There is increasing recognition that trauma-informed care should be part of all substance abuse treatment programs, given the known rate of trauma and posttraumatic stress disorder (PTSD) among such programs' clientele (
1,
2). According to U.S. population data, among men who experience PTSD in their lifetime, 52% develop an alcohol use disorder and 35% develop a drug use disorder. Among women, 28% and 27%, respectively, develop an alcohol or drug use disorder (
3). In clinical settings, the rates are higher (
4). Moreover, the comorbidity of PTSD and substance use disorder is associated with more significant clinical impairment, including worse treatment outcomes, more axis I and II disorders, increased HIV risk, legal and medical problems, suicidality, and self-harm, compared with either disorder alone (
4–
9).
It is important not only to integrate trauma counseling into treatment but also to make trauma-informed care part of treatment at all levels. Trauma-informed care takes into account the impact of a trauma on all aspects of a client's life. All staff members are trained to understand the impact that trauma may have on a client and how every interaction should focus on reducing the possibility of retraumatization (
1,
2,
10).
It is unknown how successful recent efforts to move toward this integrated approach have actually been. What are the rates of trauma-related counseling in treatment facilities? Are certain types of treatment facilities more likely to engage in trauma counseling? Also, it is unclear in what ways, if any, facilities providing trauma-related counseling might differ from facilities not providing this service. We sought to address these questions by using data from the National Survey of Substance Abuse Treatment Services (NSSATS), an annual survey conducted by the Substance Abuse and Mental Health Services Administration (SAMHSA). This survey of substance abuse treatment facilities is the most extensive national data available on level of service provision. We sought to examine the characteristics of substance abuse treatment facilities that differed in their amount of trauma-related counseling.
Methods
The NSSATS data are collected annually by SAMHSA and are available online (
11). The NSSATS is a national survey of all public and private substance abuse treatment facilities in the United States. We used data from the 2009 NSSATS. Of the 15,213 facilities eligible for the 2009 survey, 14,209 (93.4%) completed the survey. However, 696 facilities were excluded because another facility reported information for them or because they reported client counts that included clients from other facilities. Thus the final sample size was 13,513 facilities (88.8%). The number of respondents for each survey item is available online in the Substance Abuse and Mental Health Data Archive codebook (
11). Most respondents completed the survey via the Internet.
The independent variable for this study was a survey item about types of clinical services currently provided by the facilities. The item lists a variety of clinical and therapeutic approaches, including trauma-related counseling, used by substance abuse treatment facilities. Respondents are asked to mark the box that best describes how often the practice is used. Response options are never, rarely, sometimes, always or often, or not familiar with this approach. For ease of interpretation we recoded responses to the question about trauma-related counseling into two categories: no or low use (combining the responses never, rarely, and not familiar with this approach) and moderate to high use (combining the responses sometimes and always or often).
The dependent variables were 107 of the approximately 205 survey items. The survey included 43 numbered global items and a number of subitems for many of the questions. Items providing very detailed information, often the subitems of a global item, were sometimes omitted, even though the global item was included. For example, we included responses to a question about whether the facility provides substance abuse treatment services in a language other than English at a particular location but excluded responses to the 20 subitems asking about specific languages. We also excluded 45 items related to client count for specific services, such as detoxification, on a given day.
We grouped the outcome variables into two categories: services or counseling provided by the treatment facility and characteristics of the facility. Most responses are yes or no. For items that assessed frequency, the responses of never, rarely, and not familiar were coded as no, and the responses of sometimes and always or often were coded as yes. Given the large number of dependent variables, we used a conservative significance level of .001. This approach reduces the likelihood that significant findings are based solely on capitalization of chance.
We conducted chi square analyses to compare the facilities that provided no or low levels of trauma counseling with those providing moderate or high levels of trauma counseling for all dependent variables.
Results
A total of 290 (2.1%) respondents did not complete the trauma item and were removed from all analyses, leaving a final sample of 13,223 respondents.
The rates of trauma counseling reported by the programs were never, by 11.4% (N=1,535); rarely, by 20.2% (N=2,726); sometimes, by 43.9% (N=5,930); and always or often, by 21.3% (N=2,875). Another 1.2% of facilities (N=157) were not familiar with this approach.
We assessed whether facilities with high or low rates of trauma counseling differed on other variables. The presence of trauma counseling in a treatment facility was significantly related to 92 of the 107 dependent variables examined.
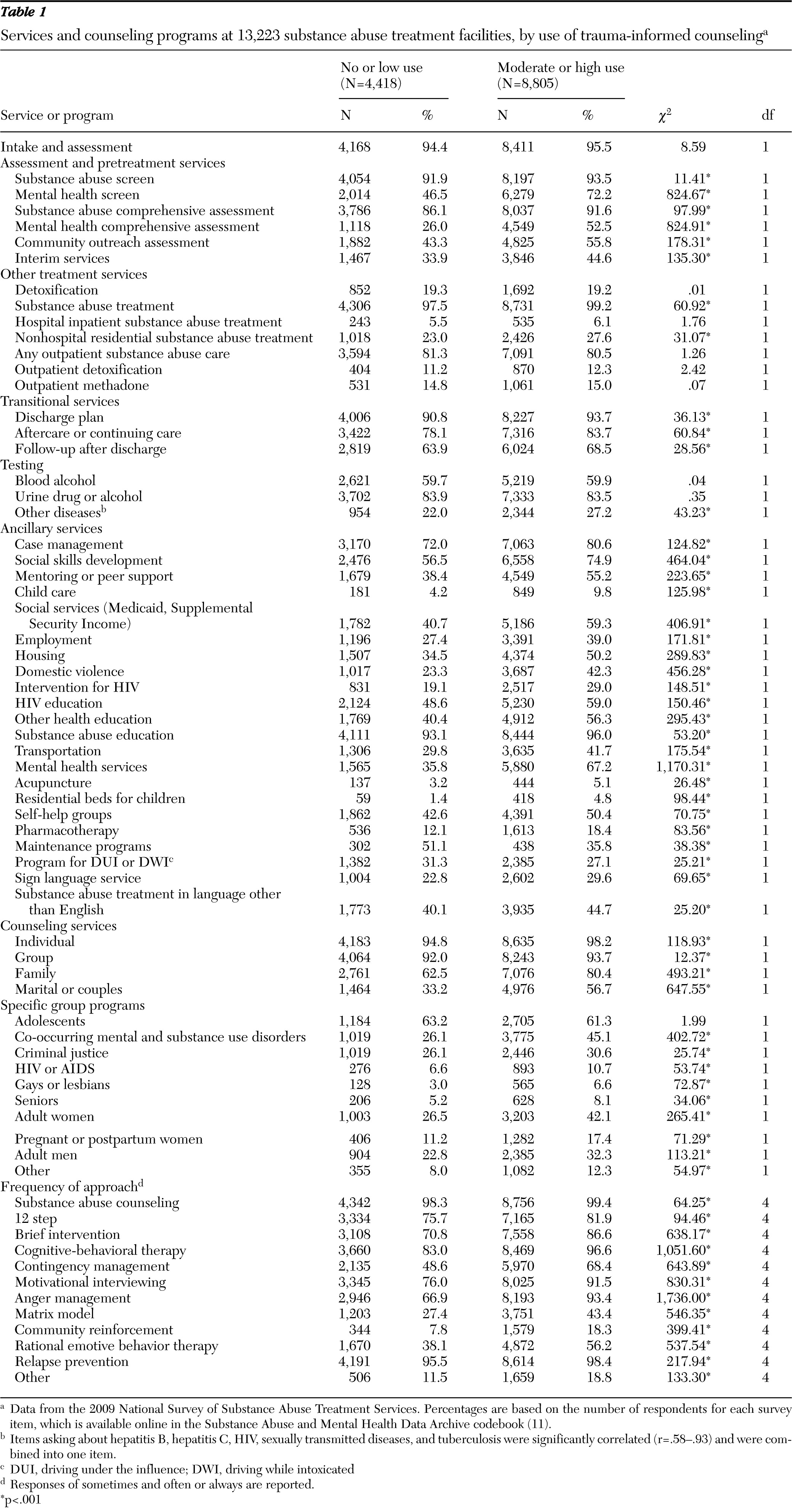
As shown in
Table 1, compared with facilities with no or low levels of trauma counseling, facilities with moderate or high levels of trauma counseling were with few exceptions significantly more likely to engage in a range of services and counseling programs. They were more likely to provide almost all pretreatment, transitional, ancillary, and counseling services as well as nine out of ten therapy groups and all 12 therapy approaches. However, the two groups of facilities did not differ in their reported use of specific treatment options directly related to substance abuse treatment, such as detoxification or methadone therapy.
Characteristics of treatment facilities were also related to trauma counseling. Facility ownership was significantly related to trauma counseling (χ2=71.94, df=5, p<.001) as was the location of the facility (χ2=37.61, df=4, p<.001). Specifically, 1,479 (38.1%) private for-profit agencies reported no or low levels of trauma counseling, making them the least likely of any type of facility to use trauma counseling. The most likely to use trauma counseling were agencies owned by the federal government and nonprofit agencies—no or low levels of trauma counseling were reported by 78 (23.6%) federal government organizations and by 2,448 (31.9%) nonprofit organizations.
Additionally, facilities located in the Northeastern United States or in territories or areas under U.S. jurisdiction were significantly more likely than those in the Midwest, South, or West to use trauma counseling. A total of 1,826 (70.1%) of the agencies in the Northeastern United States and 159 (77.9%) of the agencies in areas under U.S. jurisdiction reported moderate or high levels of trauma counseling compared with 2,004 (64.8%), 2,416 (67.0%), and 2,400 (64.5%) facilities, respectively, in the Midwest, South, or West.
Facilities with moderate or high levels of trauma counseling were significantly more likely to have procedures in place related to increasing supervision and educational services for staff and clients (continuing education for staff, χ2=32.76, df=1, p<.001; case review with supervisor, χ2=41.62, df=1, p<.001; case review by quality review, χ2=134.40, df=1, p<.001; periodic utilization review, χ2=157.49, df=1, p<.001; and client satisfaction surveys, χ2=58.93, df=1, p<.001). The only service that was equally provided by all facilities was periodic drug testing.
Compared with facilities with no or low levels of trauma counseling, facilities with moderate or high levels of trauma counseling were significantly more likely to have established facilitywide accreditations beyond accreditations related only to substance abuse (accreditation by the state health department, χ2=20.64, df=1, p<.001; state mental health department, χ2=233.78, df=1, p<.001; Joint Commission, χ2=41.27, df=1, p<.001; Commission on Accreditation of Rehabilitation Facilities, χ2=11.23, df=1, p<.001; National Committee for Quality Assurance, χ2=10.49, df=1, p<.001; and Council on Accreditation, χ2=16.49, df=1, p<.001). Additionally, compared with facilities with no or low levels of trauma counseling, facilities with moderate or high levels of trauma counseling were significantly more likely to accept a wide range of payment options (treatment at no charge, χ2=46.22, df=1, p<.001; Medicare, χ2=218.11, df=1, p<.001; Medicaid, χ2=179.81, df=1, p<.001; private health insurance, χ2=168.16, df=1, p<.001; military insurance, χ2=257.72, df=1, p<.001; and recovery vouchers, χ2=15.62, df=1, p<.001). No differences were found for cash payment.
Discussion
Research has shown that comorbidity of PTSD and substance use disorder is highly prevalent (
4,
5), making trauma-informed care at substance abuse treatment facilities an important aspect of treatment. We found that a majority of substance abuse treatment facilities (66.6%) reported using trauma-related counseling with clients. This is encouraging given the advantages, including improvements in mental health symptoms (
12), of addressing trauma with substance abuse clients.
We also found that facilities using moderate or high levels of trauma counseling were much more likely to provide clients with a wide range of additional services related to their treatment, including a range of counseling techniques and group programs. Additional ancillary services, such as education, child care, and employment, were aimed at assisting clients in all aspects of their lives. Having access to such services has been shown to improve the clients' chances for successful treatment outcomes (
13,
14).
The fact that a majority of facilities reported trauma counseling is evidence of the strides that have been made to incorporate trauma counseling into substance abuse treatment. However, a significant minority of facilities (33.4%) rarely, if ever, engaged in trauma counseling. Notably, this study indicated that certain types of treatment facilities should be the focus of education efforts to raise awareness. These include facilities located in the South, Midwest, and West and for-profit facilities. Nonprofit facilities may be more likely to engage in trauma counseling than for-profit facilities because they may be more likely to keep abreast of government-sponsored training and initiatives (including the current focus on trauma-informed care), given that typically they are funded through government grants.
The NSSATS provides extensive data about substance abuse treatment facilities within the United States. However, it has a number of limitations. The survey attempts to obtain responses from all known facilities, but it is a voluntary survey and thus nonresponse is a concern. It is unknown whether the 6.6% of facilities that decided not to participate in 2009 varied in meaningful ways from facilities that completed the survey. The survey contained one question related to trauma counseling, and more detailed information was not available. Additionally, outcome data, psychometric validation of the survey, and data regarding the quality of trauma counseling or the model of trauma counseling used were not available. Finally, the survey response format was self-report, so it is possible that facilities inflated their responses regarding using trauma counseling. Also, it was unclear what types of services facilities included in their definition of trauma-related counseling.
Conclusions
Providing trauma counseling was associated with the provision of a number of additional treatment-related services and a greater variety of counseling approaches. Thus facilities with moderate or high levels of trauma counseling had more programs and services in place to improve care provided to clients. However, the testing and treatment options directly related to substance use provided by a facility did not tend to differ on the basis of the level of trauma counseling offered.
Future research providing more detailed information about trauma counseling would be beneficial. One important step is to conduct a study about the content of trauma counseling currently offered by facilities and whether the treatment is informed by evidence.
Acknowledgments and disclosures
The authors report no competing interests.