The therapeutic effectiveness of electroconvulsive therapy, at least for unilateral nondominant electrode placement (UL), depends in part on the degree to which the stimulus intensity exceeds the seizure threshold—that is, on the relative stimulus intensity.
1–3 Evidence suggests that for bilateral (BL) ECT, higher relative stimulus intensity is associated with a more rapid therapeutic response,
1,2 whereas barely suprathreshold UL ECT has a significantly reduced antidepressant potency compared with moderately suprathreshold UL ECT (150% above threshold).
1–3 This information might be applied clinically by determining the seizure threshold at the first treatment
4,5 and subsequently administering treatments at a desired intensity above that threshold. Maintaining such a desired relative stimulus intensity during the course of treatments is confounded, however, by a variable increase in seizure threshold that occurs over the treatment course.
1,6–8 Such a rise in the seizure threshold will lessen the degree to which a fixed stimulus dosage exceeds the seizure threshold and thus will possibly result in diminished treatment therapeutic potency, particularly for UL ECT.
Whether increases in the seizure threshold that decrease relative stimulus intensity during ECT treatment course affect therapeutic potency has not been adequately studied. The small number of studies that have examined relations between the anticonvulsant effects of ECT and its therapeutic efficacy have produced inconsistent findings.
1,2,4,7–9 Of these studies, only one examined the therapeutic effect of decreases in relative stimulus intensity with UL ECT.
9 The results of that study are difficult to interpret, however, because there were only 9 subjects, and they were treated for mania with a mixture of dominant and nondominant UL ECT.
If decreases in relative stimulus intensity over the treatment course diminish the efficacy of ECT, it would be clinically useful to have a means to detect the rise in seizure threshold and thereby be able to increase stimulus intensity to maintain an adequate relative stimulus dosage.
6 In the absence of such information, the practitioner must either perform multiple seizure threshold titrations over the treatment course, which is impractical, or use BL or high-intensity UL ECT in all cases. Unfortunately, the latter two alternatives would result in greater adverse cognitive effects.
1,2,6,10–12Recent research by our group
3,13,14 and others
15 suggests that ictal EEG measures of the ECT seizure may, in fact, be used to provide a means of estimating relative stimulus intensity. In fact, ictal EEG measures of the ECT seizure—including immediate poststimulus amplitude, midictal amplitude, immediate postictal amplitude, ictal slow-wave duration, immediate poststimulus coherence (interhemispheric correlation of low frequency activity), and time to the onset of high-amplitude ictal slowing—have been shown to be sensitive to relatively large differences (125%–150%) in relative stimulus intensity.
3,13–15 Further, ictal EEG evidence of diminished ECT seizure intensity has been found to be associated with ECT nonresponse.
3,14,15 However, no study has directly examined whether such ictal EEG indices are sensitive to the somewhat smaller decreases in relative stimulus intensity that occur as seizure threshold rises over the clinical ECT course (47%–50% by treatments 5–7
4,7 and 42%–99% by the end of the treatment course
4,8,9) and whether such indices might signal changes in the therapeutic potency of the ECT seizure.
This report examines the relationship between this anticonvulsant effect of ECT, ictal EEG measures of seizure intensity, and treatment therapeutic potency.
RESULTS
Change in Seizure Threshold From Treatment 1 to Treatment 6
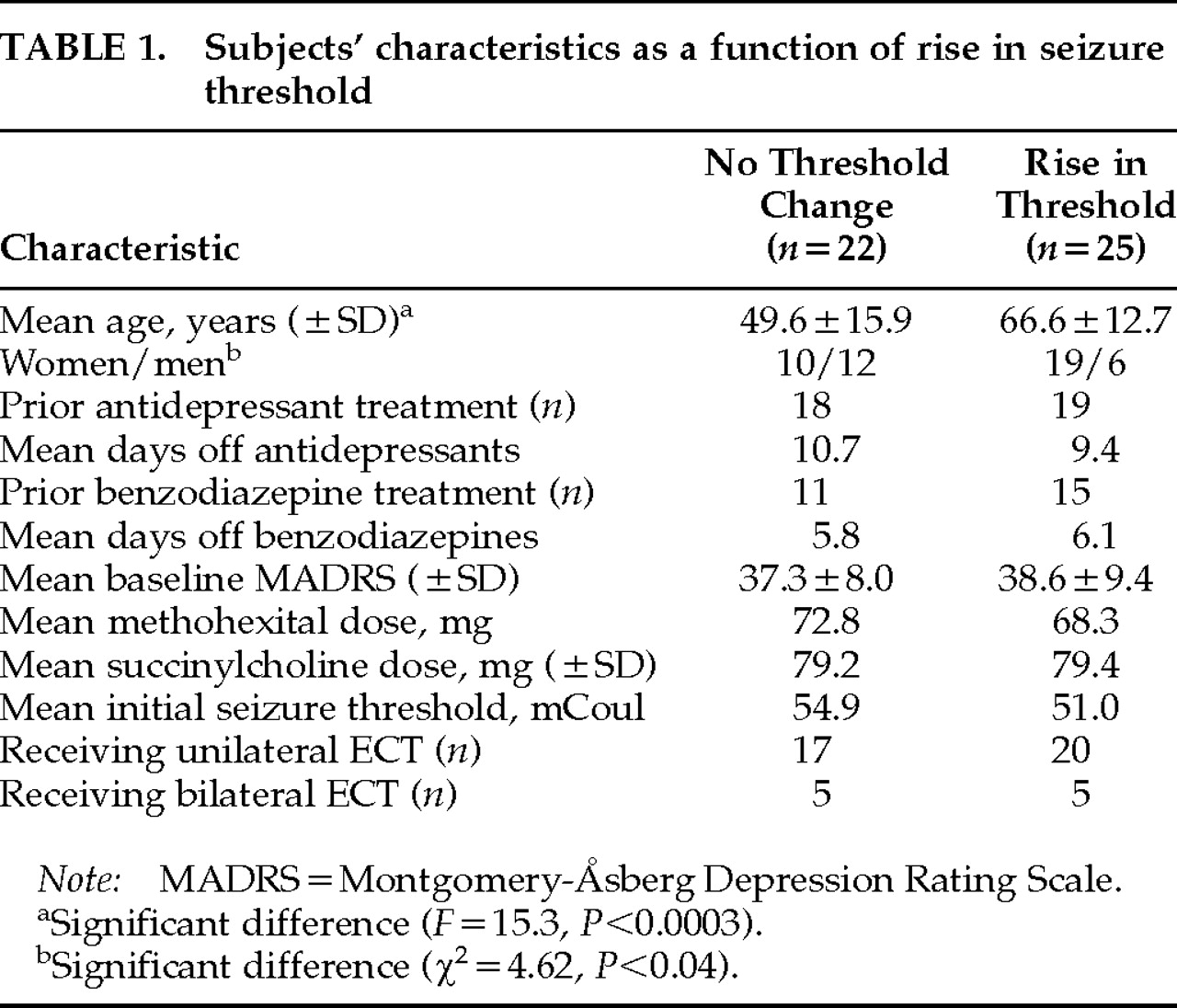
The seizure threshold rose by at least 50% in 25 of 47 subjects. Of those 25 subjects, the seizure threshold increased 50% (one dose level of the seizure threshold titration protocol used)
5,7 for 21 subjects, and for 4 subjects there was a 125% increase (2 dose levels of the seizure threshold titration protocol). The mean percentage increase in seizure threshold for the entire group was 40%. Subject characteristics as a function of whether there was a rise in seizure threshold appear in
Table 1.
In order to study the relationship between increases in the seizure threshold, electrode placement, and gender, a logistic regression was carried out; the percentage rise in threshold served as the dependent variable, and electrode placement, age, and gender were the independent predictor variables. As previously reported for the original sample,
5,7 older subjects were significantly more likely to have a rise in seizure threshold (
F=9.5,
P<0.002). Electrode placement and gender were not related to the change in the seizure threshold.
Relationship Between a Rise in Seizure Threshold and the Therapeutic Response at Treatment 6
A logistic regression was carried out in which rise in seizure threshold, electrode placement, age, and gender were simultaneously entered into a model of therapeutic response at treatment 6 (dichotomous response criteria based on the CGI described above). A rise in threshold was associated with a significantly lower likelihood of therapeutic response (χ
2=4.64,
P=0.031), and older subjects were more likely to be nonresponders (χ
2=5.32,
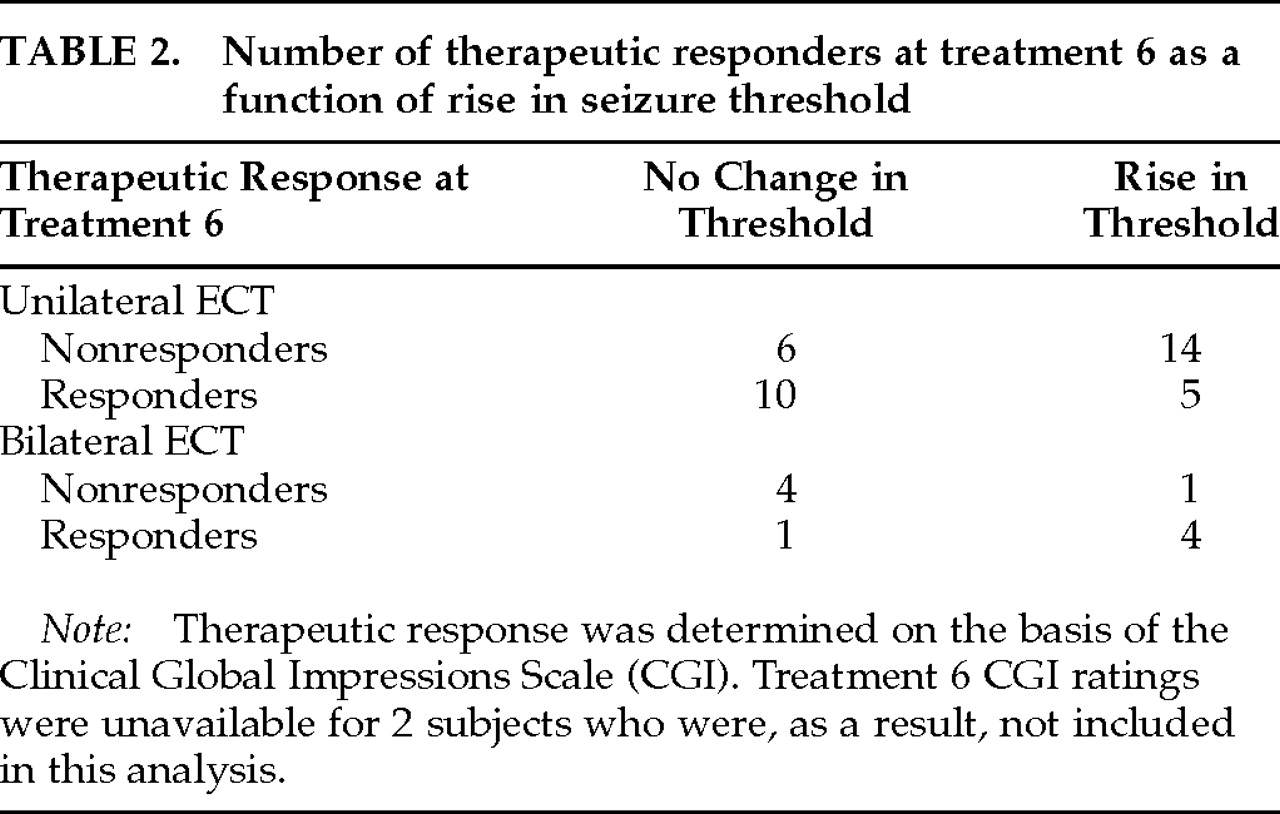
P=0.021). Older subjects were also more likely to have a rise in seizure threshold. Electrode placement and gender were not found to be related to therapeutic outcome in this model. However, a significant association between these two variables was seen only with UL ECT. For UL ECT, there were significantly greater numbers of therapeutic responders among those who did not have a rise in seizure threshold (lowering of relative stimulus intensity; 63%, 10/16) versus those in whom the seizure threshold did rise (26%, 5/19; χ
2=4.64,
P=0.031;
Table 2). It is of note that none of the 4 individuals receiving UL ECT who had a 125% rise in seizure threshold were therapeutic responders at treatment 6. In terms of therapeutic response determined on the basis of MADRS ratings, there was a trend for individuals who experienced a rise in seizure threshold to be nonresponders (53%, 9/17, vs. 25%, 5/20; χ
2=3.05,
P=0.08). However, treatment 6 MADRS scores were not significantly different as a function of rises in the seizure threshold.
Relationship Between a Rise in Seizure Threshold and the Ictal EEG
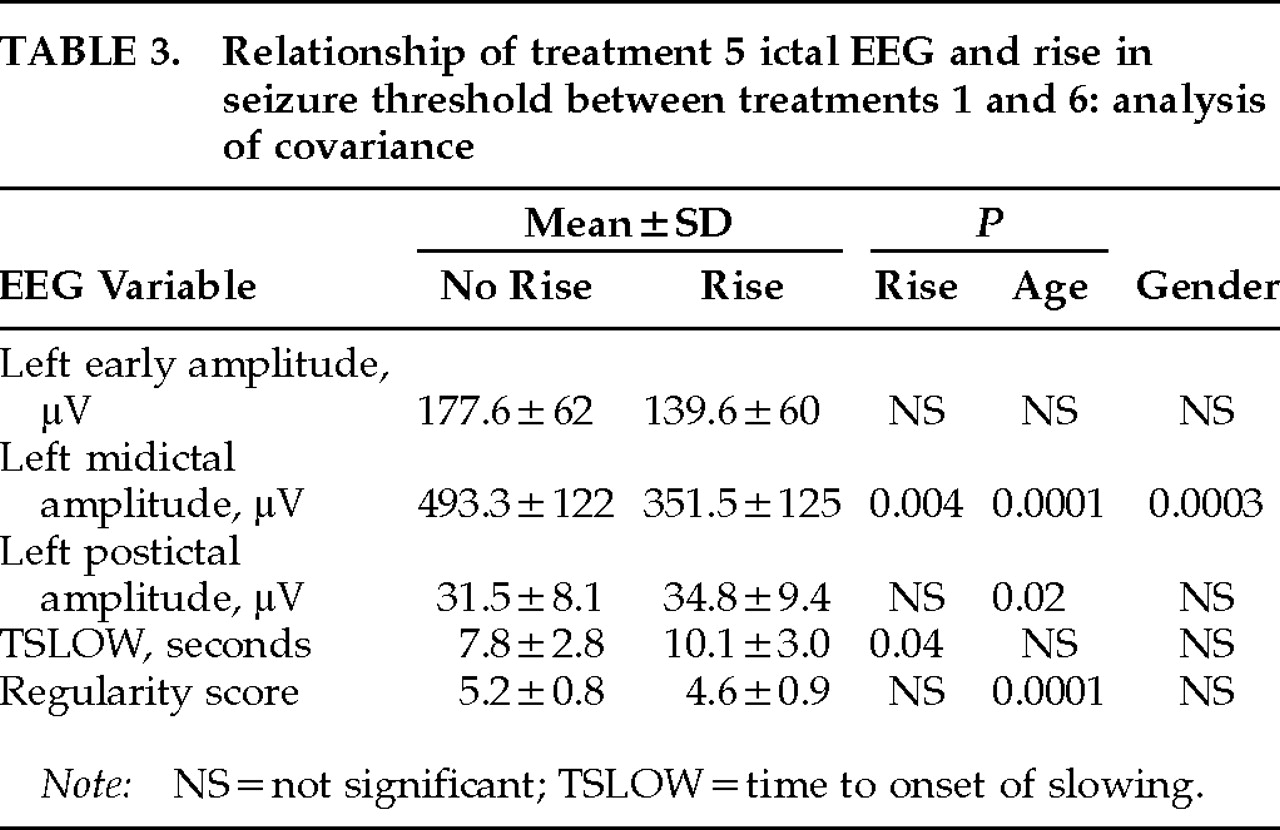
A multivariate analysis of covariance (MANCOVA) was carried out with treatment 5 data for all five ictal EEG variables serving as dependent variables. Rise in threshold (this was a dichotomous variable, rated 0 for no detectable change in threshold [<50% rise] and 1 if the threshold rose at least 50%) was an independent variable, along with electrode placement and the interaction of these two variables. Age and gender served as covariates. The analysis was intended to test the hypothesis that subjects with an increase in seizure threshold from the first to the sixth ECT treatment would also have evidence of decreased seizure intensity in treatment 5 ictal EEG variables. Results appear in
Table 3. A significant multivariate main effect of rise in threshold was found (multivariate
F=4.9, df=5,25,
P=0.003). Ictal EEG evidence of diminished seizure intensity was associated with rises in the seizure threshold only for UL ECT (
F=2.88, df=5,32,
P=0.029). Gender and age were both significant covariates (gender:
F=3.22, df=5,32,
P=0.02; age:
F=5.26, df=5,32,
P=0.0012).
Follow-up univariate analysis showed that patients with a rise in the seizure threshold had evidence of decreased seizure intensity in all ictal EEG variables, although this effect was only significant for midictal magnitude (
F=10.1,
P=0.004) and TSLOW (
F=4.9,
P=0.04;
Table 3). Age and gender were significant covariates for a number of measures (
Table 3).
We also tested whether the difference in treatment 2 and treatment 5 ictal EEG variables was related to increases in seizure threshold occurring between treatments 1 and 6. This approach is advantageous for clinical application because it eliminates the problem of interindividual variation in the ictal EEG.
6 Repeated-measures analysis of variance was performed with ictal EEG indices at treatment 2 and treatment 5 serving as the repeated measures and rise in threshold serving as the independent variable. A significant effect of rise in threshold over time was seen only for left midictal amplitude (
F=6.4,
P=0.02). For subjects who had no change in threshold, the mean midictal amplitude rose from 465 μV (SD=129) at treatment 2 to 479 μV (SD=131) at treatment 5, whereas for those who had a rise in seizure threshold, the mean midictal amplitude decreased from 420 μV (SD=121) at treatment 2 to 363 μV (SD=131) at treatment 5, indicative of a significant decrease in seizure intensity.
An Ictal EEG Model to Predict When a Rise in Seizure Threshold Has Occurred
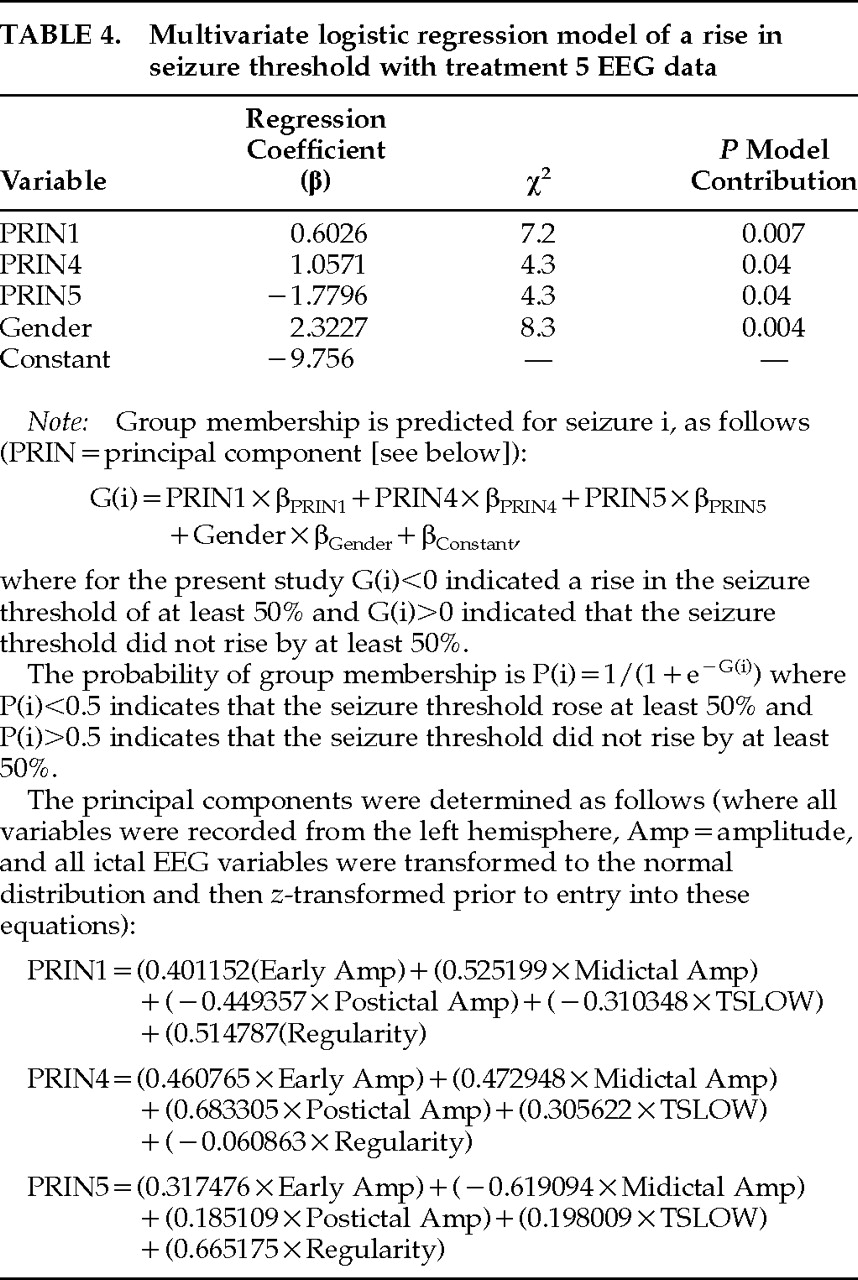
A multivariate logistic regression model of whether a rise in threshold occurred between treatments 1 and 6 was developed with the principal components of treatment 5 left-sided ictal EEG variables and both age and gender for UL ECT data (variables added stepwise). Data from subjects who received BL ECT were not included in this analysis, since a relationship between rise in threshold and both therapeutic outcome and ictal EEG variables was found only for UL ECT. As shown in
Table 4, only EEG principal components 1, 4, and 5 and gender contributed significantly (
P<0.05) to the prediction of a rise in threshold and were included in the final model. In order to estimate the expected predictive accuracy of this model, the “leave one out” procedure was used, demonstrating an accuracy (percentage of correct classifications) of 82%, with an 88% sensitivity (13/15 accuracy for identifying a rise in threshold) and a specificity of 78% (14/18 accuracy for identifying no change in threshold). Age was not included in the model because it provided no additional information to the EEG data, so that once EEG variables were entered into the model it no longer made a significant contribution to the prediction of a rise in threshold. In a model including only gender and age, both contributed to prediction of rise in threshold, but the expected accuracy of the model was only 66%. This finding suggests that although age is predictive of a rise in threshold, EEG indices account for that predictive capacity and provide significant additional ability to predict changes in the seizure threshold.
The logistic regression model based on the principal components of treatment 5 ictal EEG data is most heavily dependent on midictal amplitude, as would have been expected on the basis of the MANCOVA described above. For all three principal components included in the model, this variable is weighted heavily and in a polarity such that greater midictal amplitude is associated with prediction of no threshold change. Also, for the first principal component, which made the largest contribution to the model, greater seizure intensity was associated with a greater likelihood of no seizure threshold change for all 5 ictal EEG variables (higher ictal amplitude and regularity, lower postictal amplitude, and TSLOW).
In order to develop a model that capitalized on the advantages of an intraindividual comparison of EEG data across the relevant portion of the treatment course, a multivariate logistic regression model of rise in threshold was developed, using the difference between treatment 2 and treatment 5 ictal EEG data, age, and gender. The variables that contributed significantly to this model were principal component 5 (χ2=5.1, P=0.03), age (χ2=8.3, P=0.004), and gender (χ2=4.4, P=0.04). When tested with the “leave-one-out” procedure, this model had a predictive accuracy of 80% with an expected sensitivity of 76% (13/17 correct prediction rate for a rise in threshold) and an associated specificity of 85% (11/13 correct prediction rate for no change in threshold) for identifying a rise in seizure threshold. Principal component 5 of the differences between treatment 2 and treatment 5 ictal EEG variables is dominated by the difference in midictal magnitude, as would have been expected from the repeated-measures analysis described above. The weighting of this variable in the model was such that a large positive difference between treatment 2 and treatment 5 midictal amplitude (decrease in midictal amplitude from treatment 2 to treatment 5 suggesting a decrease in seizure intensity) was associated with a greater likelihood of a rise in seizure threshold.
Relationship Between Treatment 5 Ictal EEG and Therapeutic Response
A multivariate analysis of covariance was carried out for all subjects with treatment 5 data for all five ictal EEG measures serving as the dependent variables. Therapeutic response (derived from treatment 6 CGI ratings) was the independent variable, along with electrode placement and their interaction, and age and gender were covariates. A significant main effect for therapeutic response was found (F=2.72, P=0.037), as well as a trend for electrode placement (F=1.98, P=0.08). There was no significant electrode placement by therapeutic response interaction found. Age was a significant covariate (F=3.92, P=0.007), but gender was not.
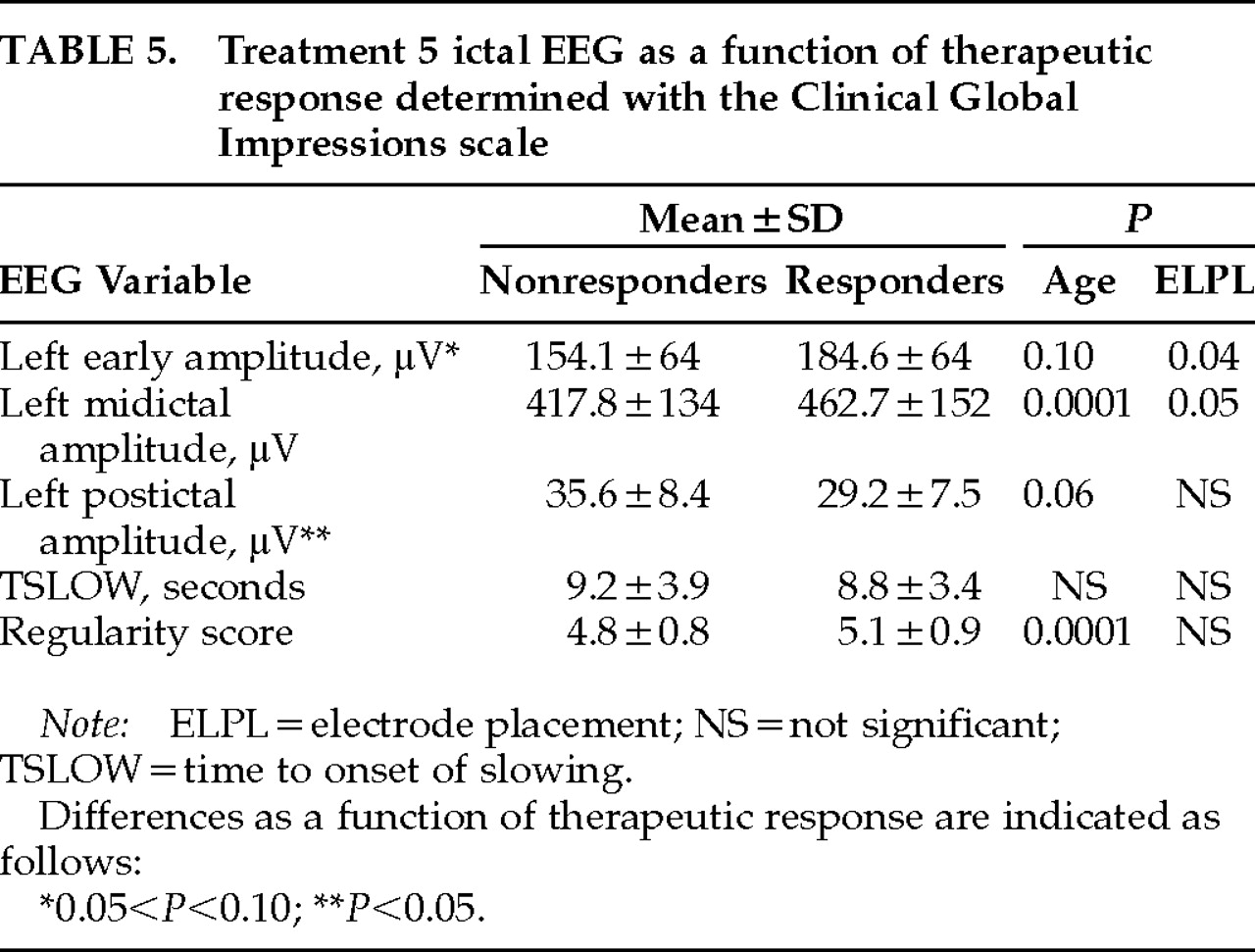
On the basis of these findings, follow-up univariate analyses of covariance were carried out with each EEG variable as the dependent variable, CGI-based dichotomous therapeutic response and electrode placement as the independent variables, and age as a covariate. The results (
Table 5) are consistent with greater seizure intensity (greater early and midictal amplitude and regularity and smaller TSLOW and postictal amplitude) in responders as compared with nonresponders. This effect was significant only for postictal amplitude (
F=5.12,
P=0.02), and there was a trend for greater early amplitude in responders (
F=2.69,
P=0.10).
An Ictal EEG Model of Therapeutic Response at Treatment 6
First, the ictal EEG variables that best predicted a change in seizure threshold were used to develop models that predicted therapeutic response at treatment 6. For UL ECT, age, gender, and treatment 5 ictal EEG data principal components 1, 4, and 5 (see
Table 4) were entered into a logistic regression model of dichotomous response at treatment 6. Only principal component 1 (χ
2=5.42,
P=0.02) and gender (χ
2=5.39,
P=0.02) were significantly related to therapeutic response and contributed significantly to the model. When tested with the “leave-one-out” procedure, the model was associated with a 70% accuracy in predicting dichotomous therapeutic response, with an associated sensitivity of 67% (10/15) and specificity of 72% (13/18) for detecting nonresponders.
A multivariate linear regression model of MADRS score at treatment 6 was also developed with these three principal components. Age, gender, and baseline MADRS score were also included in the model. Once again, only the first principal component of the EEG data significantly contributed to this model (see
Table 4), along with baseline MADRS (
R2=0.10,
F=5.0,
P=0.033). Principal component 1 accounted for 18.3% of the variance in treatment 6 MADRS (
R2=0.183,
F=6.9,
P=0.013). The weightings of principal component 1 in both of the logistic and linear regression models were such that ictal EEG evidence of greater seizure intensity for all 5 ictal EEG variables was associated with a greater likelihood of predicting therapeutic response.
We also explored whether ictal EEG principal components other than those that were significantly related to rise in threshold (components 1, 4, and 5 out of 5 possible principal components) might explain additional variance in therapeutic response. Principal components 2 and 3 were added stepwise to the logistic regression model of CGI-based dichotomous therapeutic response and to the multiple regression model of MADRS score at treatment 6 described above. Neither of these components significantly contributed to the logistic regression model; however, principal component 3 contributed significantly to the model of MADRS score including principal component 1 and baseline MADRS score. This component accounted for an additional 13% of the variance in MADRS score (R2=0.13, F=5.8, P=0.023); as a result, a model of MADRS score including baseline MADRS (R2=0.10) and principal component 1 (R2=0.183) accounted for a total of 41.5% of the variance (R2=0.415) in MADRS score at treatment 6. This additional contribution of principal component 3 is consistent with the finding of significantly smaller postictal amplitude and a trend for greater early amplitude in therapeutic responders as compared with nonresponders, since principal component 3 weights those two variables highly (weighting for postictal amplitude=0.52401; weighting for early amplitude=–0.514666).
Models of therapeutic response on the basis of the principal components of difference between treatment 2 and treatment 5 ictal EEG data and both gender and age were also developed; however, the principal components of the ictal EEG variables did not contribute significantly to either model.
DISCUSSION
This study is the first to demonstrate that decreases in relative stimulus intensity occurring over the treatment course with UL ECT (as a result of rises in the seizure threshold not accompanied by increases in absolute stimulus intensity) are associated with decreased therapeutic potency. An effect on therapeutic response was seen even though the change in relative stimulus intensity was smaller than those in previous studies reporting that differences in relative stimulus intensity affect therapeutic outcome, particularly for UL ECT.
1–3 The magnitude of the differences in seizure threshold seen in the present study (40%) is in agreement with what has been previously reported at this point in the treatment course,
4,5,7 as is the finding that older subjects were more likely to have a seizure threshold rise.
5,7 (The subjects in the present study are a subset of those in Coffey et al.
7)
The present results do not contrast with previous reports suggesting that rises in the seizure threshold are associated with a good therapeutic response
4,9 or are unrelated to therapeutic response,
7–9 since these other investigations either studied BL ECT
9 or were designed to maintain a constant relative stimulus intensity in the face of changes in the seizure threshold. Instead, we hypothesize that rises in threshold may have two distinct and opposite relationships to therapeutic outcome. First, the positive relationship between rises in threshold and therapeutic benefit reported in some studies suggests that such rises may in themselves be a marker of a physiologic change taking place in the brain that is necessary for therapeutic benefit with ECT, such as the activation of endogenous anticonvulsant processes.
4 On the other hand, rises in seizure threshold with UL ECT that are not accompanied by increased absolute stimulus intensity also act to decrease the relative stimulus intensity of UL ECT and thereby diminish treatment therapeutic effectiveness
2.
The evidence that these rises in the seizure threshold may be associated with diminished therapeutic potency of UL ECT suggests that it will be important to detect and adjust for such changes in the clinical setting. As mentioned previously, since it is impractical to perform repeated seizure threshold titrations and since the exclusive use of BL ECT or maximal intensity UL ECT is associated with increased cognitive side effects,
1,2,6,10–12 it is particularly important to develop a method for estimation of the seizure threshold throughout the course. In this regard, the present study provides evidence that a rise in the seizure threshold is associated with ictal EEG evidence of decreased seizure “intensity” (lower ictal amplitude and regularity, and greater postictal amplitude and time to onset of slowing).
These findings are in agreement with previous ictal EEG studies of UL ECT demonstrating that barely suprathreshold ECT was associated with evidence of decreased seizure intensity in these same variables compared with moderately suprathreshold ECT (125% and 150% of seizure threshold).
3,13,15 This study further suggests that such ictal EEG changes are detectable when the differences in seizure threshold are smaller (generally 50% changes were seen in this clinical study, compared with differences with UL ECT of 125% to 150% studied earlier in research populations). Further, because decreases in relative stimulus intensity at the end of the treatment course are likely to be even larger than those seen here, the magnitude of such ictal EEG effects may even be greater at that point.
The fact that increases in the seizure threshold occurring over the UL ECT course are accompanied by ictal EEG evidence of decreased seizure intensity is further evidence of an anticonvulsant effect of ECT, possibly mediated by increases in GABA activity, as has been proposed.
25 Although these changes have been hypothesized to be involved in the mechanism of action of ECT, the present study suggests that when they diminish the intensity of UL ECT seizures, they may result in a decrease in treatment therapeutic potency. We have also previously found evidence of a decrease in seizure intensity in the ictal EEG over the treatment course for UL ECT when there is no change in relative stimulus intensity, but the relationship of this finding to therapeutic outcome could not be determined.
26 Further work is needed to determine whether ictal EEG evidence of an anticonvulsant effect that does
not diminish UL ECT relative stimulus intensity is associated with the therapeutic response to ECT.
In contrast to these UL ECT findings, ictal EEG evidence of decreased seizure intensity did not accompany rises in the seizure threshold for BL ECT. Still, the present findings must be viewed as preliminary because of the small number of subjects studied who received BL ECT.
The UL ECT findings must also be considered in the context of the limitations of the procedure used to determine the seizure threshold.
5 The accuracy of seizure threshold determinations is constrained by the 50% increments in charge that were employed. Further, available evidence suggests that this procedure likely overestimated the seizure threshold in approximately half of the subjects.
5 Additional studies are needed to confirm these findings using a lower initial stimulus intensity and smaller dosing increments.
In terms of applying this information in the clinical setting, we developed multivariate logistic regression models of when a rise in seizure threshold has taken place, using manually rated ictal EEG variables. A model including three principal components (components 1, 4, and 5) of treatment 5 ictal EEG variables and gender was associated with a predictive accuracy of 82% for identifying when a rise in threshold has taken place at treatment 6 (88% sensitivity, 78% specificity). The ictal EEG variable that contributed most strongly to this model was midictal amplitude, though for all variables ictal EEG evidence of diminished seizure intensity tended to be associated with a higher likelihood of a rise in seizure threshold. A within-subjects model was also developed using the difference in ictal EEG indices at treatments 2 and 5, as well as age and gender. This model also weighted midictal amplitude most heavily, so that decreases in EEG amplitude at treatment 5 compared with treatment 2 were associated with a greater likelihood of a rise in seizure threshold. This model was associated with an 80% predictive accuracy.
Used in a clinical setting, such EEG models could allow practitioners to maintain a desired relative stimulus intensity by determining when changes in threshold have taken place, allowing the stimulus intensity to be adjusted accordingly. The model based on the differences between treatments 2 and 5 is the first such model based on a within-subjects approach, which has the advantage of diminishing intersubject variability in the ictal EEG.
6The variables that best predicted a rise in threshold were also used to develop models of therapeutic response. Significant relationships between treatment 5 ictal EEG variables and therapeutic response were found, but there did not appear to be a relationship between therapeutic response and the difference between treatment 2 and 5 EEG data. Ictal EEG evidence of greater seizure intensity for all treatment 5 ictal EEG variables studied tended to be associated with a greater likelihood of a good therapeutic response on both a dichotomous CGI-based outcome rating scale and a continuous MADRS rating at treatment 6. A multivariate logistic regression model including principal component 1 for treatment 5 ictal EEG data and gender was associated with an expected correct therapeutic response prediction rate of 70% at treatment 6. The same variable was significantly related to treatment 6 MADRS score, and the addition of principal component 3 resulted in a multivariate linear regression model that accounted for 41.5% of the variance in MADRS score. These analyses indicated that greater early and midictal amplitude and postictal suppression were associated with a better therapeutic response, and thus they are in agreement with a previous report of a significant relationship between these same ictal EEG variables and therapeutic response at treatment 6 in one study employing computer EEG analysis
3 and two reports of manual ratings of greater ictal EEG postictal suppression in ECT responders.
16,27The same combination of ictal EEG variables (principal component 1) was a significant predictor of both a rise in seizure threshold and therapeutic response. This finding supports the potential utility of those ictal EEG indices in the clinical setting. This evidence suggests that such indices would be able to detect changes in the seizure threshold that occurred over the treatment course and allow stimulus intensity adjustments to be made accordingly. It also suggests that adjustments made on that basis may improve the therapeutic effectiveness of ECT.
In summary, these findings indicate that increases in seizure threshold occurring clinically over the treatment course are associated with ictal EEG evidence of diminished seizure intensity and that they affect the therapeutic response to ECT. Ictal EEG models are able to detect such changes as well as reflect therapeutic potency. Thus, ictal EEG indices have considerable potential as a means to maintain seizure adequacy in the clinical setting.