The concept of attention-deficit/hyperactivity disorder (ADHD) has evolved over the last 30 years. DSM-II
1 defined a disorder called “hyperkinetic reaction of childhood (or adolescence).” DSM-III
2 described the disorder as a developmentally inappropriate degree of inattention, impulsivity, and hyperactivity; and DSM-IV
3 described it in terms of inattention and/or hyperactivity-impulsivity. Theories on the pathophysiology of the disorder include the suggestion that it is caused by malfunctioning of the brain dopaminergic system.
4Symptoms of children with ADHD include hyperkinesis and distractibility, variability of task performance, disorganization, an inability to plan or follow through on a plan, an inability to shift set and reprogram activities when needed, and deficient rule-governing behavior. These symptoms have been associated with abnormalities of the brain's frontal lobe systems, particularly the “executive systems.”
5,6 Because there has not been a definitive anatomic localization of all these symptoms to the frontal lobes, we will use the term
frontal systems, rather than frontal lobe, functions.
Although laboratory measures of impulsiveness and response inhibition and other “frontal systems” functions differentiate children with ADHD from normal children, such measures do not consistently differentiate between ADHD and other clinical groups.
12,13 It is therefore necessary to include clinical control groups in studies of frontal systems dysfunction in ADHD. A significant deficiency of most such studies dealing with the role of frontal systems dysfunction in ADHD is the lack of a control group of children with learning disabilities (LD). In a review of studies of frontal systems dysfunction in ADHD by Barkley et al., only 3 of the 22 studies used children with achievement difficulties or LD as controls.
14 Learning disability is a common comorbidity of ADHD.
15 Children with LD commonly have cognitive abnormalities (language, visual, spatial). The suggested association between frontal systems dysfunction and ADHD may, in fact, be related to LD and its cognitive abnormalities and not specifically to ADHD.
The purpose of this study is to examine frontal systems dysfunctions in ADHD children and to assess whether such dysfunctions are specific to ADHD or are equally present in children with learning disabilities. We used tests for frontal systems functions that are appropriate for use in children, and grouped them into four sets: 1) attention, inhibition, and response after cueing; 2) working memory and the ability to maintain a sequence; 3) problem solving and the ability to establish, maintain, and change set and to monitor personal behavior; and 4) motor and verbal learning.
METHODS
Subjects
A frontal systems test battery was administered to 81 consecutive patients evaluated in our neurobehavioral clinic at North Shore University Hospital. Sixty-two patients met the inclusionary criteria: age 6 to 13 years, average intelligence, no major neurological abnormalities (such as Tourette's syndrome or a seizure disorder), and no major psychiatric abnormalities (such as conduct disorder or depression). Informed consent was obtained from parents.
ADHD was clinically diagnosed by strict DSM-III-R criteria,
16 based on behavioral questionnaires (described below) completed by parents and teachers and on parent interviews. The diagnosis was made by a team of experienced clinicians including a child neurologist (Y. F.), a neuropsychologist (J. W. L.), and a child psychiatrist.
Criteria for a diagnosis of LD were reading, mathematics, or written expression achievement abnormalities at or below the 16th percentile, as determined by national standardized or special education testing.
Thirty-six children were diagnosed with ADHD; 26 of these children had LD. Twenty-six children did not have ADHD; of these, 22 had LD. Four children could not be classified as ADHD or LD and were not included in the study. The three study groups were, therefore, ADHD+LD (group 1), LD alone (group 2), and ADHD alone (group 3).
Measures: Behavioral, Cognitive, and Frontal Systems
Parents completed the Child Behavior Checklist (CBCL)
17 and the Conners Parents Questionnaire.
18 The Teacher Response Form (TRF)
19 and the Conners Teachers Questionnaire
18 were completed by the teacher or guidance counselor who was best acquainted with the child.
A neuropsychological battery of tests is routinely used in our neurobehavioral program for children with school-related problems. It includes the Raven Progressive Coloured
20 or Standard Matrices test,
21 the Token Test for Children,
22 the Boston Naming Test,
23 the CELF-R Word Structure subtest,
24 the WRAML Story Memory subtest,
25 the Stanford-Binet-IV Sentence Memory subtest,
26 and the Visual-Motor Integration Test.
27 It also includes the Stanford-Binet-IV Bead Memory subtest
26 and the Selective Reminding Learning Test,
28 which can be considered frontal systems measures by the criteria discussed below and are included in the frontal systems measures for the present study.
An average of the results of the first four measures listed above was calculated to provide a general measure of nonverbal reasoning and language skills, which we have called “General.”
Tests reflecting frontal systems functions that are appropriate for use in children were selected through a review of the literature and were grouped into four domains: Attention-Inhibition-Cueing, Working Memory, Problem Solving, and Learning.
Tests related to attention and inhibition
5 and response after cueing
29 are the Gordon Diagnostic System subtests: the Delay subtest (efficiency, number correct, and total responses), the Vigilance subtest (number correct and commission errors), and the Distractibility subtest (number correct and commission errors).
30 Other tests related to inhibition only are the Rampart drawing of the Dementia Rating Scale
31 with specifically developed scoring rules for errors and the Matching Familiar Figures Test with number correct and error measures.
32Working memory and the ability to maintain a sequence are tested by the Wechsler Intelligence Scale for Children–Revised (WISC-R) or WISC-III Digit Span subtest
33,34 with separate analyses of digits forward and digits backward;
35 the Illinois Test of Psycholinguistic Abilities (ITPA) Visual Sequential Memory subtest;
36 the Stanford-Binet-IV Bead Memory subtest;
26 the Kaufman Assessment Battery for Children (KABC) Hand Movement subtest
37 used on dominant and nondominant hands; and the Token Test for Children, parts three and four.
22The ability to solve problems and, more specifically, the ability to establish, maintain, and change set and the ability to monitor personal behavior
5 are examined by the Wisconsin Card Sorting Test
38 with categories and perseverative error measures.
Learning ability is tested by the Serial Hand Movement Learning Test with a series of six or eight hand movements, constructed specifically for this study from the KABC Hand Movements subtest. The test reflects the ability to learn a complex motor sequence.
5 The Buschke Selective Reminding Learning Test provides measures of verbal learning and consistency.
Data Analysis
Mean z-scores were calculated for each variable for the three experimental groups. In addition, we calculated the proportion of individuals who were “impaired” on each test, defined as those who scored at or below 1 standard deviation of the mean. In a normative sample, 16% of the subjects may score less than 1 standard deviation, and we can expect that 16% of our subjects would score below that point if their distribution were the same as the distribution of the normative group. Binomial statistics were used to assess the likelihood that the proportion of patients scoring at or below that point was greater than would be expected by chance.
Comparison of the study groups (ADHD+LD, LD alone, ADHD alone) was performed by analyzing each variable with a one-way analysis of variance (ANOVA) and Student-Newman-Keuls post hoc mean comparisons (significance set at the 0.05 level) done by SPSS/PC+ Release 6.0.1.
39 Multiple ANOVAs were chosen over a single multivariate analysis because of the exploratory nature of the study and the correlated nature of the measures.
40RESULTS
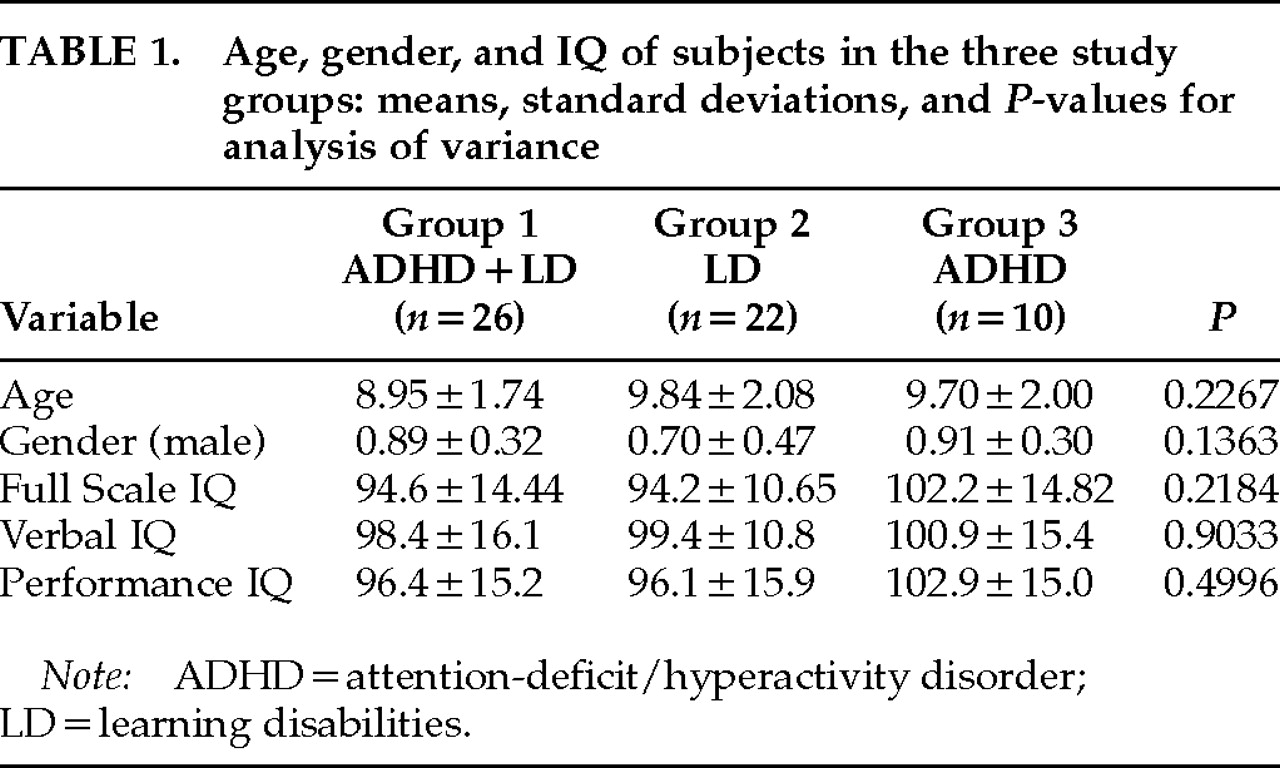
There were no significant differences of age, gender, or Full Scale, Verbal, or Performance IQ among the experimental groups (
Table 1).
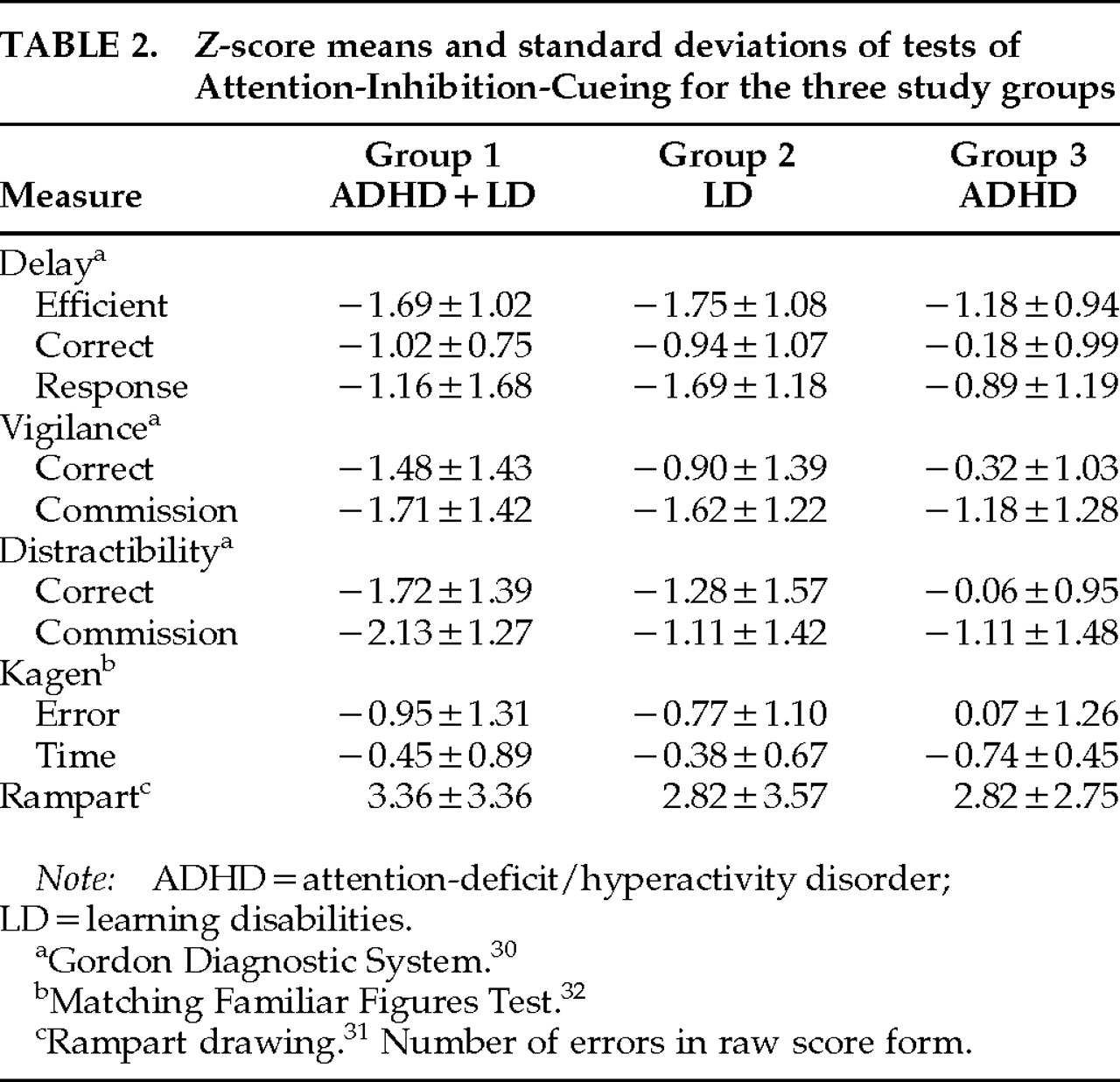
Table 2,
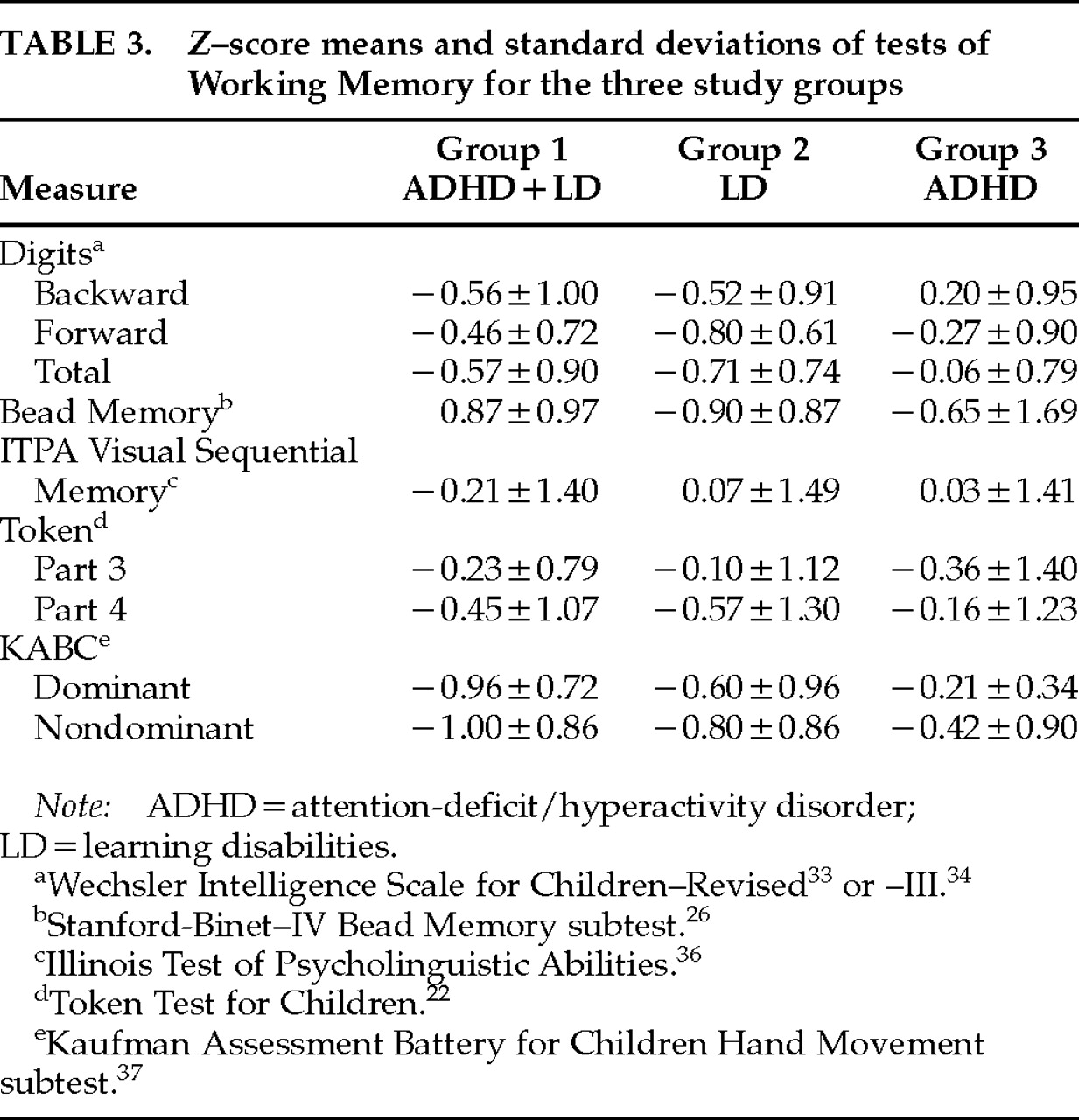
Table 3, and
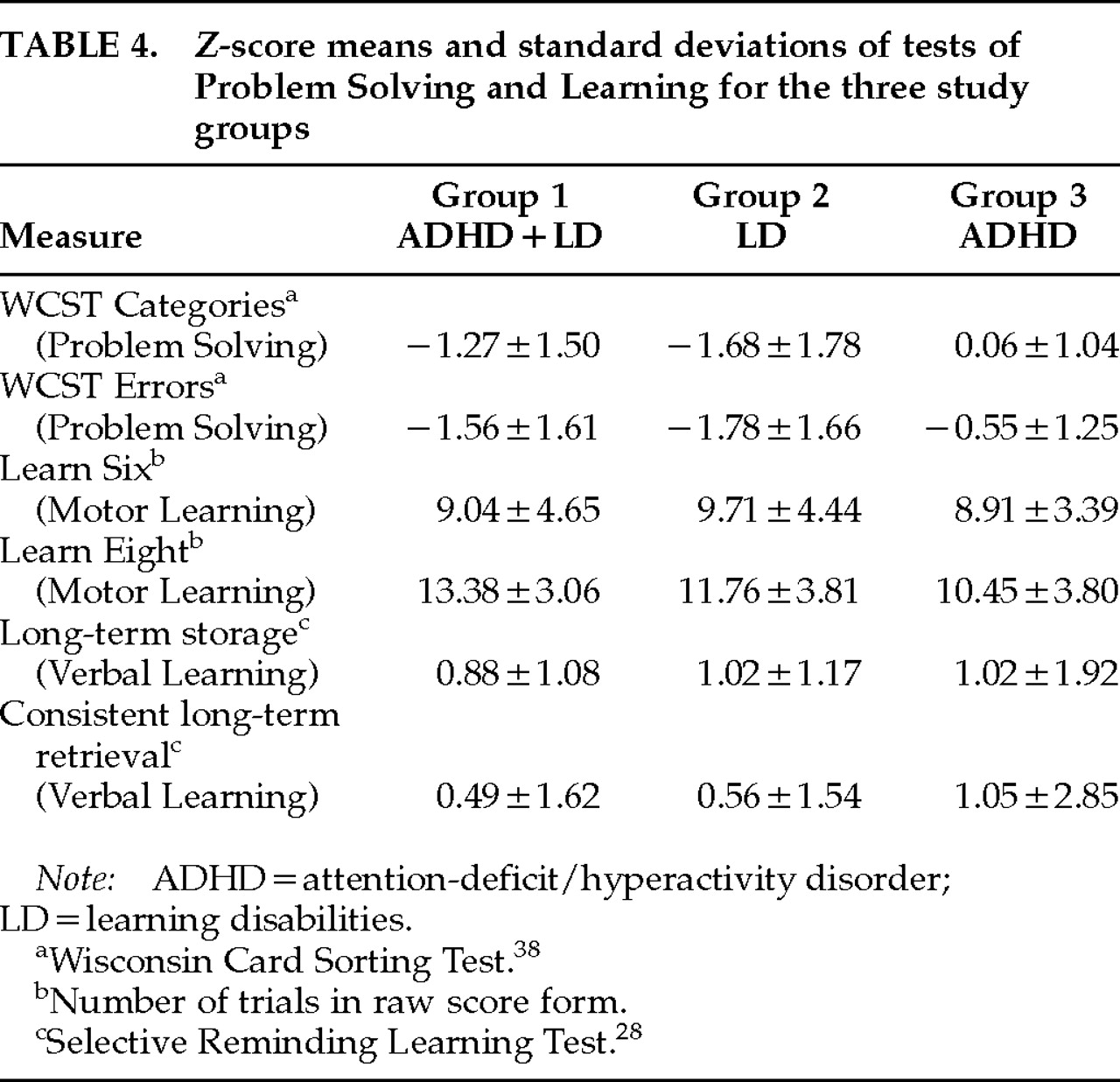
Table 4 show
z-score means and standard deviations of frontal systems tests grouped under Attention-Inhibition-Cueing, Working Memory, and Problem Solving and Learning, respectively. The mean
z-scores for many measures of Attention-Inhibition-Cueing and of Problem Solving are –1 or less.
The number of tests with a mean z-score of –1 or less is 10 (45%) of the 22 tests for which standardized norms are available for the ADHD+LD group, 7 of 22 (32%) for the LD-only group, and 3 of 22 (14%) for the ADHD-only group. The two groups with LD (groups 1 and 2) appear, therefore, more impaired than the ADHD-only group (group 3).
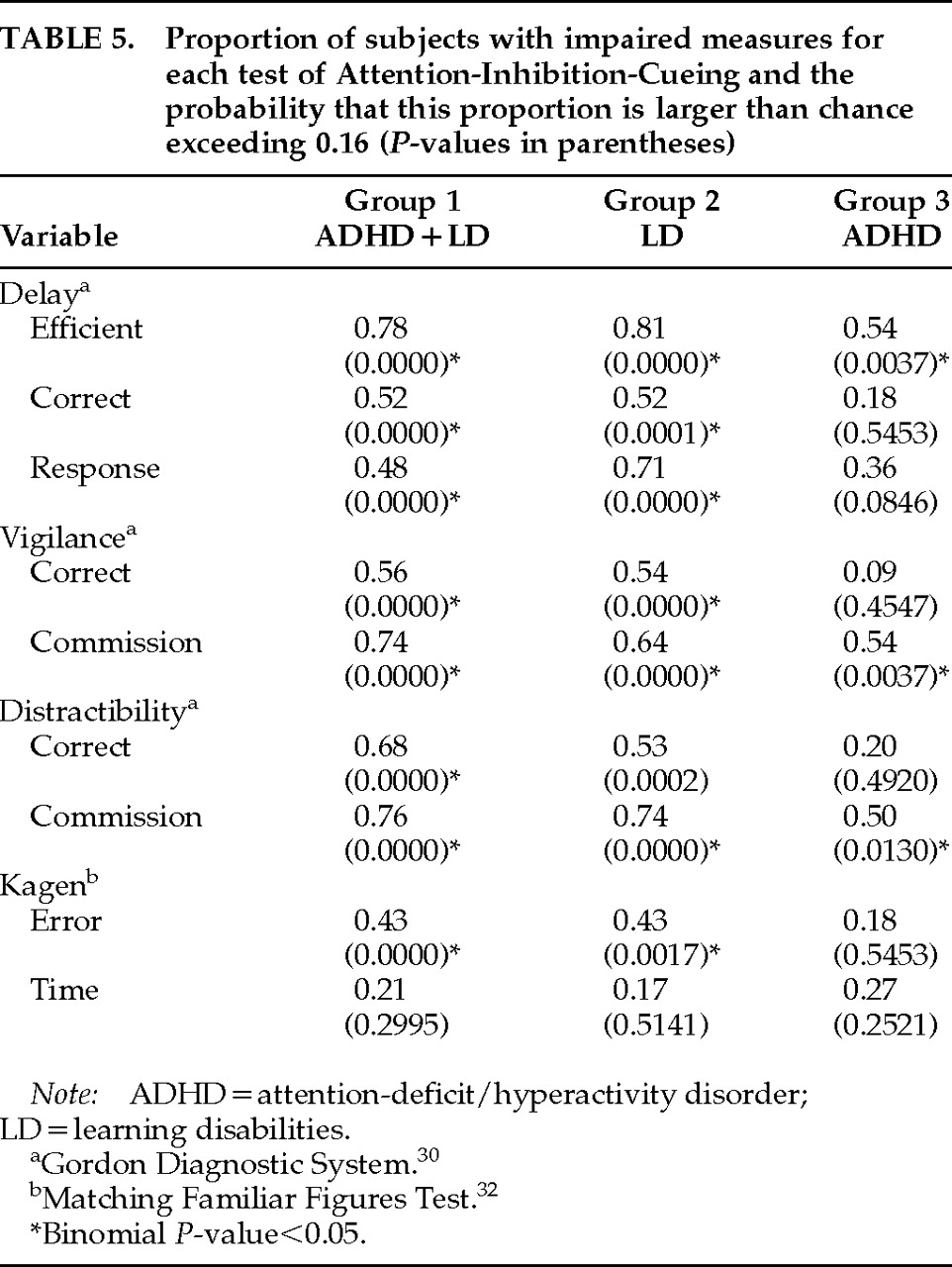
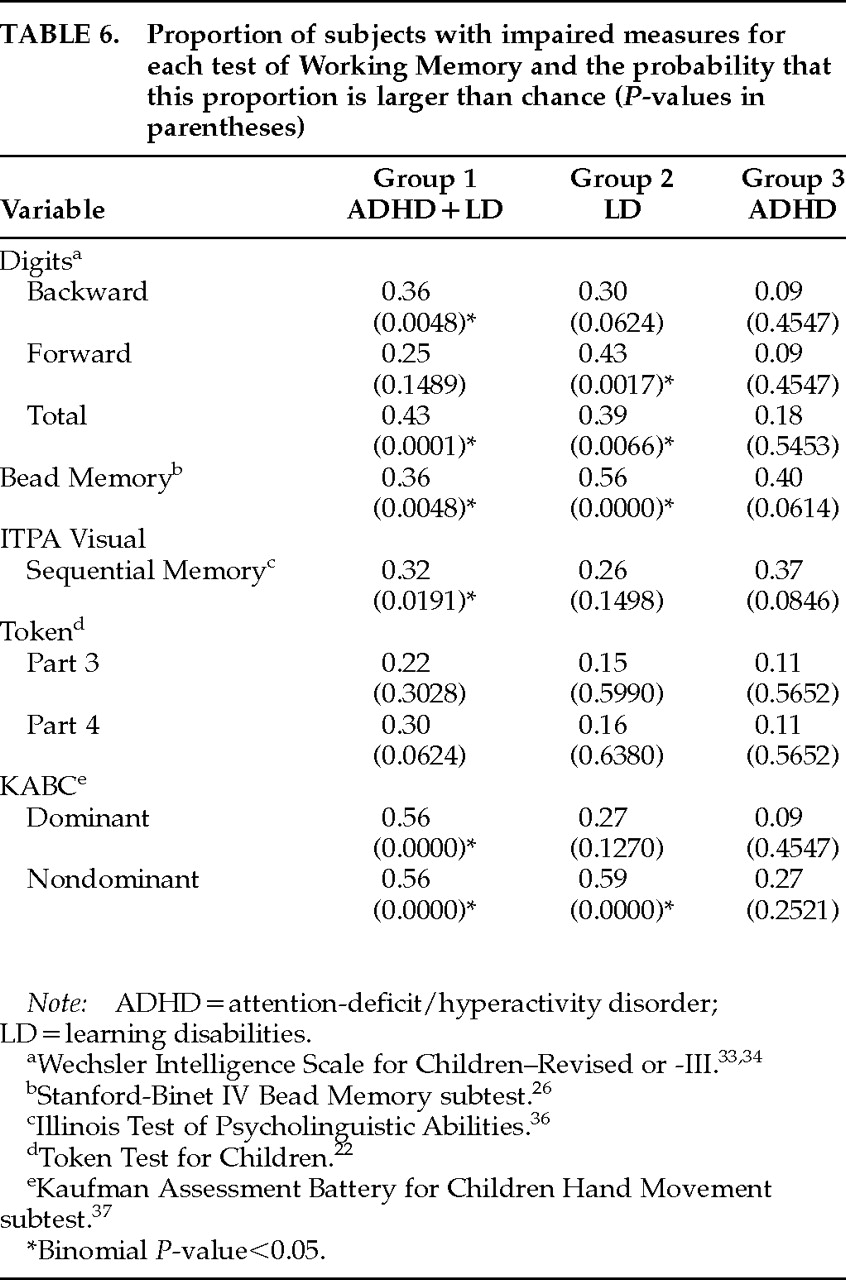
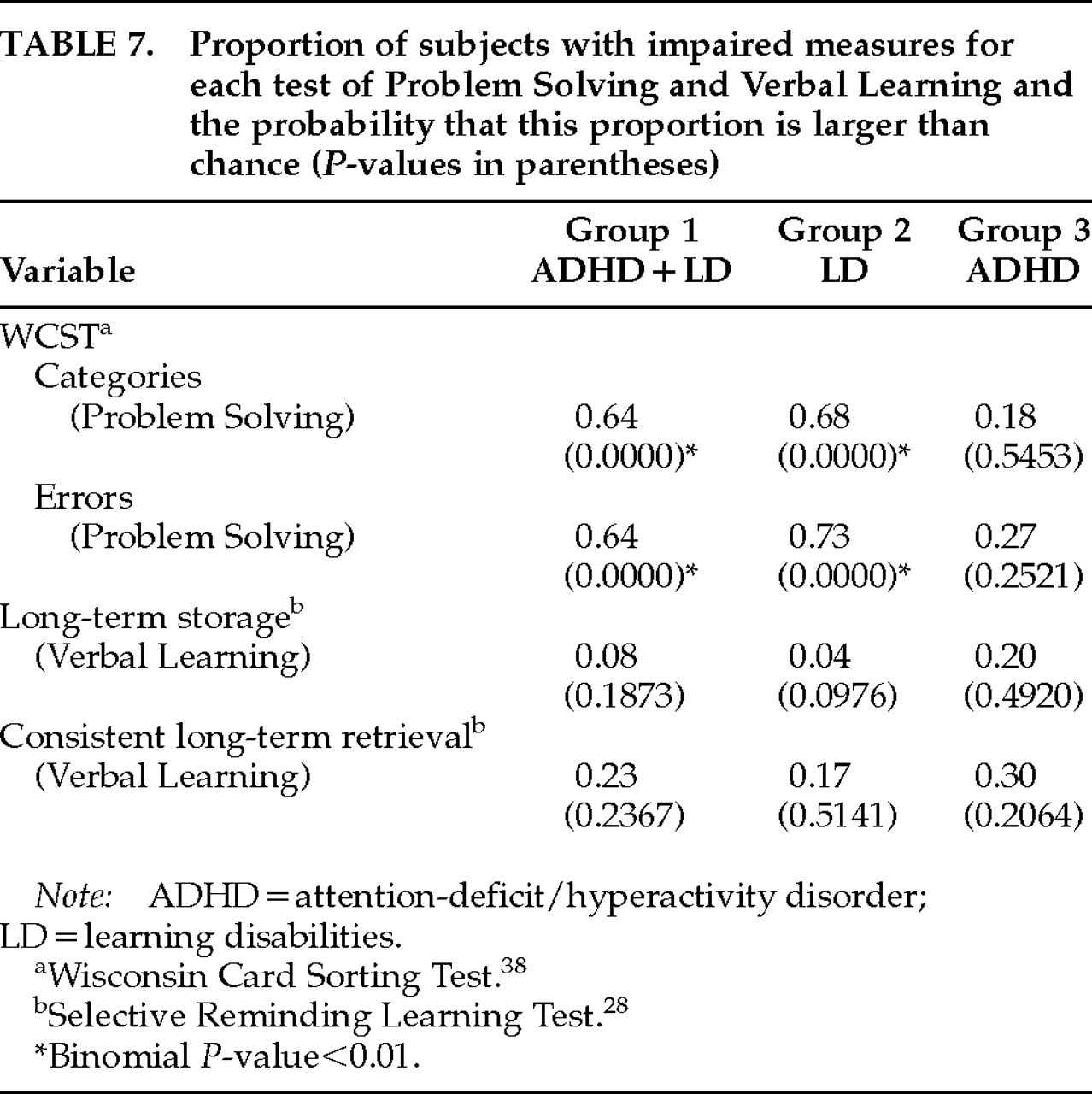
The proportion of subjects with impaired test scores (
z-scores of –1 or less), and the probability that this proportion is larger than would be expected by chance (0.16) according to the binomial test, are calculated for each test (
Table 5 through
Table 7). The proportion of subjects with impaired test scores is greater than chance for many measures of Attention-Inhibition-Cueing and of Problem Solving. The percentage of tests with a significant proportion of impaired test scores for tests of Attention-Inhibition-Cueing is 89, 89, and 33 for groups 1, 2, and 3, respectively; for Working Memory, 67, 44, and 0, respectively; for Problem Solving, 100, 100, and 0, respectively. There is, therefore, more impairment in the two groups with learning disabilities (groups 1 and 2) than in the ADHD-only group (group 3) for all the categories of tests. Verbal Learning was normal for the three groups.
The Rampart Drawing test from
Table 2 and the motor learning measures from
Table 4 were not included in this summary because norms were not available to make them comparable to the other measures. Verbal Learning was normal (at mid-average) for all groups.
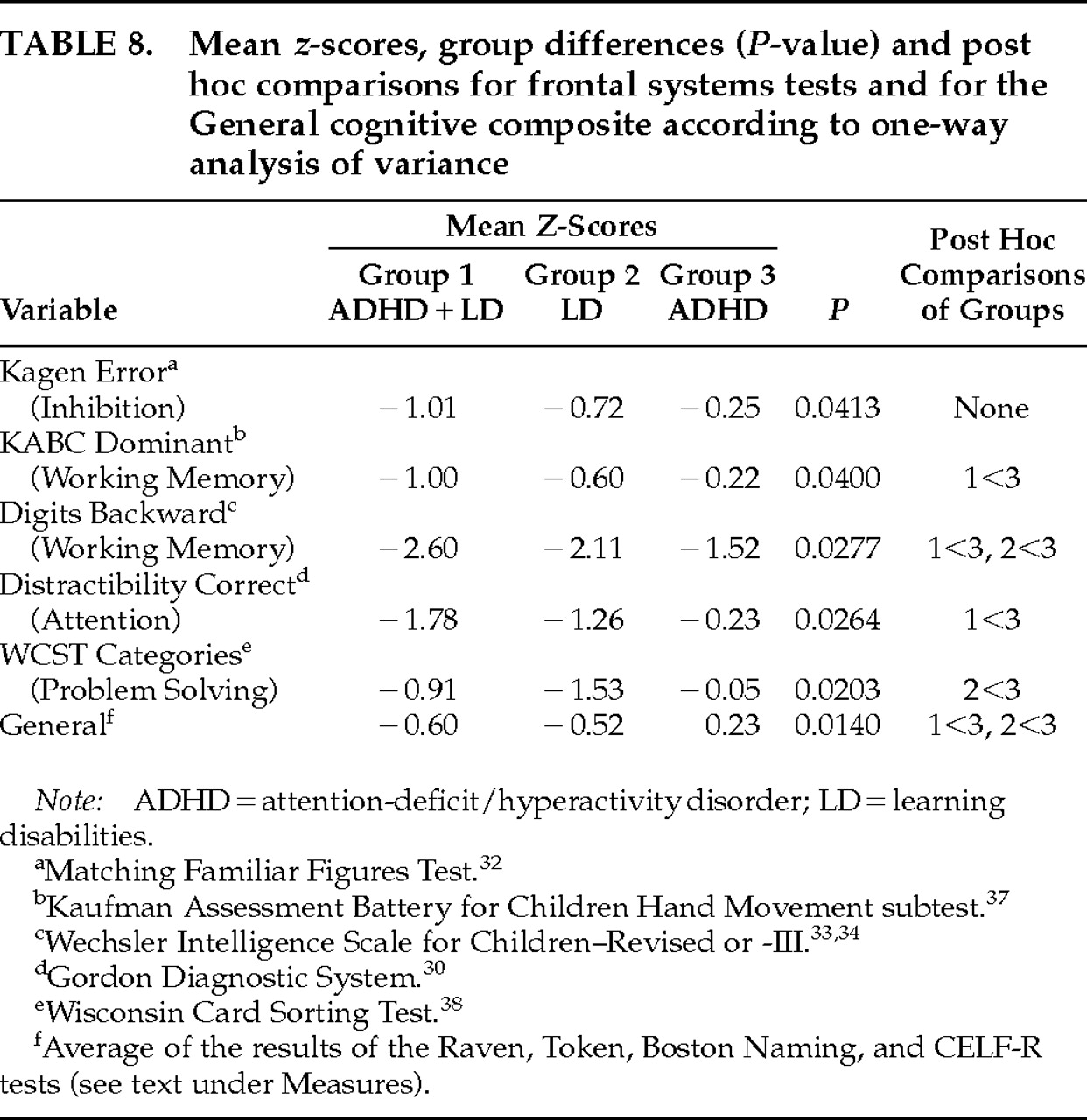
Table 8 shows the results of a one-way ANOVA comparing the mean
z-scores of the three experimental groups, along with results of post hoc Student-Newman-Keuls mean comparisons tests. Only tests with probability values of less than 0.05 are presented. The groups differed significantly on the Correct answers of the Distractibility test and on the Kagen Error test (Attention-Inhibition-Cueing); on the KABC dominant and the Digits Backward tests (Working Memory); and on the Categories part of the WCST (Problem Solving). The significant post hoc mean differences demonstrate that the groups with LD (groups 1 and 2) perform more poorly than the group of ADHD only (group 3).
Table 8 also shows the results of a one-way ANOVA of the “general” measure of cognition (composed of an average of the results of the Raven, Token, Boston Naming, and CELF-R tests). The groups with learning disabilities (groups 1 and 2) had a significantly worse performance than the ADHD-only group (group 3;
P<0.014).
DISCUSSION
Measures of response inhibition and sustained attention, ability to respond after cueing, and problem solving were often impaired (z-score means less than –1) for the three study groups, and the number of individuals with impaired performance on these measures, as well as on measures of working memory and motor learning, was often higher than would be expected by chance. We therefore confirm that ADHD, LD, and ADHD+LD subjects do not perform well on tests that examine executive and other frontal systems functions.
Our study demonstrates, though, that abnormalities of these functions are not specifically related to ADHD. The two groups of LD patients (LD and ADHD+LD) performed worse than the ADHD-only group. Also, the ADHD+LD group did not differ significantly from the LD-only group, showing no evidence for an ADHD+LD synergism. Therefore, there is a stronger LD effect than an ADHD effect on executive frontal systems functions.This result is not due to the choice of tests, to IQ difference among the groups, to lack of statistical power, or to our ADHD definition. Our measures were chosen to test the full range of frontal systems functions. They were not chosen to differentiate children with learning disabilities from children with ADHD. There was no significant difference in general intelligence between the groups. Absence of ADHD effect is not related to lack of statistical power, because a significant difference was found between the small ADHD group (group 3) and the LD and ADHD+LD groups, whereas no significant difference was found between the larger ADHD+LD and LD groups. We also recalculated group differences after applying more stringent criteria for ADHD diagnosis (by increasing the number of affirmative answers on the DSM-III-R questions needed for ADHD diagnosis from 6 up to 11). There was still no significant consistent difference between the ADHD and the non-ADHD groups.
The high frequency of LD among ADHD children makes differences between an unselected group of ADHD and normal children impossible to interpret as due to ADHD alone. Most studies of executive and other frontal systems functions in ADHD do not control for the presence of LD. Barkley et al.
14 reviewed 22 such studies. Only three had a control group of children with LD, usually reading disability: Felton et al.,
41 using linguistic fluency and semantic fluency tests, found no differences between reading-disabled groups with or without ADD with hyperactivity (ADD+H). McGee et al.
42 found that ADD+H 13-year-old children with reading disabilities had lower scores on the Rey-Osterrieth Complex Figure Test than did children with only ADD+H, again demonstrating a reading disability rather than ADHD effect. Douglas and Benezra,
43 again using the Rey-Osterrieth Complex Figures Test, did not find a significant difference between the performance of children with reading disabilities and children with ADD+H. These three studies, although using somewhat different test batteries, demonstrate that the presence of LD is at least an equal factor to ADHD, and possibly a more important one, in correlating with frontal systems functions.
Barkley et al.
14 also reported their own study comparing results of 26 measures of “frontal lobe functions” in clinic-referred small groups of ADD+H boys, ADD–H boys, LD–non-ADD boys, and normal control subjects. Significant differences were found between normal control subjects and the other groups on two Stroop measures, namely, words and interference. Omission errors on a continuous performance task differentiated ADD+H boys from normal control subjects, and ADD–H boys from the LD boys and normal control subjects.
Robins
44 studied the responses of children with ADHD, LD, and ADHD+LD on 12 neuropsychological measures including subtests of the WISC-R, the Beery, Trail Making, Matching Familiar Figures Test, Rey Auditory-Verbal Learning Test, and Gordon Delay and Vigilance subtests. Significant differences between the groups on a multiple discriminant-function analysis were related to “the constructs of self-regulation and planning/accuracy/speed.” The ADHD and ADHD+LD groups were more impulsive, less accurate, and more variable in terms of self-regulation than the LD sample. The three groups did not differ on other executive measures including those of sustained attention, auditory memory for digits, or verbal learning.
August and Garfinkel
45 raised the question of whether or not defective cognitive mechanisms are specific to ADHD. They compared three groups of ADHD children and normal control subjects by using several cognitive measures. One ADHD group included children who also had a reading/spelling disability (the Cognitive group). The other two groups of ADHD children had either low or high scores on the Conduct Disorder-Aggressive scale of the Yale Children's Inventory and comprised the Mild Behavioral and Severe Behavioral Groups, respectively. The Mild Behavioral group did not meet the clinical cutoff on the Conduct Disorder-Aggressive scale and will be considered for the purpose of this discussion an ADHD group without “conduct-aggression” behavior or reading/spelling disabilities. The Cognitive group differed significantly from the Mild Behavioral group on several measures. The Cognitive group made significantly more errors than the Mild Behavioral group on a continuous performance test, had more omissions, commissions, and total errors on a maze test (typically ADHD and frontal measures), and performed more poorly on a test of word knowledge, rapid word reading, and recognition of fragmented words. In other words, the group with reading/spelling disability performed worse than the ADHD-only group, a finding consistent with our results. It is of note that this study did not attempt to control the findings for intelligence, discussing the point that matching or controlling for intelligence may be an excessive measure. Certain cognitive deficits of reading-disabled students may contribute to a lower general intelligence, but this does not mean that they have deficits in all areas as a correction for general intelligence would imply.
Korkman and Pesonen
46 compared three groups of children—ADHD only, LD only, and ADHD+LD—on 19 cognitive measures. Individual ANOVAs showed significant differences among the three groups on measures of attention and response control, storytelling, graphomotor skill, and digit span. Although post hoc analyses were not reported,
t statistics between the LD-only and the ADHD-only groups demonstrated that the ADHD group performed better on the measures of auditory analysis of speech, storytelling, and digit span, whereas the LD group performed better on tests of response control. Consistent with our study, there were no significant differences between the two groups on attention measures.
These authors also report significant differences in Verbal IQ scores among their groups, with the ADHD-only group having the highest, as is the case in our study. They did not correct for this difference, noting that it may distort true conditions given the tendency toward specific language deficiencies in children with reading and spelling problems.
Our study has some limitations, chiefly the small number of ADHD-only (group 3) patients, the inclusion of multiple forms of LD (reading, mathematics, or written expression), and the usual referral bias of a specialty clinic. Nevertheless, our results suggest that abnormalities detected in laboratory tests of impulsive response, attention, and problem solving, which are considered frontal systems or executive functions, are not exclusive ADHD characteristics and are equally (or more) prevalent in children with LD. This result would be expected, given the complexity of the laboratory tests and the complicated integration of cognitive processes needed for their successful completion; the close association between brain centers of “processing” and those of “executive functions” that may be impaired in LD and ADHD, respectively; and the broad characterization of executive control as discussed by Stuss and Benson.
5,6 In addition, our results suggest that tests assessing only frontal systems or executive functions cannot be used to differentiate ADHD from LD.