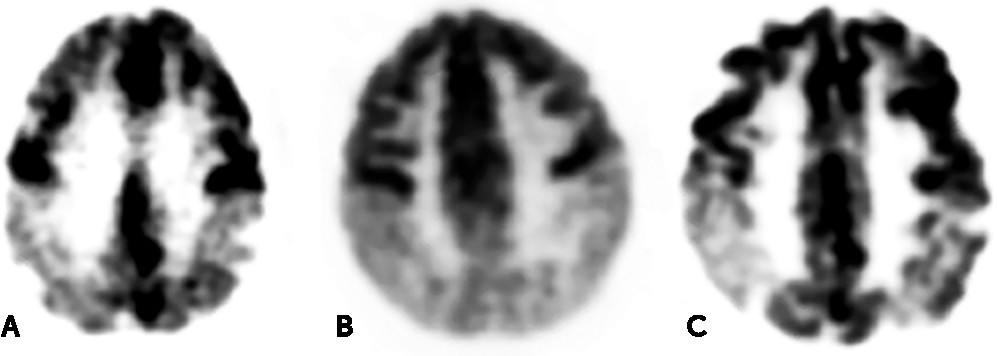
5 She demonstrated normal language and memory but marked abnormalities on drawings and tasks involving overlapping or Gestalt figures, visual search, and letter location. Her neurological examination was otherwise normal. MRI results suggested that the patient had PCA, evident as parietal and posterior temporal hypometabolism on fluorodeoxyglucose positron emission tomography (FDG-PET) (
Figure 1A). CSF biomarkers for Alzheimer’s disease (β42 amyloid, total tau, and phosph-tau) confirmed a diagnosis of PCA due to Alzheimer’s,
6 and the patient was treated with donepezil (10 mg/daily) and memantine extended release (28 mg/daily). She also received varying doses of escitalopram for mood and anxiety.
At the 2-year follow-up, the patient became poorly motivated beyond any depression or problems with mood. She had continued treatment with donepezil and memantine, without clear treatment response. However, her mood and anxiety had improved with escitalopram. She felt severely limited in activities of daily living due to the visuospatial deficits of Bálint’s syndrome (simultanagnosia, oculomotor apraxia, and optic ataxia), with an inability to even locate food and utensils placed before her. She was started on methylphenidate (5 mg twice/day) and become significantly more active. Although her visuospatial deficits and examination results did not improve, for the first time in several years she began spending significantly more time with her children, exercising, and socializing with friends.
Patient 2
A 57-year-old woman presented with 4 years of progressive visuospatial difficulties, such as localizing nobs and finding words on pages. She demonstrated an inability to use controls or a keyboard, to find a signature block on paperwork, and to read more than two lines on a page before the “words disappear.” Her MMSE score was 13/30. Her language was intact, but her memory was mild to moderately impaired. The main neurological deficits were observed on visuospatial tasks, including drawings and visual search localization. No further deficits were observed on other tasks. MRI results suggested a diagnosis of PCA, and temporoparietal and occipital hypometabolism was found on FDG-PET (
Figure 1B). CSF biomarkers were consistent with Alzheimer’s, and the patient was treated with donepezil (10 mg/day), memantine (10 mg/twice daily), and escitalopram (10 mg/day) for depression with anxiety.
At the 2-year follow-up, the patient’s mood was generally euthymic, but she had become inactive and disengaged, primarily due to Bálint’s syndrome and visuospatial constraints. She had continued treatment with donepezil and memantine, without definite treatment response. However, she was euthymic, with minimal reported anxiety while receiving escitalopram. She was started on methylphenidate (5 mg/twice daily). Although neither her visuospatial deficits nor examination results improved, her family described her as initiating more activities, as well as walking more. Additionally, and to the surprise of her family, she was able to perform more than one task at a time.
Patient 3
A 62-year-old woman presented with 1 year of progressive visuospatial difficulties localizing keypad buttons on telephones and items on desks. She also showed environmental disorientation and was unable to drive. She described difficulty voting due to an inability to locate the circles on the punch ballot. On examination, the patient’s MMSE score was 27/30, her language was intact, and her memory was mildly impaired. However, she could not perform simple drawings, interpret overlapping or crosshatched figures, or localize dots or letters. Her neurological examination was otherwise normal. MRI results were nondiagnostic, but an FDG-PET showed parietal hypometabolism (
Figure 1C). An amyloid PET scan was positive for amyloid neuritic plaques, consistent with PCA due to Alzheimer’s disease.
6 Treatment included donepezil (10 mg/day) and memantine extended release (28 mg/day), as well as several antidepressants for both depression and anxiety.
At the 3-year follow-up, the patient had apathy out of proportion to any other evidence of depression or anxiety and consistent with pronounced and limiting visuospatial difficulties. She had continued treatment with donepezil and memantine with little treatment response. However, the addition of methylphenidate (5 mg b.i.d.) resulted in rapid improvement of her symptoms. She demonstrated increased engagement with her children, such as taking camping trips, and she had started participating in physical activities, such as exercise. Additionally, she had attended a college reunion.
Discussion
Among the three PCA patients above, treatment with low-dose methylphenidate was effective in attenuating some symptoms, without any reported adverse effects. Although their attention and visuospatial deficits were not improved, they became motivated and involved in activities. This observation is important, because there is no effective treatment for PCA, and patients with this disorder frequently withdraw and disengage because they are effectively visually impaired. The lack of motivation and initiation is often disproportionate to the effects on mood, and these symptoms may not respond to antidepressant medications.
Previous studies have reported that patients with Alzheimer’s disease who were treated with methylphenidate showed improved in symptoms.
7–10 Apathy and poor motivation are common in Alzheimer’s disease, including PCA due to Alzheimer’s, and may result from dysfunction in the dopaminergic brain reward system, as well as from perceived inability to function in visual environments. Early research suggested that negative symptoms among patients with dementia, independent of depression, were responsive to methylphenidate treatment.
11 Subsequent randomized, double-blind trials among outpatients with mild-to-moderate Alzheimer’s symptoms who were treated with methylphenidate (20 mg/day) and one open-label study reported improvements on apathy scores with treatment.
7–10 Methylphenidate may be particularly helpful for patients with the PCA variant of Alzheimer’s, who often become poorly motivated to initiate activities due to limiting visuospatial impairments. Moreover, previous and current research suggest that methylphenidate may help to improve attention, depression, and decision-making behavior among patients with dementias.
12This preliminary report, along with previous work, highlights the need for research on the use of methylphenidate, or other psychostimulants, for the PCA variant of Alzheimer’s disease or other forms of visual impairment due to deficits in specific brain regions.