Risperidone for the Treatment of Behavioral Disturbances in Dementia: A Case Series
Abstract
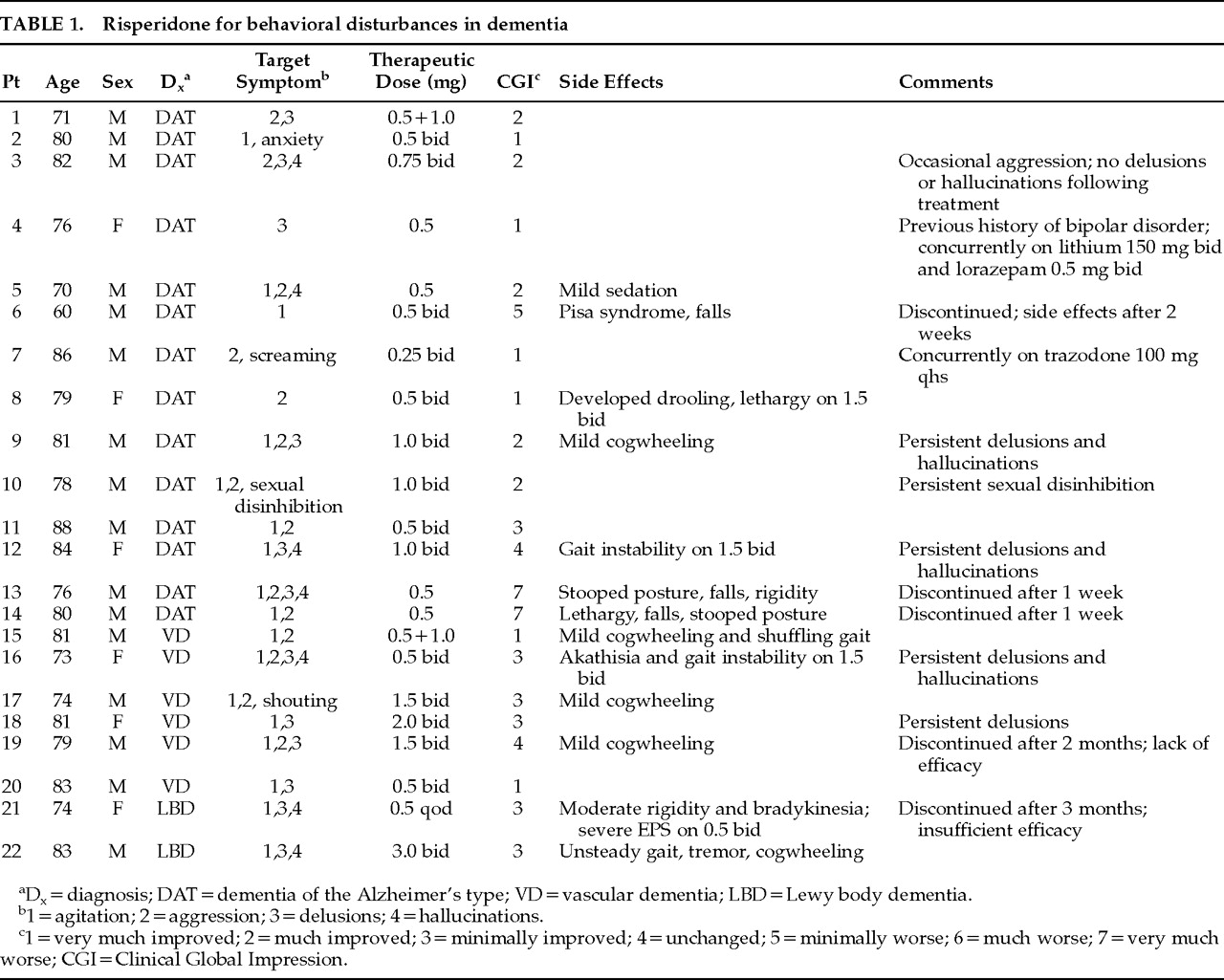
PATIENTS
RESULTS
Case Report
Patient 8. This 79-year-old woman was a resident in a long-term care facility. She was diagnosed as having dementia of the Alzheimer's type, Global Deterioration Scale (GDS)4 stage 6–7. Other than a history of syncope and a fractured ankle, she was medically well. She was extremely resistant to care and physically aggressive toward staff and co-residents. She would wander and make numerous attempts to leave the facility, often pulling other residents with her. Even though she had not been treated previously with a neuroleptic, her family chose treatment with risperidone as a first-line agent because of their concerns about side effects of neuroleptics. She was started on risperidone 0.25 mg bid and slowly increased to 1.5 mg bid. Behavior improved significantly. She was no longer aggressive, and staff were able to bathe and shower her with much less agitation. Over a period of 1 month on 1.5 mg bid, however, she became lethargic and would drool. Risperidone was reduced to 0.5 mg bid, with resolution of these side effects. Overall outcome was assessed as very much improved over 10 months of ongoing therapy.
Patient 20. This 83-year-old man was a resident in a long-term care facility. He was diagnosed as having vascular dementia and scored 15/30 on the Mini-Mental State Examination.5 His medical history included carcinoma of the lung, coronary artery disease, and atrial fibrillation. His only concurrent medication was digoxin. He had marked persecutory delusions of people trying to steal his belongings and attempting to harm him. These resulted in ongoing agitation manifested by repeated perseverative complaints, calling out for help, restlessness, and anxiety, which made it difficult for staff to give him care. He was previously treated with haloperidol, methotrimeprazine, and lorazepam, all of which were ineffective. He was treated with risperidone 0.5 mg bid and showed a marked decrease in delusions, agitation, calling out, restlessness, and anxiety, allowing staff to manage him quite easily. No EPS were noted, and he was assessed as being very much improved over the course of his 6-month trial.
Patient 22. This 83-year-old man was admitted to an acute psychogeriatric unit for marked delusions, hallucinations, and agitation. He was diagnosed as having dementia and fulfilled consensus guidelines for the clinical diagnosis of dementia with Lewy bodies.2 He was terrified that the Mafia was trying to kill him, and he was constantly responding to auditory hallucinations of voices telling him they were “coming to get him.” He would barricade his room at night and would not sleep for fear of being killed. Because of his distress, he was treated with loxapine in increasing doses of up to 20 mg per day. His delusions and hallucinations slowly decreased, but he experienced severe tremor, akinesia, and several falls. A brief trial of clozapine 6.25 mg was discontinued because of excessive sedation. He was started on risperidone 0.5 mg. On low doses of risperidone he had no EPS, and there was a diminution of his agitation, as evidenced by a decrease in restlessness and calling out and fewer attempts to leave the unit. His delusions and hallucinations, however, persisted. As a result, risperidone was increased slowly to a maximum of 3 mg po bid. At this dosage there was no further improvement in the psychosis, but there was an increase in EPS, including tremor, rabbit syndrome, and bradykinesia. The risperidone was discontinued after a 3-month trial as a result of lack of sufficient efficacy rather than side effects. He was assessed as being minimally improved in view of the decrease in his agitation.
Patient 14. This 80-year-old man was a resident in a long-term care facility. He was diagnosed as having dementia of the Alzheimer's type, GDS stage 6. He had a history of hypertension and B12 deficiency but was on no medications other than monthly B12 injections. He was very aggressive with staff and had injured several nurses by punching and kicking them during care. Agitation was manifested by constant pacing, restlessness, and negativism. He had several unsuccessful trials of medications, including lorazepam 0.5 mg prn (ineffective), trazodone 50 mg po qhs (excessive daytime sedation), chlorpromazine 10 mg bid (excessive sedation), and loxapine 5 mg (marked rigidity and bradykinesia). He was started on risperidone 0.5 mg, and within several days he was overly sedated, was no longer able to feed himself, and could no longer walk because of gait instability and markedly stooped posture. The risperidone was discontinued, and he improved to baseline within 3 days.
DISCUSSION
References
Information & Authors
Information
Published In

History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
There are no citations for this item
View Options
View options
PDF/ePub
View PDF/ePubGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).