Attention-deficit hyperactivity disorder (ADHD) is a common childhood disorder that has been estimated to affect 3 to 5 percent of school-age children (
1). Recent studies have shown that ADHD is associated with significant impairment in multiple domains of functioning, including a high frequency of psychiatric comorbidity with disruptive mood and anxiety disorders, poor educational attainment, lower IQ, and low occupational performance (
2,
3,
4,
5,
6,
7). ADHD is also associated with maladaptive interpersonal interactions and low self-esteem (
8,
9,
10,
11,
12).
Although similar findings of comorbidity and dysfunction have been reported in large epidemiological studies of children (
13,
14,
15,
16,
17,
18), some pediatricians have suggested that children with ADHD who receive their diagnosis and are managed in the primary care setting have fewer comorbid psychiatric disorders and milder impairments than those seen in psychiatric clinics (
19,
20,
21). The question of whether such ascertainment bias exists has important clinical, scientific, and public health implications, particularly considering that the majority of children with ADHD are treated by primary care physicians (
20).
Among children with ADHD, the presence of comorbid psychiatric disorders predicts both the persistence of ADHD into adulthood and a more complicated course with poorer outcomes (
3,
7,
22,
23,
24). If pediatric samples of children with ADHD were found to have rates of comorbid psychiatric disorders similar to those seen in psychiatric samples, the implication would be that pediatric patients with ADHD may have an equally high risk of experiencing a complicated course and compromised outcome. To our knowledge, this question has not been adequately examined.
We sought to determine whether comorbidity and other clinical correlates of ADHD would differ among children referred to pediatric and to psychiatric clinics. To this end, we compared rates of comorbidity and degree of dysfunction in a large sample of children with ADHD drawn from pediatric and psychiatric practices. On the basis of current notions in pediatric practice, we predicted that children with ADHD recruited from pediatric practices would have less comorbidity and less dysfunction than those recruited from a child psychiatry clinic.
Methods
Sample
The sample included 522 children and adolescents of both sexes, 6 to 18 years of age, with (N=280) and without (N=242) ADHD. Children were excluded from the study if they had been adopted; if the nuclear family was not available for study; or if they had major sensorimotor handicaps, such as paralysis, deafness, blindness, or psychosis, autism, inadequate command of the English language, or a full-scale IQ below 80. Each of the children with ADHD met
DSM-III-R (
25) criteria for a diagnosis of ADHD at the time of clinical referral, and at the time of recruitment, they all had active symptoms of the disorder. Written informed consent was obtained from each parent for his or her child, and children and adolescents provided written assent to participate. The study was approved by the institutional review board of Massachusetts General Hospital.
Our psychiatric sample was made up of consecutive referrals during the late 1980s and early 1990s to the pediatric psychopharmacology program at a large urban medical center. The children were referred by parents, pediatricians, and schools for psychiatric evaluation. Participants in the pediatric sample were consecutively recruited from several pediatric sites of a large health maintenance organization, including both inner-city and suburban locations, in the greater Boston area. Children who came for routine physical examination to the urban medical center and the pediatric sites of the health maintenance organization were recruited as control subjects for the psychiatric sample and pediatric sample, respectively. A detailed description of the selection process has been published elsewhere (
26,
27,
28).
A three-stage ascertainment procedure was used in the selection of participants. For participants with ADHD, the first stage was the original referral to a psychiatric or a pediatric clinic that resulted in a diagnosis of ADHD. To minimize bias, since the diagnosis of ADHD was made by different clinicians using different clinical standards, a second systematic screening step was included: a telephone questionnaire consisting of the 14 DSM-III-R symptoms was administered to the mother of each child who had a diagnosis of ADHD. In the final step, eligible subjects who consented to participate in the study received a comprehensive assessment battery, including a structured diagnostic interview. Only those who received a diagnosis of ADHD at all three stages were included in the study.
Control subjects were also screened in three stages. First, patients referred for routine physical examination were recruited at each site. Second, the DSM-III-R telephone questionnaire was administered to the children's mothers. Eligible subjects who consented to participate received the same assessment battery as the ADHD sample. Only those for whom no diagnosis of ADHD was made at any of the three stages were included in the study.
Assessments
Participants were assessed with
DSM-III-R structured clinical interviews, which were supplemented, when possible, with questions from the
DSM-IV. In cases in which
DSM-IV information was not collected, proxies for
DSM-IV ADHD subtypes were constructed on the basis of
DSM-III-R symptoms (
1,
25). Psychiatric assessments relied on the Schedule for Affective Disorders and Schizophrenia for School-Age Children, Epidemiologic, version 4 (Kiddie-SADS-E) (
29,
30); for children 12 years old and under, this instrument was completed with the mother, and for children over 12, directly with the youth.
All assessment personnel were blinded to the participants' diagnosis and ascertainment source. Interviews were conducted by raters with undergraduate degrees in psychology who completed an intensive training program. The training program consisted of familiarization with psychiatric nosology and structured interviews, observation of interviews carried out by experienced raters and clinicians, and then supervised execution of interviews. Kappa coefficients of agreement were calculated between raters and board-certified child and adult psychiatrists listening to audio tapes made by the raters. For 173 interviews, the median kappa was .86, and the kappa was .99 for diagnosis of ADHD.
All diagnostic uncertainties were resolved by a committee of board-certified child and adult psychiatrists, chaired by the principal investigator (JB). The committee members were blind to the participant's initial site of diagnosis, ADHD status, and psychological tests. Psychiatric disorders were diagnosed only if the interview criteria were met unequivocally. The summary variable "two or more anxiety disorders" was used to define clinically meaningful anxiety disorders (
31). For children over age 12, data from direct and indirect interviews were combined and considered positive when criteria were endorsed by either parent or child. In addition, a
DSM-III-R Global Assessment of Function (GAF) was made. The GAF score summarizes a child's overall function on a scale ranging from 1, worst, to 90, best; it also gives a rating of a child's current function—that is, over the past month—and worst lifetime function (
25).
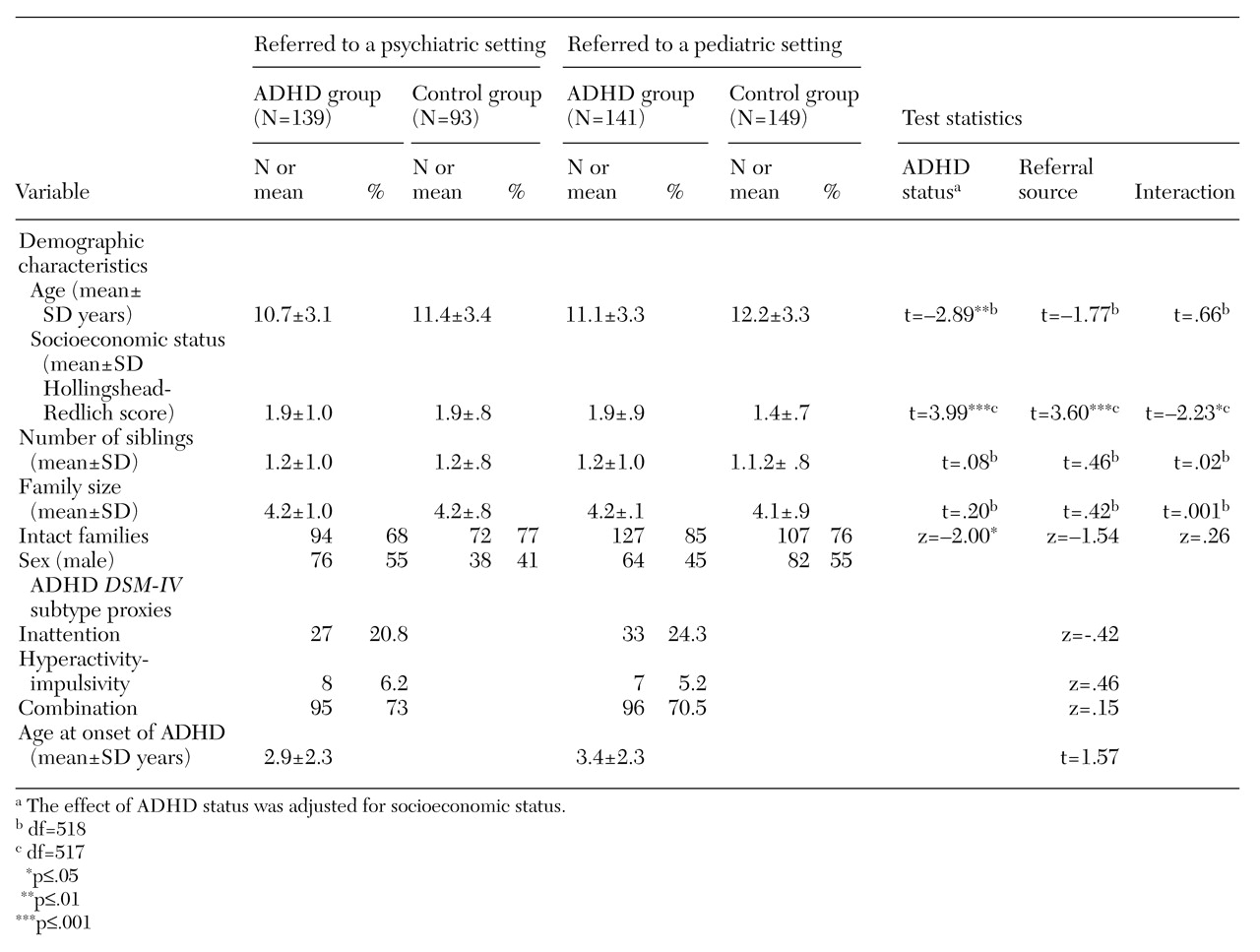
Additional data were collected to assess social and academic functioning. Socioeconomic status (SES) was defined by the Hollingshead-Redlich Scale, which ranges from 1 to 5, with higher numbers corresponding to lower social classes (
32). Family intactness was defined as a binary variable—parents married and the family living together, or parents divorced or separated and the family not living together. Family functioning was measured with the Family Environment Scale (FES) (
33). The FES has high internal and test-retest reliability and availability of norms. It measures the quality of family relationships along three dimensions: cohesion—the degree of commitment, help, and support family members provide for one another, measured on a scale from 1 to 68; expressiveness—the extent to which family members are encouraged to act and express their feelings openly, on a scale of 15 to 73; and conflict—the amount of openly expressed anger, aggression, and conflict among family members, on a scale of 32 to 81.
Social functioning was evaluated with the Social Adjustment Inventory for Children and Adolescents (SAICA) (
34), a semistructured interview schedule that assesses adaptive functioning. It consists of a series of 4-point scales that assess relationships with parents and peers, social activities, and interpersonal problems. Cognitive ability was assessed with the methods described by Sattler (
35); full-scale IQ was estimated from the block design and vocabulary subtests of the Wechsler Intelligence Scale for Children-Revised (WISC-R) (
36). Scores can range from 80 to 133, with higher scores indicating better performance. The Freedom From Distractibility Index, derived from the digit span, arithmetic, and coding subscales of the WISC-R, was also calculated; scores can range from 50 to 150, with higher scores indicating better performance.
We assessed reading and arithmetic achievement with subtests of the Wide Range Achievement Test-Revised (WRAT-R) and the Gilmore Oral Reading Test (
37,
38). Scores on the two tests can range from 46 to 155 and from 60 to 140, respectively, with higher scores indicating better performance. The definition of learning disabilities under Public Law 94-142 requires a significant discrepancy between a child's potential and his or her achievement (
39). We operationalized this definition with the procedure recommended by Reynolds that we have used elsewhere (
40,
41). This procedure yields two binary variables indicating the presence of learning disabilities in reading and in arithmetic.
Statistical analysis
Logistic and linear regression were used to evaluate the influence of a diagnosis of ADHD and the ascertainment source—psychiatric or pediatric—on the outcome variables. Each regression analysis modeled the outcome as a function of three predictors: ascertainment source of diagnosis—psychiatric versus pediatric; ADHD status of the participant—ADHD versus control; and the interaction of ADHD status and ascertainment source, which indicates whether the effects of ADHD status on outcome differ by ascertainment source. This approach provides two types of information about potential ascertainment biases. A significant difference between ascertainment sites would suggest that, regardless of the ADHD diagnosis, there were differences in outcome between sites. A significant interaction would mean that the effect of ADHD status on outcome differed between ascertainment sources.
All analyses were two-tailed, and the alpha level was set at .01 to minimize the risk of type I errors due to multiple statistical tests. For certain diagnostic outcomes, insufficient data prevented the fitting of a standard logistic regression model using maximum-likelihood inference. In these cases, we employed an alternative logistic model that uses conditional exact inference as implemented in LogXact (
42). This method is designed to accommodate situations when the usual assumptions for likelihood ratio and Wald's tests do not hold because the data are insufficient.
Functioning measures
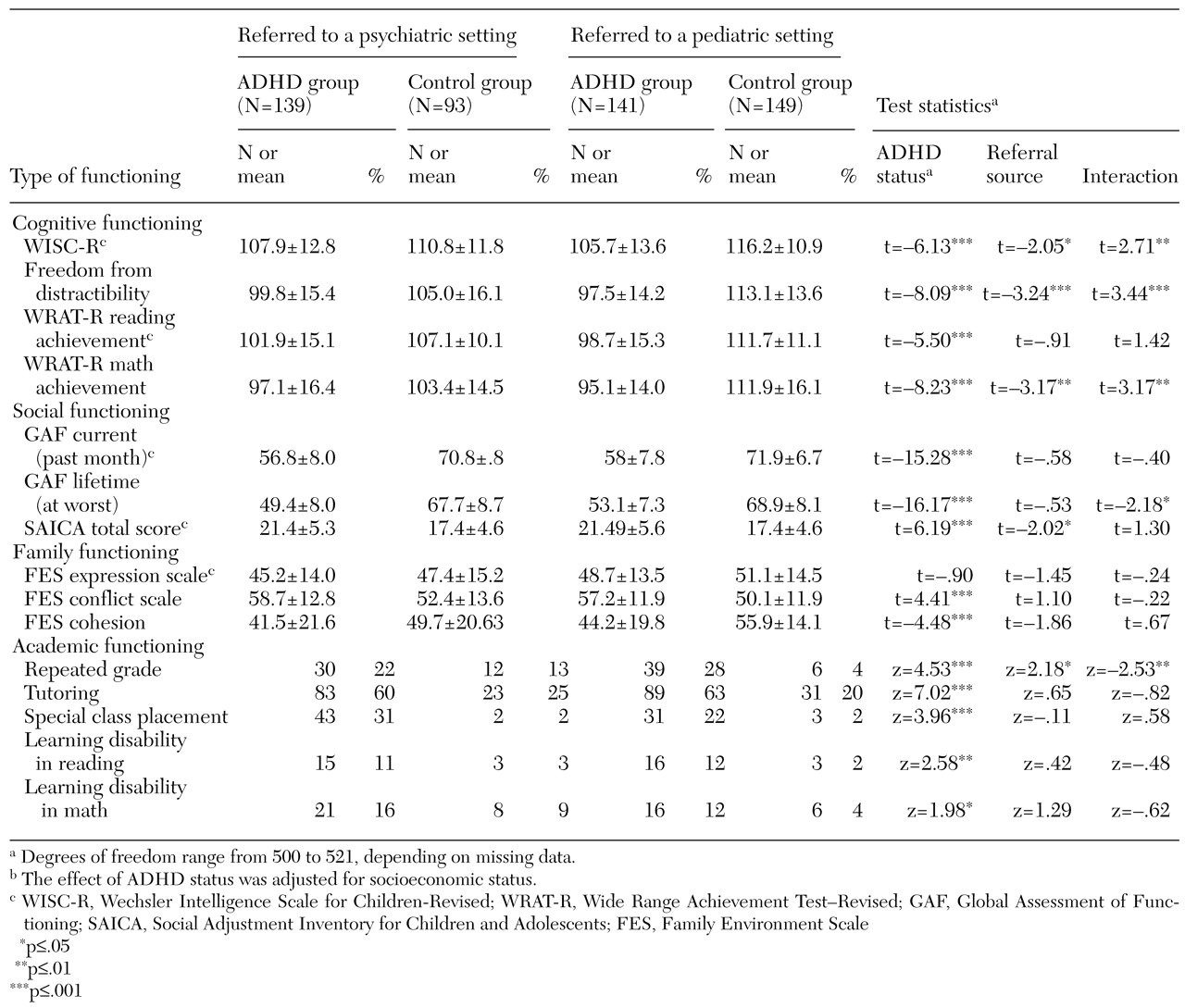
As
Table 4 shows, statistically significant differences were found between children with and without ADHD on measures of intellectual function—full-scale IQ as measured by the WISC-R—and academic achievement—as measured by the reading and math achievement subtests of the WRAT-R. Children with ADHD were more likely than control subjects to have both lifetime and current impairments on the GAF. Children with ADHD were also more likely than control subjects to have significantly less family cohesion and higher levels of family conflict. Children with ADHD and comorbid psychiatric disorders had poorer social functioning overall than children without ADHD. Academic dysfunction was also seen more frequently among children with ADHD, as reflected in higher percentages of tutoring, repeated grades, and special class placement.
We found significant interactions between ADHD status and ascertainment source for full-scale IQ, freedom from distractibility, and the WRAT-R math achievement subtest. The latter two outcomes also showed significant main effects for ascertainment source. Follow-up tests comparing the three outcomes by ascertainment source for children with and without ADHD showed that for those with ADHD, scores for full-scale IQ, freedom from distractibility, and WRAT-R math achievement scores were not significantly different by ascertainment score. However, for children without ADHD, the scores for freedom from distractibility (z=-3.06, p=.002) and WRAT-R math achievement (z=-2.98, p=.003) were significantly lower for children from the psychiatric site.
Discussion
This is the largest case-control study to date of systematically assessed, referred children of both sexes with and without ADHD diagnosed in pediatric and psychiatric practices. Children with ADHD from the two settings had striking similarities in many nonoverlapping domains of functioning, including comorbid psychiatric disorders and measures of interpersonal, cognitive, academic, and family functioning. These similarities are striking, particularly given our comprehensive assessment procedures and methodologically sound sampling strategy (
43) and the adequacy of the statistical power our study had to detect clinically meaningful differences. Despite a higher prevalence of two ADHD symptoms among the children with ADHD from the psychiatric setting, these findings challenge the idea that children with ADHD treated in the primary care setting are less impaired and suggest that studies of children with ADHD from psychiatric settings are not compromised by referral bias.
Despite methodological differences, our findings are highly consistent with results reported for community samples (
12,
13,
14,
15,
16,
17,
44,
45,
46,
47). For example, community samples in Puerto Rico, New Zealand, Canada, and the United States identified patterns of comorbidity among children with ADHD that are consistent with our findings in a referred sample (
12,
13,
14,
15,
16,
17,
44,
45,
48,
49,
50). Recent extensive literature reviews (
46,
47) concluded that co-occurring disorders are common among persons with ADHD. In a study of 8,000 children by Wolraich and colleagues (
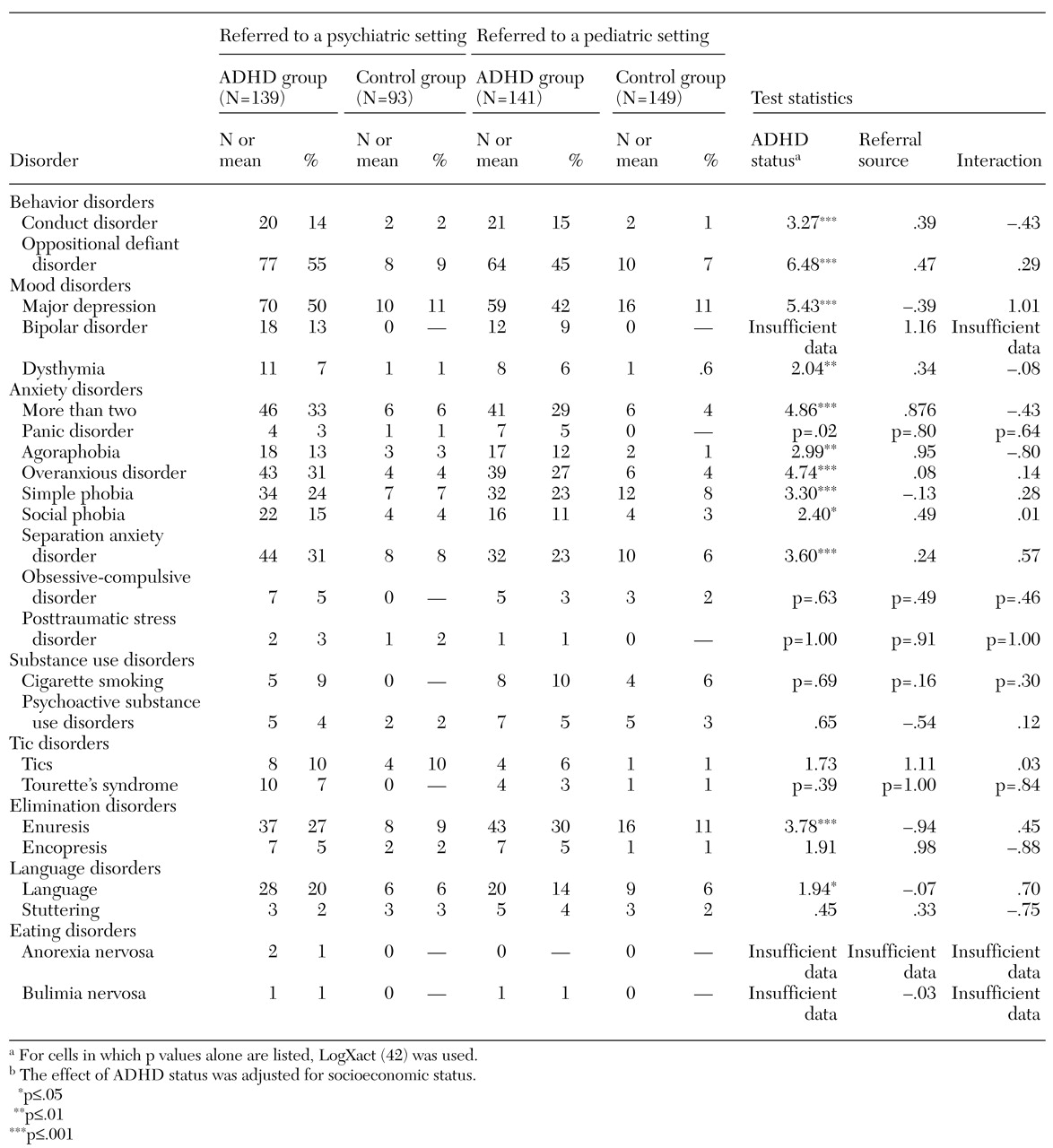
51), 29 percent of children with ADHD had comorbid anxiety or depression, and 29 percent had comorbid conduct disorder. These findings are consistent with those from our pediatric and psychiatric samples.
Wasserman and associates (
21) surveyed pediatric primary care pro-viders on the behavioral problems of 21,000 children seen in primary care practices. In this nonreferred sample, 9.2 percent of the children were identified as having clinically significant inattention or hyperactivity. Of these, about 40 percent had conduct problems and 19 percent showed anxiety or sadness. The similarities between these findings and ours are remarkable considering that only 37 percent of clinicians in the study by Wasserman and associates used standardized questionnaires.
Our results, which show that ADHD is frequently associated with comorbid psychiatric disorders in primary care settings, are difficult to reconcile with the results of other studies (
20,
21,
48,
49,
50). Yet the implications for primary care clinicians are substantial. Conventional wisdom about the absence of comorbid disorders among children with ADHD may result from the underdiagnosis of behavioral disorders in the primary care setting. The discrepancy between our findings and clinical lore suggests that the identification of ADHD and comorbid disorders in research studies differs from their identification in pediatric practice. Research studies use systematic efforts to elicit information from parents and clinicians (
12,
13,
14,
15,
16,
17,
18,
48). In clinical practice, primary care practitioners may not routinely collect behavioral information (
21,
51,
52,
53,
54,
55,
56,
57). Thus a large number of youths with impairing psychiatric disorders are undiagnosed and untreated (
52,
53,
54,
55,
56,
57,
58,
59). If parents are reluctant to discuss their children's emotional problems with clinicians, and pediatricians have a low index of suspicion for the presence of ADHD and other mental disorders in youths, these conditions may not be identified without the systematic collection of information (
21,
53,
54,
55,
56).
Since comorbid psychiatric disorders among children with ADHD are associated with a more compromised outcome, and considering that the vast majority of children with ADHD are treated in the primary care setting, our findings call for improved methods of identifying comorbid emotional and behavioral disorders that place some children with ADHD at very high risk of compromised outcomes (
4,
6,
7,
8,
9,
10,
58,
59). Moreover, since many comorbid conditions can be successfully treated, their identification in pediatric practice is of very high clinical relevance. Undiagnosed and untreated psychiatric disorders impair educational and occupational achievement and psychosocial functioning. Such impairments in turn lead to greater use of health care and government resources (
52,
58,
59).
Our study must be interpreted in light of its methodological limitations. Given that children with ADHD were selected on the basis of DSM-III-R criteria, our findings may not generalize to DSM-IV. However, because more than 90 percent of our sample met criteria for at least one DSM-IV subtype, it is likely that our results can be extrapolated to DSM-IV. Because the sample was largely Caucasian, our results may not generalize to minority groups.
Another threat to generalizability stems from our exclusion of subjects who had been adopted or whose nuclear family was not available. However, the generalizability of our findings is limited only to the extent that the pattern of results reported here would differ if we had selected a sample that included adopted children and children whose nuclear family was not available and the proportion of these children differed across the two referral sources. Given that these children are uncommon relative to the children we studied, the rate of referral of this subgroup would have to differ substantially between the pediatric and psychiatric clinics to threaten the conclusions derived from our findings.
Another potential source of bias arises from the lack of direct interviews with children younger than 12 years of age, which may have resulted in underestimation of the prevalence of some disorders. Also, mothers may have a tendency not to report more than one disorder for their children—referred to as the halo effect (
60). These methodological limitations are minimized by the adequate statistical power of our study, the similar numbers of children ascertained in pediatric and psychiatric settings and the adequate gender representation in our sample, and the comprehensive assessment battery we used (
51,
52,
53).