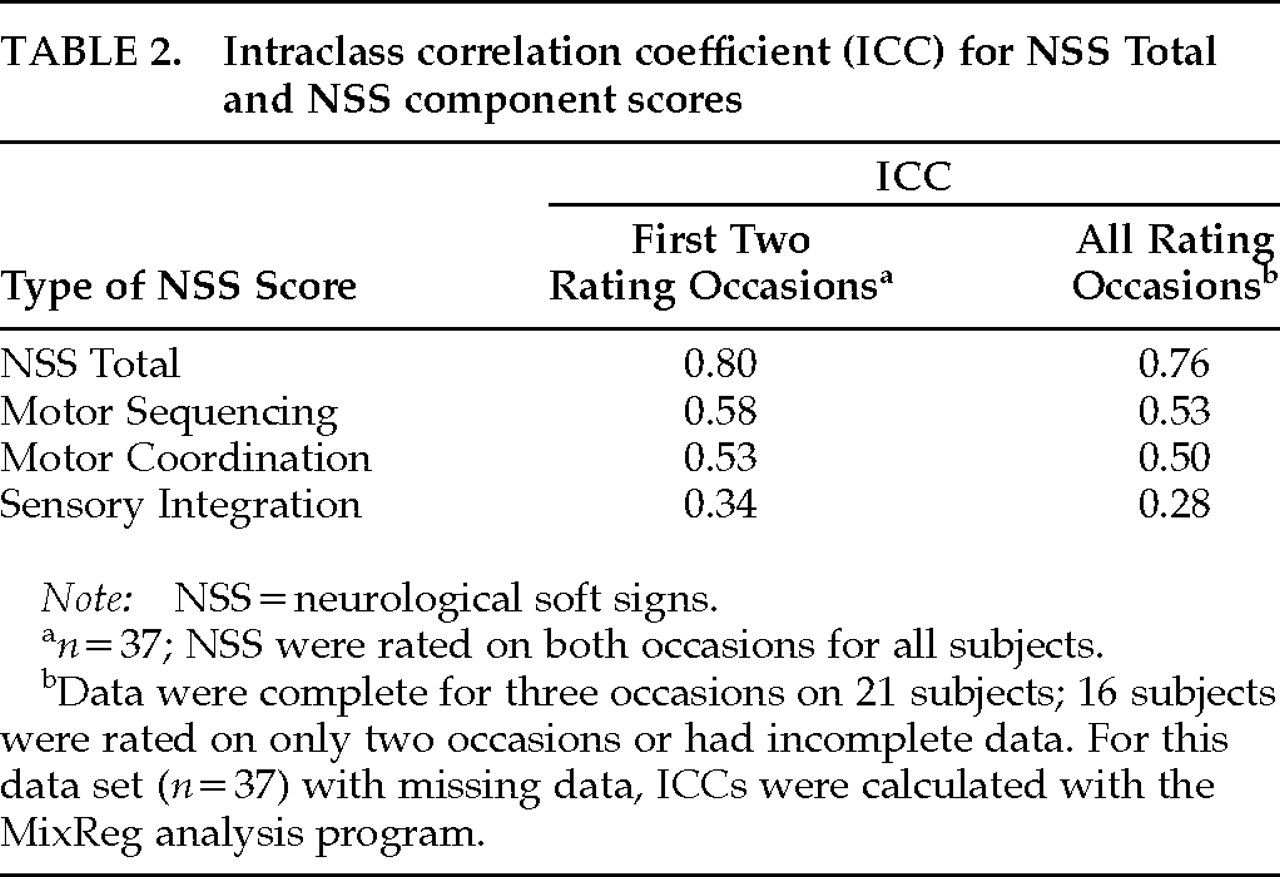
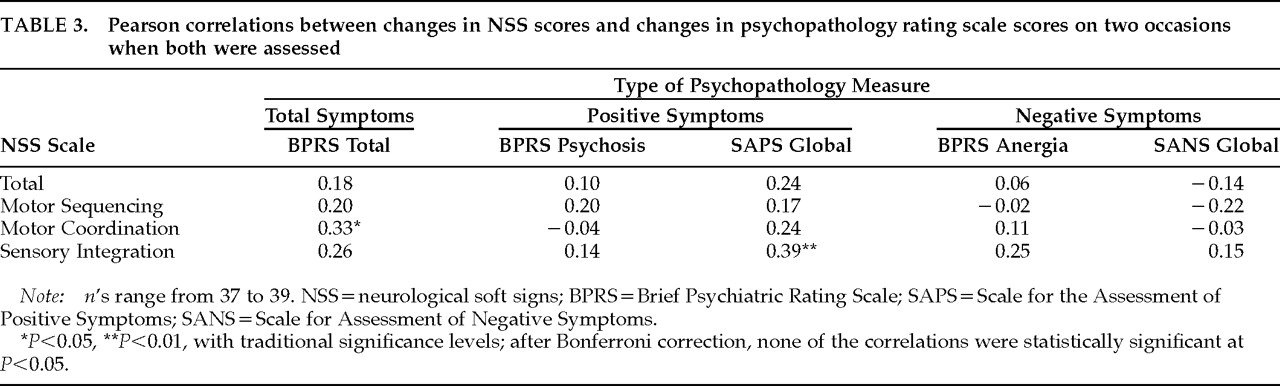
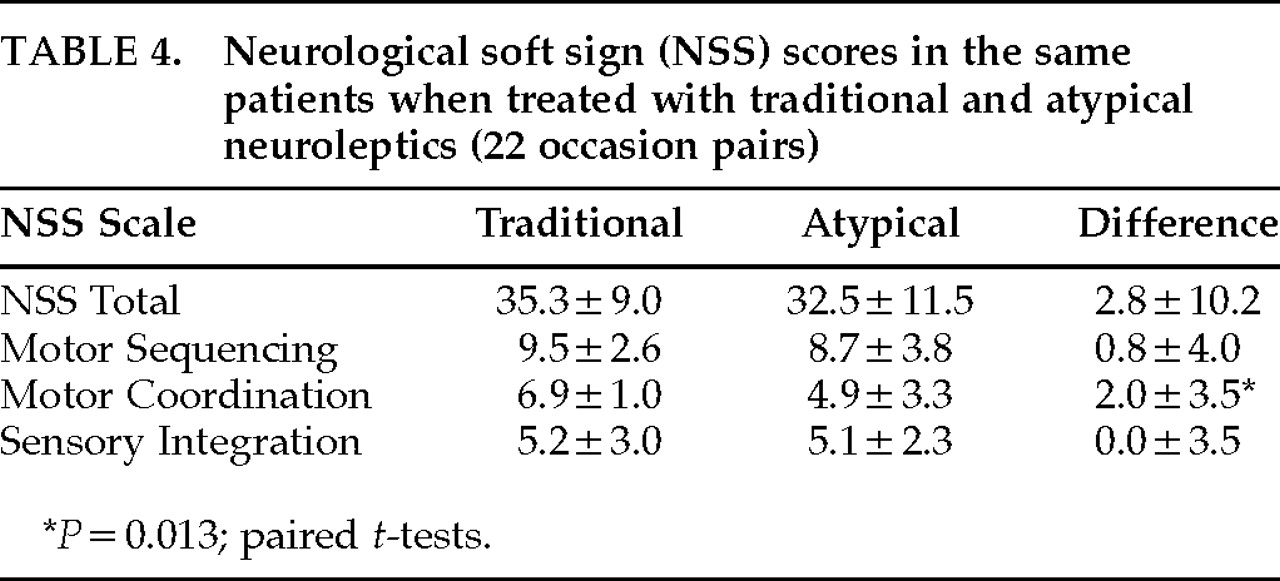
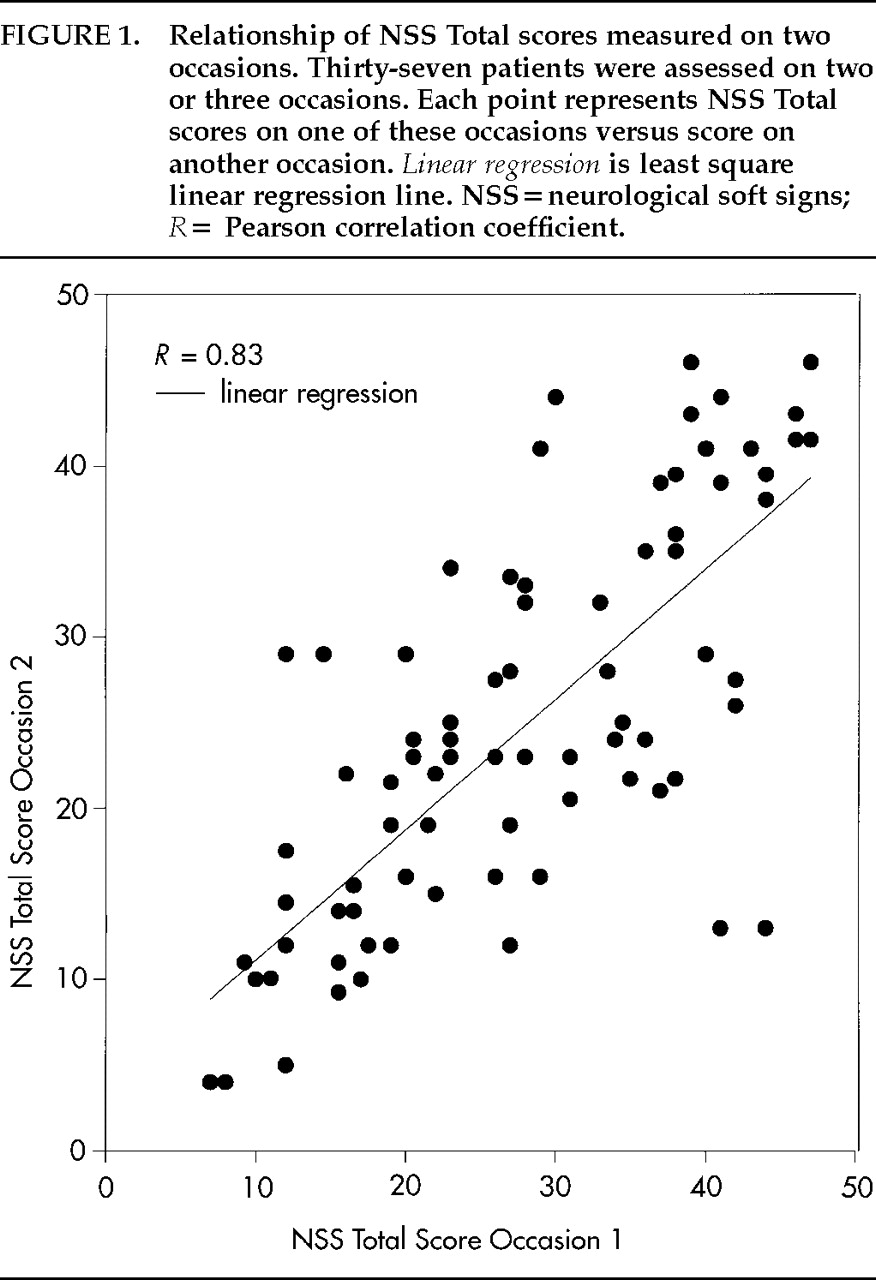
NSS Total scores showed relatively high stability over time (as indicated by ICCs and correlation coefficients), and changes in these scores were not related to time between ratings, changes in psychopathology scores, or neuroleptic drug treatments. These findings support the idea that this measure may be relatively stable in chronically hospitalized schizophrenic patients and has some properties of a trait-like characteristic. This hypothesis agrees with the findings or suggestions of some other investigators.
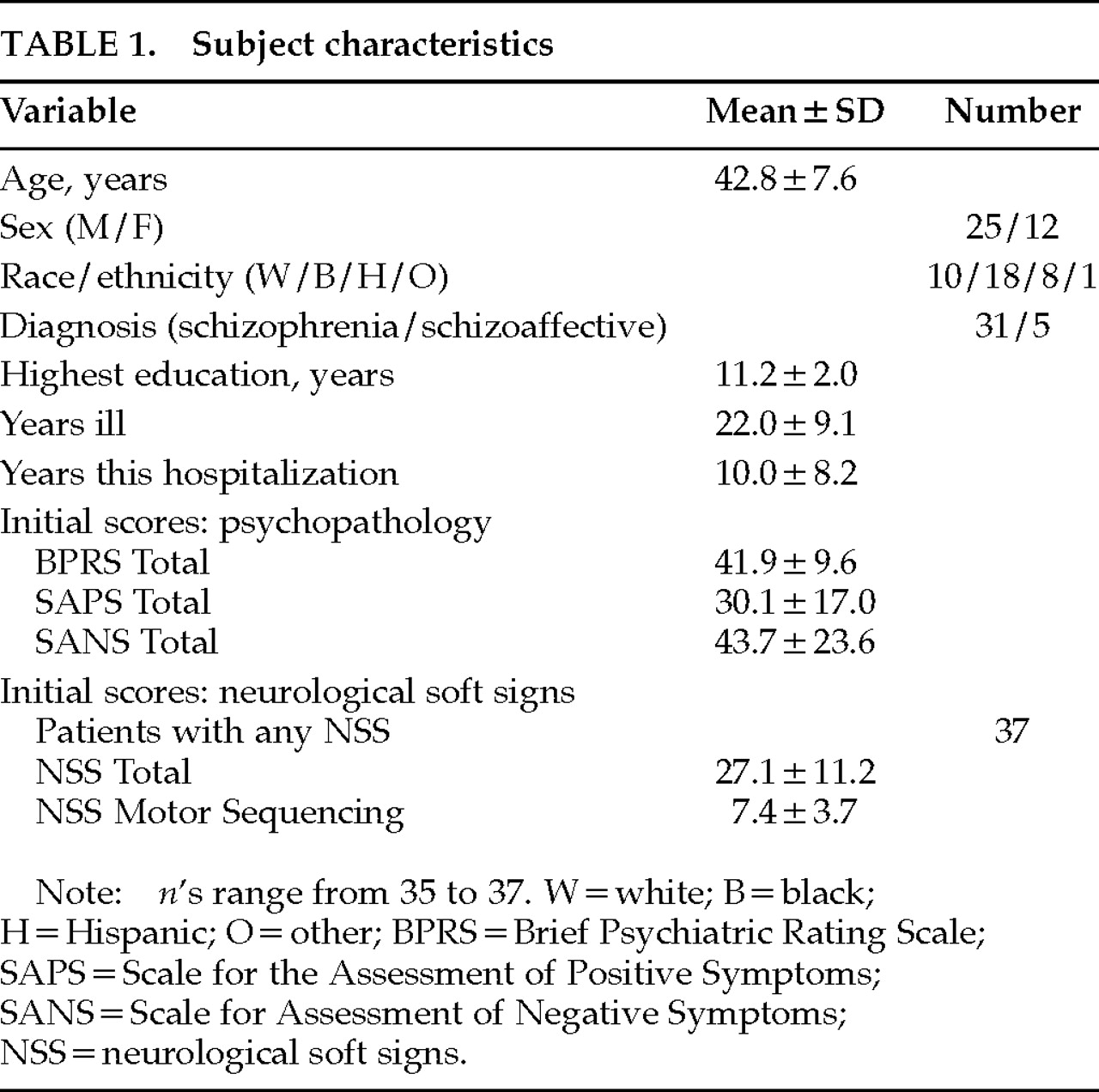
1,5 The NSS Total scores did not increase in severity over several years and did not significantly correlate with length of illness, suggesting that they were not progressive over the time period of the illness we evaluated. We were not able to study our patients early in their illness or compare neurological signs they currently had with those in their first or second hospitalization. It is possible that neurological signs have a more variable picture or progressive course in acute schizophrenic patients, earlier in the course of the illness, or in less chronically ill schizophrenic patients, as suggested by reports of two other investigations.
6,7Some studies have reported a high correlation of tardive dyskinesia (TD) and NSS scores,
15 but this has not been universally found.
16 Although most of our patients did not have prominent signs of tardive dyskinesia, we did not serially assess with the Abnormal Involuntary Movement Scale or another tardive dyskinesia measure. If NSS and TD scores were highly correlated and covaried consistently in our sample, this might present a confounding factor in the interpretation of the substantive significance of the stability of NSS total scores over time.
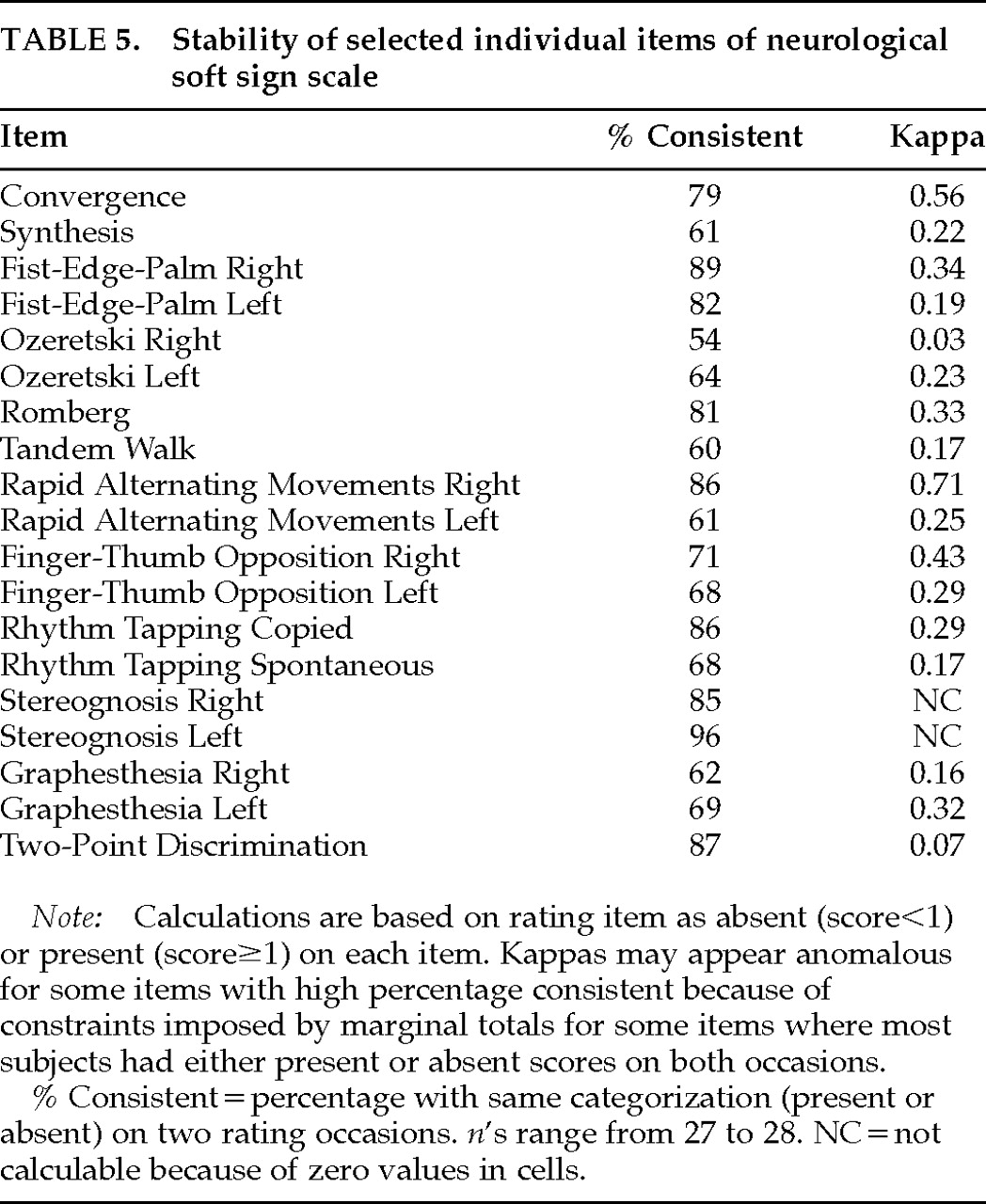
Our findings that motor sequencing and motor coordination scores showed only moderate stability, and sensory integration fairly low stability, over time suggest that NSS Total scores are a preferable measure to choose for correlational studies of long-term clinical response or other trait-like characteristics. Since individual signs showed considerable variability in their stability, they should not be relied on in predictive or correlational studies. The lower stability of many individual signs is consistent with a preliminary meeting poster on NSS item stability presented by Sanders and associates.
17An ideal trait-like characteristic would show high stability not only in total score but also in individual component subscores and item scores. Since we did not find this to be the case, it makes the interpretation of NSS as a classical trait-like characteristic more ambiguous. Although component subscores showed the same pattern of correlations with dependent variables (psychopathology scores, time between ratings) as did total score, their within-subject stability across time, as indicated by Pearson and intraclass correlation coefficients, was lower. If the subscores were uncorrelated or weakly correlated with NSS Total scores, they might represent independent factors. This might help explain the differences in stability of NSS Total and component scores across time. The psychometric properties of the NSS scale have not been extensively investigated. Whether the component subscores represent consistent independent entities is unclear. Buchanan and Heinrichs
8 reported that NSS Total scores for their scale were significantly correlated with component subscores in schizophrenic patients (
r 0.57–0.69,
P<0.01). However, they found considerably smaller correlations among the different NSS component scores themselves (
r 0.26–0.31). In our sample of chronically hospitalized schizophrenic patients, NSS Total scores were also highly correlated with the three component subscores (
r=0.62–0.88,
P<0.001). However, contrary to the findings of Buchanan and Heinrichs, NSS motor sequencing and motor coordination subscores also showed fairly high correlations (
r 0.64–0.72,
P<0.001); sensory integration scores showed a lower correlation with the other NSS component scores (
r 0.28–0.46,
P range 0.11–0.015). These correlations suggest that some of the component scores may not represent statistically independent factors in our patients, although a formal factor analysis scale has not been performed. Therefore, the explanation of the differences in the stability of the component scores on the basis of “independent factors” is less plausible. Alternatively, the correlations between different subscores may represent a functional interdependence between different brain areas. It is possible that the deficits represented by high neurological soft sign scores in chronic schizophrenic patients are not localized to a single brain region, but rather may represent a more general problem in interneuronal signaling. Even though patients may exhibit variable severity in specific expressions of motor or cognitive-motor function at different times, the total extent of the deficit, represented by NSS Total score, remains fairly constant. Longitudinal research of NSS over the developmental course of patients with schizophrenia who become chronically hospitalized may provide evidence to support this interpretation.