Participants
Participants were a subgroup of all youths whose cases were active in one or more of five San Diego County public sectors of care—child welfare, juvenile justice, special education, alcohol and drug, and mental health—from January through June 1997. Interviews were completed between October 1997 and February 1999, and complete data were obtained for 1,715 (66 percent) of the eligible sample (
3). The 947 participants were aged 13 to 18 years.
Sample weights were assigned to represent the original sample of all youths in the system of care. All numbers reported reflect actual numbers available for analysis; percentages reflect sample weighting procedures.
Of the study subsample of 947, a total of 628 youths (66 percent) were male. The mean±SD age was 15.9±1.6 years. The racial and ethnic distribution was 341 (33 percent) Caucasian, 272 (32 percent) Latino, 194 (21 percent) African American, 75 (8 percent) Asian American or Pacific Islander, and 65 (7 percent) multiracial or other.
Procedure and measures
To assess past-year psychiatric disorders, youths and their parents were interviewed individually with the youth and parent reports of the Diagnostic Interview Schedule for Children (DISC-IV) (
5). The youths were assessed for substance use disorders with the youth report of the Composite International Diagnostic Interview—Substance Abuse Module (CIDI-SAM). Youths were assessed for functional impairment with the Children's Global Assessment Scale and the Columbia Impairment Scale. Youths and their parents were interviewed about service use with the parent and youth reports of the Services Assessment for Children and Adolescents (SACA) (
6). Parents were administered the Caregiver Strain Questionnaire (
7).
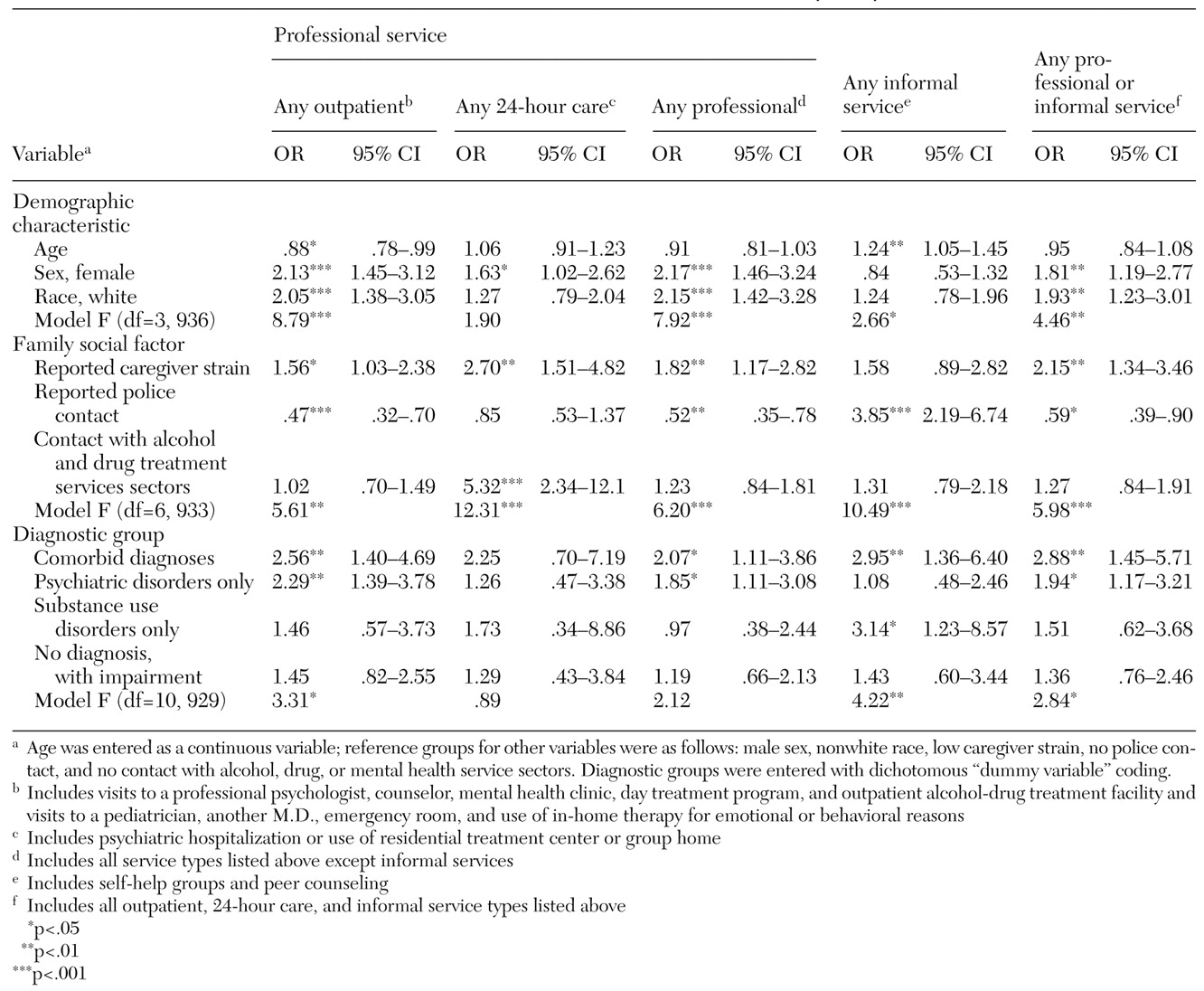
Youths were classified into five diagnostic groups: comorbid psychiatric and substance use disorders (N=174), psychiatric disorder only (N=385), substance use disorder only (N=58), no diagnosis with functional impairment (N=143), and no diagnosis and no functional impairment (N=187). Within each group that had a diagnosis, youths could have multiple diagnoses; for example, youths in the group with psychiatric disorders only could have multiple non-substance use diagnoses.
Mental health services were classified into three groups: professional outpatient, 24-hour care, and informal. Professional outpatient included visits to a professional psychologist, counselor, mental health clinic, day treatment program, and alcohol-drug treatment facility; visits to a pediatrician, another type of M.D., and the emergency department; and in-home therapy for emotional or behavioral reasons. Included in 24-hour care were psychiatric hospitalization and a residential treatment center or group home. Informal services included peer counseling, support groups, and alternative healers. Two summary categories were created: any professional care, which included professional outpatient and 24-hour care; and any service, which included all professional and informal services.
Chi square analyses tested for significant differences in service use rates across diagnostic groups. Multiple logistic regression analyses tested whether these differences remained when the analysis controlled for the effects of potential confounders such as sociodemographic characteristics and caregiver strain. All analyses were conducted with STATA, version 7.0, with data weighted to represent the system-of-care population.